
Case Report | DOI: https://doi.org/10.31579/2690-4861/323
1 A & U Tibbia College, Karol Bagh, New Delhi.
2 Govt. Unani Medical College& Hospital, Bangalore, KA.
*Corresponding Author: Tabassum K, Govt. Unani Medical College& Hospital, Bangalore, KA.
Citation: Aysha Raza, Tabassum K., (2023), Rare Case Report of Robert Uterus with Ovarian Endometrioma, International Journal of Clinical Case Reports and Reviews, 14(2); DOI:10.31579/2690-4861/323
Copyright: © 2023, Tabassum K. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 July 2023 | Accepted: 19 July 2023 | Published: 28 July 2023
Keywords: robert uterus; septate uterus; endometrioma; dysmenorrhoea and infertility
Robert's uterus is a rare type of congenital uterine anomaly where septum divides the uterine cavity asymmetrically resulting in the formation of a noncommunicating hemiuterus. Patients may present with recurrent pain, severe dysmenorrhea, recurrent abortions, and infertility. A 25 years nulliparous female with complaint of severe dysmenorrhea without bleeding per vagina since her menarche was visited to our clinic. She attained her menarche at the age of 12 years which was followed by severe dysmenorrhea in every month. Dysmenorrhea persisted and increased in intensity gradually. She had a history of a spontaneous first trimester miscarriage, followed by secondary infertility for 3 years. She also had severe deep dyspareunia with gradually decreasing coital frequency. Since her menarche she was taking regular analgesics oral and parenteral and the frequency of same has increased in the last few years. USG showed a septate uterus with hemorrhagic collection in the left endometrial cavity linear calcifications described likely retained product of conception. MRI showed thick uterine septum completely dividing the uterine cavity asymmetrically with no communication with cervix indicative of Robert's uterus. Here, we reported same case that was initially diagnosed by ultrasound scan and confirmed by MRI technique.
Abnormal fusion of Mullerian duct in embryonic life is the origin of variety of malformations which may alter the reproductive outcome of the patients. Septate uterus is caused by incomplete resorption of the Mullerian duct during embryogenesis. Uterine anomalies can lead to infertility and problems with reproduction among women. A lot of uterine malformation like septate uterus, unicornuate uterus, and bicornuate uterus result from abnormal development of mullarian duct fusion during uterus development
The prevalence of septate uterus in the general population is 2.3%, the incidence of Robert's uterus is very rare with only handful of cases in published literature. Robert's uterus is a rare type of complete septate uterus [1] Characterized by uterine septum dividing the endometrial cavity asymmetrically resulting in formation of a noncommunicating hemi uterus due to obstruction by the septum. The external uterine contour is otherwise normal. It was first described and reported by Robert in 1970 [2] and it is also known as asymmetrical septate uterus.
Robert's uterus is a rare type of congenital uterine anomaly where septum divides the uterine cavity asymmetrically resulting in the formation of a noncommunicating hemiuterus. Patients may present with recurrent pain, dysmenorrhea, recurrent abortions, and infertility. [3] They are often misdiagnosed as unicornuate uterus with a noncommunicating horn.
Patients with Robert's uterus usually present with severe dysmenorrhea, recurrent abortions, infertility. Due to the obstruction by the septum, menstrual blood in the noncommunicating hemi uterus gets collected resulting in hematometra which causes severe dysmenorrhea. [1] The patients can also present with acute pain of the abdomen as an emergency. [2] Partial reflux of menstrual blood can cause hematosalpinx and even endometriosis as in this case. Very few cases of pregnancy in the noncommunicating half of the uterus have also been reported. [5,6]
Gynaecologist and sonologists should be aware of and alert to this rare entity while evaluating and managing cases of uterine abnormalities and endometriosis. Prompt early diagnosis and proper management of uterine abnormalities are important for avoiding future morbidity because these are major factors in protecting fertility. [4,5]
A 25-year nulliparous female with complaint of severe dysmenorrhea without bleeding per vagina since her menarche was visited to our clinic. She attained her menarche at the age of 12 years which was followed by severe dysmenorrhea in every month. She also complained there was no bleeding per vagina during periods. Only cyclical pain persisted and increased in intensity gradually, which was not tolerable. Her married life was 4 years, and she had a history of a spontaneous first trimester miscarriage, followed by secondary infertility for 3 years. She also had severe deep dyspareunia with gradually decreasing coital frequency. Since her menarche she was taking regular analgesics oral and parenteral and the frequency of same has increased in the last few years. On examination, her general condition was good and body mass index was 22.9 K/m2. Abdominal examination revealed no abnormalities but mild tenderness in hypogastrium and right iliac fossa with vague suprapubic mass on right side. Her speculum examination revealed healthy cervix and vagina. Vaginal examination revealed extremely tender bulky uterus deviated to right side with restricted mobility.
Laboratory investigations includes hematological and hormonal profile was done and were found with in normal limits. Her USG report showed noncommunicating cavitated uterine mass with deviated uterine cavity, with differential diagnosis of septate uterus with noncommunicating horn and enlarged cystic right ovarian endometrioma. There was also hemorrhagic collection in left endometrial cavity with liner calcification as described likely retained products of conception.
