
Research Article | DOI: https://doi.org/10.31579/2641-0419/050
*Corresponding Author: Gary L. Murray, The Heart and Vascular Institute, Germantown TN- USA
Citation: Gary L. Murray, Colombo J (2020) (r) Alpha Lipoic Acid Is a Safe, Effective Pharmacologic Therapy of Chronic Orthostatic Hypotension Associated with Low Sympathetic Tone. J. Clinical Cardiology and Cardiovascular Interventions, 3(4); Doi:10.31579/2641-0419/050
Copyright: © 2020 Gary L. Murray. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 February 2020 | Accepted: 04 March 2020 | Published: 10 March 2020
Keywords: α-lipoic acid, orthostatic hypotension, autonomic nervous system, parasympathetic nervous system,sympathetic nervous system
Abstract
Chronic orthostatic hypotension (OH), affecting 10 to 30% of the elderly, is associated with falls, and increased morbidity and mortality. Current pharmacologic therapy can cause or worsen hypertension and fluid retention. (r) α lipoic acid (ALA), a powerful natural antioxidant, avoids those complications and may assist management ofchronic neurogenic orthostatic hypotension (NOH). The purpose of this study is to demonstrate improvement in the symptoms of orthostatic dysfunction with r-ALA, including improved sympathetic (S) and blood pressure (BP) responses to head-up postural change (standing).
A cohort of 109 patients with low S tone upon standing was detected using the ANX —3.0, Autonomic Monitor, ANSAR Medical Technologies, Inc., Philadelphia, PA. From the cohort, 29patients demonstrated NOH (change in (Δ) standing BP ≤ —20/–10 mm Hg) and 60 patients demonstrated orthostatic intolerance (OI, Δ standing systolic BP between –6 and –19 mm Hg). These 89 were given ALA orally: either 590 to 788 mg (r) ALA or 867 to 1,500 mg of the less expensive 50 to 50% mixture (r) ALA and inactive (s) ALA. Changes in their S- and P tone, and BPs, were compared with 20 control patients during mean follow-up of 2.28 years.
Nineteen of 29 (66%) NOH patients responded with a Δ standing BP from –28/–6 mm Hg to 0/þ2 mm Hg. Forty of 60 (67%) of patients with OI responded with a Δ standing BP of –9/þ1 mm Hg to þ6/þ2 mm Hg. Although all patients treated with ALA increased S tone, the Δ BP depended upon the pretreatment of S tone. Those with the lowest S tone responded the least well. The only treatment side effects were nausea, intolerable in only 5%. Nausea improved with routine gastrointestinal medica- tions. Glucose levels improved in the 28% of patients who were diabetic. Also, resting hypertension improved. Control patients had no Δ BP and no increase in S tone. (r)ALA improves S-, and BP, responses to head-up postural change, and thereby NOH/OI, in a majority of patients without causing harmful side effects.
Chronic orthostatic hypotension (OH, defined as fall of systolic blood pressure [BP] or diastolic BP ≤ 20/10 mm Hg within 3 minutes of standing still) isprevalent atany age, but mostly in the elderly1 in whom neurogenic orthostatic hypotension (NOH [such as low sympathetic (S) tone
with head-up postural change (i.e., standing)]) is by far more common than venostasis or iatrogeniccauses, with OH prevalence rates up to 30%.2 OH is a common cause of lightheadedness in elderly or chronic disease patients and is one of the earliest, and arguably the most debilitating, symptom of autonomic dysfunction.[3,4] OH is associated with increased mortality in the elderly: hazard ratios of systolic BP OH: 1.69 to 2.04; diastolic BP OH: 2.2. [5] OH in diabetics can be an early manifestation of cardiac autonomicneuropathy, and possibly in nondiabetics and the elderly. Cardiac autonomic neuropathy increases mortality by 25 to 50% within 10 years, [6] and heart failure death or hospitalization is also high (hazard ratio 1.85).[7] Oxidative stress, regardless of the source (sugar acidosis, low antiox- idant levels, psychosocial stress, lack of exercise, smoking, pollution, etc.), causes autonomic injury that precedes dia-betic autonomic neuropathy. Autonomic injury affects all systems of the body. Oxidative and nitrosative stress damages the more sensitive tissues, including peripheral and central nerves, endothelial cells, immune cells, the microvasculature, and glomerular filtration structures. Therapies known to reduce oxidative stress are therefore recommended. α-lipoic acid (ALA), through its multiple antioxidant properties, has long been found to slow or stay the progression of autonomic injury.[8,9]
The autonomic nervous system plays a critical role in BP regulation. [10] Since (r) ALA has been used in treating diabetic cardiac autonomic neuropathy, including orthostatic dys- function and hypertension, [11–14] we postulated it might improve NOH as well as orthostatic intolerance (OI) in nondiabetics, without causing or worsening hypertension or volume overload; as do most frequently used pharmaco- logic agents. [15]
As human longevity increases worldwide, OH will become increasingly problematic. Presently, most types of OH are treated similarly. Medications with hypotensive side effects are reduced or discontinued, compression hose for lower extremityedema, and occasional abdominal binders to increase venous return, fludrocortisone, increased oral fluid and salt intake to increase plasma volume, midodrine for vasoconstric- tion, and most recently droxidopa to increase norepinephrine levels. [16] Other medications are uncommonly used. [17,18] How-ever, many of these measures can cause or exacerbate pre- existing hypertension, or worsen congestive heart failure. Clearly, much more efficacious treatment is needed.
