
Case Report | DOI: https://doi.org/10.31579/2692-9406/083
*Corresponding Author: Anil Kumar Sakalecha, Department of Radio-Diagnosis, Sri Devaraj Urs Academy of Higher Education & Research, Tamaka, Kolar, Karnataka.
Citation: Parameshwar Keerthi B H, Anil K Sakalecha, Varun S, Shivaprasad G Savagave. (2021). Re-Print: An Interesting Case of Disseminated Tuberculoma of Brain and Spinal Cord Type of Study: Case Report. Biomedical Research and Clinical Reviews. 5(1); DOI: 10.31579/2692-9406/083.
Copyright: © 2021 Anil Kumar Sakalecha, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 24 August 2021 | Accepted: 22 September 2021 | Published: 01 October 2021
Keywords: tuberculosis; CNS; tuberculoma; ring enhancing lesion; MRI
Tuberculosis is an important public problem worldwide from 19th century. Manifestations of tuberculosis widely classified as pulmonary and extra pulmonary manifestations. Central nervous system (CNS) tuberculosis is a serious condition where patients most often present with seizure. Tuberculoma is one of the CNS manifestations of tuberculosis. The imaging feature of tuberculoma is ring enhancing lesions. Tuberculoma should be differentiated from other diseases with ring enhancing lesions like neurocysticercosis, coccidiomycosis, toxoplasmosis and malignancies.
Tuberculoma of brain is an important manifestation of CNS tuberculosis. It constitutes approximately 5% of overall extra pulmonary manifestation of tuberculosis [1]. Spinal tuberculoma on other hand is extremely a rare manifestation occurring at the frequency of 1 in 50,000 individuals. It constitutes only 2% of CNS tuberculosis [2].
Tuberculosis (TB) is a great threat in developing countries with 8.6 million new cases and 1.3 million deaths worldwide in 2012. It is a disease of poverty affecting most of the underdeveloped and developing countires [3]. In India prevalence of tuberculosis is approximately 1.8 million cases per year [4].
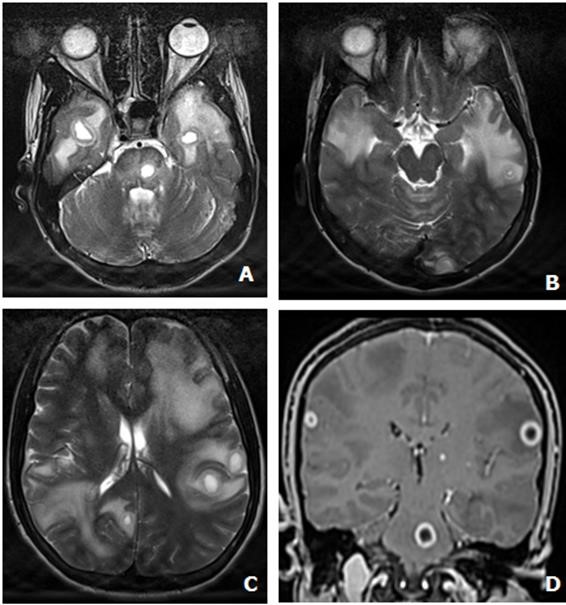
30 Y/M, a known case of tuberculosis on ATT for 3 months presented with history of weakness of both lower limbs. 1.5 Tesla MRI scanner (SIEMENS® MAGNETOM AVANTO) was used for diagnosis.
Multifocal, well-defined, variable sized, rounded and ovoid, thick walled solid and cystic lesions with diffuse perilesional edema in bilateral cerebral and cerebellar hemispheres, predominantly at grey-white matter junctions, left pons, cerebellar vermis, cervical and thoracic segment of spinal cord at the level of C4 and D11 vertebral levels. Few of the lesions revealed internal T2 hyperintense signal– suggestive of liquefaction. Few of the lesions revealed central T2 hypointense signal– suggestive of caseation. On post-contrast study, the liquefactive lesions demonstrated smooth ring enhancement. Solid lesions demonstrated homogeneous enhancement. Diffuse cerebral edema noted in the form of effacement of sylvian fissure and cortical sulci. On MR-Spectroscopy elevated lipid peak (1.3 ppm), mildly reduced NAA (3.2 ppm), reduced NAA/Cho ratio were seen. All vertebrae were normal.
Above imaging features were suggestive of disseminated central nervous tuberculoma.


Central nervous system (CNS) tuberculosis is a life threatening and devastating condition which is curable when diagnosed in early stages. Imaging manifestations of CNS tuberculosis are meningitis, tuberculoma, miliary tuberculosis, abscess, cerebritis, and encephalopathy. Tuberculoma is the most common parenchymal lesion in CNS tuberculosis which could be found in any portion of the intracranial space. The lesion may be solitary or multiple and may be seen with or without meningitis [5].
Most common clinical findings in CNS tuberculosis encountered is seizure followed by meningitis. Other manifestations include focal neurological deficits, behavioural changes, and altered sensorium [6].
Mode of spread for spinal tuberculoma is CSF spread, haematogenous spread or local spread from spinal tuberculosis. In our case spinal tuberculoma was associated with pulmonary tuberculosis. It is important to look for pulmonary tuberculosis in patients with spinal intramedullary tuberculomas. Lu M et al in his study also showed a positive association between spinal tuberculoma and pulmonary tuberculosis [7].
On MRI, the lesions are classified as non caseating granuloma, caseating granuloma, caseating granuloma with central liquefaction and calcified granuloma. Non caseating granuloma are iso-to-hypointense on T1, hyperintense on T2 weighted image with homogeneous enhancement on post contrast image. Caseating granuloma are hypointense on both T1 and T2 weighted image with hyperintense rim on T1 weighted image and homogeneous or ring enhancement on post contrast enhancement. Caseating granuloma with liquefaction are iso-to-hypointense lesion with peripheral hyperintense rim and hypointense with central hyperintensity on T2 weighted image with ring enhancement on post contrast image. Calcified granuloma are hypointense on T1 and T2 weighted image with no significant enhancement on post contrast study.
ATT treatment include isoniazid (INH) 300 mg/day, rifampicin (RF) 450 mg/day, pyrazinamide 1500 mg/day, and ethambutol 800 mg/day daily for 2 months, followed by INH and RF for 4 months. Pyridoxine at 40 mg/day was given for all 6 months. Prednisolone at 1 mg/kg body weight was given for 1 month and then subsequently tapered over a period of 1 month. Follow up MRI imaging should be performed to look for the reduction in the size of the lesion. Pulmonary CT should also be performed to look for the regression of the lesions.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