MRI report revealed bulky uterus with spitting of endometrium noted with intercornual distance at 2.06 cm, fundal cleft of <1cm>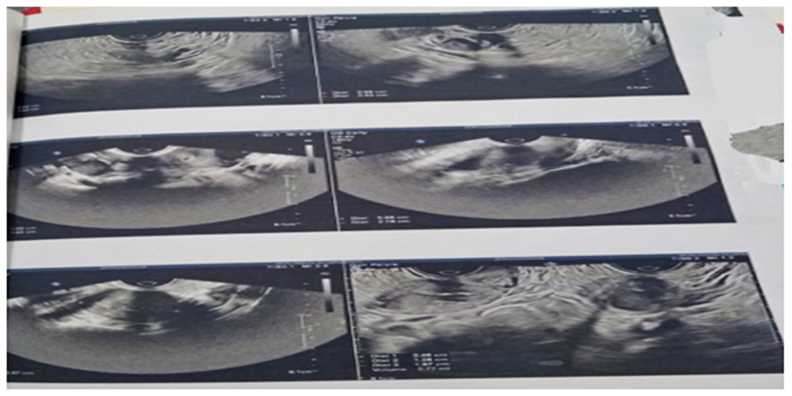
Uterine anomalies are related to an increased risk of infertility, miscarriage, premature birth, fetal loss and caesarian section. [5-7] In present case, according to the patient history, septate uterus has influences fertility and there was a previous history of abortion.
Ultrasonography is a simple, quick, and noninvasive technique for detecting and diagnosing uterine anomalies. Despite the notable advantages of this technique, unfortunately the obstetric ultrasound scan done on our patient could not detect the septate uterus as anomalies accordance with uterus exactly and it could be probably because of lack of experience. However, our MRI images diagnosed this problem accuracy. Grimbizis et al. reported that 12 (26.1%) out of their 46 infertile patients with septate uterus had laparoscopic finding of endometriosis. [7] Fayez also found endometriosis in three (43%) out of seven similar patients. [8] It seems possible that septate uterus may be involved in the pathogenesis of endometriosis and thereby plays an important role in indirect relationship within fertility. Therefore, it seems that any finding about endometriosis should be followed by carful investigation for uterine malformation especially in women affected by septate uterus.
There is not a single best modality of treatment of Robert's uterus. The surgery can be approached laparoscopically, hysteroscopically, or through a laparotomy. Total resection of the blinded cavity can be performed, [9] which was done in this case as attendant were not ready for any surgery having a chance of failure. A more conservative surgery in the form of excision of the septum with unification of the endometrial cavity can also be done. [9] Few cases of 3D ultrasound-guided hysteroscopic resection of the septum have also been reported. [10,11]
Robert's uterus should be kept as a possibility while dealing with suspected unicornuate uterus with hematometra. Primary surgery has the best chance and outcome in Mullerian anomalies, so should be dealt by an expert. Resection of hemiuterus necessitates complete shaving of the endometrium from the medial aspect to avoid the chance of recurrence. The reproductive outcome will be similar to the unicornuate uterus and elective cesarean section is advisable in view of scarred uterus and reduced volume.
The accurate diagnosis of Robert's uterus is difficult. It is mostly misdiagnosed as unicornuate uterus with a noncommunicating horn as in our case three times. Ultrasound and hysterosalpingography are the initial investigations done but are less informative as ultrasound is often operator dependent, and hysterosalpingography will not show the external uterine appearance and the noncommunicating part. MRI is the most informative noninvasive diagnostic modality in patients suspected of uterine anomalies. It will demonstrate the uterine septum as well as the normal external uterine contour which is necessary for differentiating the septate uterus from unicornuate uterus. The coronal T2W images of MRI are ideal for demonstrating the uterine septum dividing the endometrial cavity asymmetrically along with the blind ending cavity and hematometra. [7] The T1W images can show the presence of hematometra, hematosalpinx, if any. Retrospectively, MRI was re-evaluated and depiction of various structures is shown in Figure 4. In our case, the uterus appeared bulky and lobulated. There was a noncommunicating cavity on the right side of the uterus with T1 hyperintense contents and T2 shading suggestive of hemorrhagic contents. Hence, the diagnosis of obstructed rudimentary horn of the unicornuate uterus was given. To identify Robert uterus, one must look for single fundus, thick myometrium, presence of hematometra with oblique orientation of the septum joining the lateral uterine wall above internal os. Combined hysteroscopy and laparoscopy can accurately diagnose a Robert's uterus as well as differentiate it from the unicornuate uterus. The fundal contour will be normal in Robert's uterus, while there will be a fundal cleft >1 cm in unicornuate uterus. [8,11]
Robert's uterus is a rare anomaly and young women with Mullerian anomalies with intractable dysmenorrhea should be evaluated carefully to achieve a good reproductive outcome. The diagnosis of septate uterus as a congenital anomaly can be achieved easily with MRI. It can be corrected by hysteroscopic surgery and thereby decreases the rate of abortion for women greatly.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