ALA is a naturally occurring substance, a powerful thiol antioxidant that restores and recycles vitamins A, C, E, and glutathione, enhancing their efficacy. ALA also improves hyperglycemia, endothelial dysfunction, nitric oxide levels; reduces nuclear factor kappa B activity, is essential for the function of certain oxidative enzymatic activities; and has been mainly used to treat diabetic dysautonomia. [19] It also suppresses neurologic intracellular accumulation of α-synu- clein, the major cause of NOH in many neurologic dis- eases.[20,21] It exists as two enantiomers, with (r)ALA much more active than (s)ALA, and does not require a prescription. ALA treatment seems safe and effective (without hyperten-sive side effects or volume overload) for NOH or OI patients, even in nondiabetics. The purpose of this study is to demon- strate improvement in the symptoms of orthostatic dysfunc- tion with r-ALA, including improved S and BP responses to head-up postural change (standing).
Using the ANX-3.0 Autonomic Monitor (ANSAR Medical Tech- nologies, Inc., Philadelphia, PA), sympathetic- (S) and para- sympathetic (P)-activity were computed simultaneously and independently based on concurrent, continuous, time fre- quency analysis of respiratory activity, and heart rate varia-bility.[22–27] P activity measured as the respiratory frequency area (RFa) is defined as the spectral power within a 0.10 Hz- wide window centered on the fundamental respiratory fre- quency in the heart rate variability spectrum. Fundamental respiratory frequency is identified as the peak spectral mode from time-frequency analysis of
respiratory activity. RFa is a measure of vagal outflow as it affects the heart. S activity (low frequency area [LFa]) is defined as the remaining spectral power in the low-frequency window (0.04–0.15 Hz) of the heart rate variability spectrum, after computation of RFa. P- and S activity was recorded from a standard autonomic test, including (1) 5 minutes rest (seated), (2) 1 minute of breathing at 6 breaths/minute, (3) a series of 5 Valsalva maneuvers, including a 15 second Valsalva maneuver, and (4) a quick stand to 5 minutes of quiet standing. The average ratio of resting S to P activity (sympathovagal balance) reported was the average of the ratios recorded during the sampling period, not the ratio of the averages. [28]
A cohort of 109 patients with low S tone upon standing was detected using the ANX -3.0, Autonomic Monitor, ANSAR Medical Technologies, Inc., Philadelphia, PA. From the cohort, 29 patients demonstrated NOH (change in (Δ) standing BP ≤ –20/–10 mm Hg) and 60 patients demonstrated ortho- static intolerance (OI, Δ standing systolic BP between –6 and–19 mm Hg). These 89 were given ALA orally: either 590 to 788 mg (r) ALA or 867 to 1500 mg of the less expensive 50 to 50% mixture (r) ALA and inactive (s) ALA. Changes in their S- and P tone, and BPs, were compared with 20 control patients during mean follow-up of 2.28 years.
All 109 study patients had low S sitting or standing. The only change in patients’ therapy was the addition of (r) ALA or ALA (a racemic mixture of (r)-and (s) ALA). Syncopal respon- ders had no recurrence of syncope, otherwise response was defined as Δ standing systolic BP < –6 mm Hg.
This study was approved by our Institutional Review Board, and all patients signed informed consent.
Continuous data were assessed for normality with normally distributed data analyzed using Student t-tests and non-nor- mally distributed data using a Mann–Whitney U test. Dichot- omous data were analyzed using the chi-square test or Fisher’s exact test. A p-value of ≤ 0.05 was considered significant. Student t-tests were performed as two-tailed with equal variance. Significance values were determined on the null hypothesis that the pre- and post-treatment values are equal.
Patient demographics are listed in (Table 1) In the OH Group (n ¼ 29), [1] there were no females in the 10 nonresponders; [2]

there were more diabetics;80% were prescribed midodrine, fludrocortisone, or desmopressin; and [4] 20% were on beta- blockers. There were fewer patients with hypertension or congestive heart failure, but more with syncope. In the OI
group (n ¼ 60), there were fewer congestive heart failure patients, but more with syncope, fatigue, and headache.
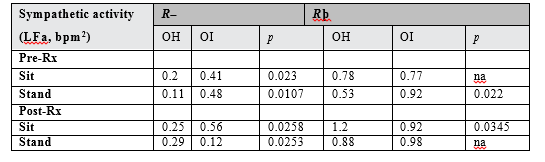
Patient autonomics and BPs are listed in (Tables 2 and 3). In the OH group, pre-and post-treatment Δ standing BP was –32/–9 mm Hg versus –29/–11 mm Hg in nonresponders, and –28/–6 mm Hg versus 0/þ2 mm Hg in responders. In the OI group, pre- and post-treatment Δ standing BP was —13/—19 mm Hg versus —12/þ2 mm Hg in nonresponders, and —9/þ1 mm Hg versus þ6/þ2 mm Hg in responders. Responders had higher S tone (Table 3). Regardless of the Δ standing BP, (r) ALA reduced sitting BP in most patients. In the controls, there was no significant difference in Δ standing BP (from a baseline of —13/—1 toa follow-up of —13/þ3), and there was a decrease in S activity with follow-up.
Discussion
NOH is caused by failure of the baroreceptor reflex and/or too low S tone, usually as a result of neurologic intracellular α- synuclein production and aggregation. [20] ALA suppresses this as an antioxidant, improving the baroreceptor reflex and Stone, in contrast to the commonly used medications, so itshould affect healing of the disorder, rather than simply treating its symptoms. Furthermore, it uniquely reduces resting hypertension and endothelial dysfunction [29,33].
Although only 28% of the patients were diabetic (Table 1), 59 of 89 (66% of all) patients responded to ALA. Sixteen of the 25 diabetics (64%) responded and 43 of 64 (67%) nondiabetics (p ¼ ns), suggesting that ALA may be equally effective for all patients with orthostatic dysfunction. Nineteen of 29 (66%) NOH and 40 of 60 (67%) OI patients responded to ALA (p ¼ ns), furthering the above suggestion. (r)ALA raised LFa (S activity) in all patients except in OI nonresponders (Table 2). Treatment Δ BP was related to pretreatment S activity. Those with the lowest sitting to stand- ing change in S activity were the nonresponders (Table 3); perhaps droxidopa would be useful in these patients.
Responders had both a decrease in mean sitting BP (145/72–125/68 mm Hg, pre- to post-(r)ALA treatment, mean dose 643 mg/d or ALA 949 mg/d), and an increase in mean standing BP (120/70–129/71 mm Hg, pre- to post- treatment). This Δ sitting BP indicates an improvement in resting hypertension and the Δ standing BP indicates an improvement in orthostatic dysfunction. OI nonresponders demonstrated a þ19 mm Hg (increase) in standing diastolic BP, which is vital in preserving coronary perfusion (Tables 1, 2). In patients with coronary artery disease, a J-curve relationship has been reported between BP and major adverse

cardiac events. [33] Given this J-curve of coronary flow and since major adverse cardiac events increase at diastolic BPs < 60 to 70 mm Hg, [33] the increase in diastolic BP in the OI nonrespon- der group could have been considered a positive OI response, but we defined a positive response as a standing decrease in only systolic BP less than —6 mm Hg, and the absence of syncope. Even though the OI nonresponders’ standing systolic BP fell 6 mm Hg or more (an average fall of 12 mm Hg, (Table 2), their diastolic BPs increased significantly (from a fall of 19 mm Hg to an increase of 2 mm Hg; p ¼ 0.0068, (Table 2). This improved outcome would raise the positive response rate to (r) ALA to 88% had we considered the J-curve of coronary perfusion, Although previous human studies of the effect of ALA upon high BP have been mixed, [34] it can reduce high BP, increase baroreceptor reflex afferent limb sensitivity, improve endothelial dysfunction, increase nitric oxide, and improve diabetic dysautonomia. In our 19 OH respon- ders, mean ΔBP to standing from pre- to post-treatment was –28/–6 mm Hg (sitting to standing, pretreatment) to 0/þ2 mm Hg (sitting to standing, post-treatment). To date, we know of no other pharmacologic treatment that both decreases resting hypertension and OH. Such treatment has the potential to reduce substantially major cardiovascular events such as stroke, congestive heart failure, myocardial infarction, and cardiovascular death (major adverse cardiac events), as well as therapeutic costs and side effects. Nausea, rare flushing, and biotin depletion are the only known side effects of (r) ALA or ALA, and are harmless and easily treatable.
In the 20 control patients, S activity decreased, although Δ BP did not, possibly because their initial S activity was the highest of all groups. Regardless, the decrease in S activity may be the prelude to further decreases in BP, if therapy is not prescribed. Since S activity controls BP and BP changes with stand (and other activities), the persistent decrease in S activity with stand indicates that there is a continued drive to further decrease BP upon standing, exacerbating orthostatic dysfunction and the associated morbidity and mortality risks. Because these untreated patients’ S activity might continue to fall, perhaps they should be started on (r) ALA or ALA.
A larger, longer study that also determines if ALA reduces major adverse cardiac events in NOH, and whether progres- sion of these conditions is slowed, is needed. Additionally, if there is a partial response to therapy, what should be done next? Certainly, adjusting other hypotensive medications without absolute indications would seem obvious. Finally, our definition of OI was arbitrary.
(r)ALA or ALA appears to safely improve NOH and OI by increasing standing S activity, as measured by LFa, and thereby standing BP responses to stand.
No funding was provided.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
