
Case Report | DOI: https://doi.org/10.31579/2640-1053/204
1Lecturer of Radiodiagnosis and Nuclear medicine, Faculty of Medicine, Ain-shams university. Radiology Consultant at Hayat National Hospital, Riyadh branch, KSA.
2Consultant of general Surgery at Hayat National Hospital, Riyadh branch, KSA.
3Specialist of general and plasic Surgery at Hayat National Hospital, Riyadh branch, KSA.
4Lecturer of Anesthesia and ICU, Faculty of Medicine, Alazhar university. Anesthesia consultant at Hayat National Hospital, Riyadh branch, KSA.
5Assistant professor of Radiodiagnosis and Nuclear medicine, Faculty of Medicine, Zagazig university, Zagazig, Egypt.
6ICU consultant at Hayat National Hospital, Riyadh branch, KSA.
*Corresponding Author: Noha Mohamed Taha, Radiology Department, Faculty of medicine, Ain shams university, Cairo, Egypt.
Citation: Noha M. Taha, Mohamed I. Ali, Mohamed Al-wazieery, Eldesoky Ibrahim Nouh, Ismail M Ali, et al, (2024), Rare case of retroperitoneal liposarcoma presented as perineal swelling (The tip of Iceberg), J. Cancer Research and Cellular Therapeutics, 8(5); DOI:10.31579/2640-1053/204
Copyright: © 2024, Noha Mohamed Taha, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 23 July 2024 | Accepted: 05 August 2024 | Published: 12 August 2024
Keywords: retroperitoneal liposarcoma; mri; subcutaneous fat
Background: Primary typical and atypical lipomatous tumors are the most common soft tissue tumors, where liposarcomas are the most common sarcoma. They are mostly found in the retroperitoneum and extremities. Rarely these tumors could present as hernias through different hernial orifices, this case report presents a rare presentation of retroperitoneal liposarcoma presented as a perineal swelling herniating through the ischiorectal and ischioanal fossa.
Case presentation: A 53 years old male patient presented to the outpatient surgery clinic in Al-Hayat National Hospital, Riyadh, kingdom of Saudi Arabia (KSA) complaining of swelling in the left gluteal area for two years, that progressively increased in size with no other symptoms. Magnetic resonance imaging (MRI) revealed a large retroperitoneal soft tissue mass lesion of fat content herniating into the perineal region. Complete surgical excision of this mass were done.
Conclusions: liposarcoma herniating through ischiorectal and ischioanal fossa are rare form of retroperitoneal liposarcoma as in this case where radiology plays an important role in initial diagnosis, staging and surgical planning.
Retroperitoneal sarcomas (RPS) are aggressive and rare type of malignant neoplasm, with incidence of about 0.5–1/100,000 inhabitants per year and account for 10–16% of all sarcomas [1]. RPS include heterogeneous and complex group of neoplasia, with four types represent almost 90% of all cases, these are, liposarcomas (LPS), leiomyosarcomas, solitary fibrous tumor, and malignant peripheral nerve sheath tumor [2].
Liposarcomas are the most common type of soft tissue sarcomas, they predominantly occur in the retroperitoneum and thigh [3]. Liposarcomas accounts for 20% of all retroperitoneal tumors and has multiple subtypes, including atypical, well-differentiated and dedifferentiated liposarcomas [4]. Due to the uncontrolled growth in the large potential space of the retroperitoneum, they mostly present with symptoms of mass effect with large median size reaching around 30 cm at the time of presentation making surgical management challenging [5]. Due to the large size of lipomatous tumors, they sometimes present as hernias which can occur through different hernial orifices either in the abdominal wall or in the groin. The herniated part of the tumor represents only the ‘tip of the iceberg’, as the main part of the tumor is not visualized clinically and is often underestimated, also this late presentation results in higher risk of de-differentiation [6].
A 53 years-old male presented to the outpatient surgery clinic in Al-Hayat National Hospital, Riyadh, KSA complaining of a swelling in the left gluteal area for two years (figure. 1), that progressively increased in size with no other symptoms. On clinical examination, the swelling was huge in size, soft, not tender not hot with normal overlying skin.
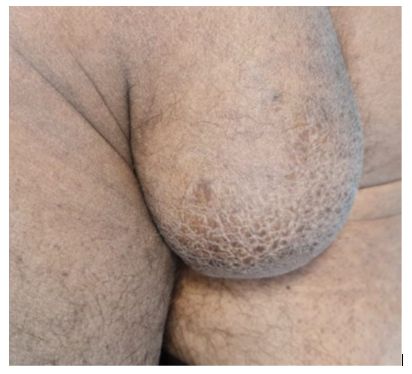
On clinical examination a huge, not tender, pedunculated mass was seen.
Figure 1: photo of the swelling on clinical exam
Ultrasound (US) examination was suspicious for a large gluteal lipoma. The surgeon requested MRI study with contrast for better assessment of the swelling and for pre-operative planning.
MRI was done including axial T1, T2, STIR WIs, coronal T2 and sagittal T2 WIs, then contrast was injection and axial, coronal and sagittal T1 fat suppressed WIs were acquired. On pre contrast images a large well-defined dumbbell shaped mass measuring 11.2 x 9.8 x 31 cm in the AP, TR, and CC dimensions respectively, was seen in the retroperitoneum extending to the left perineal region, filling the lower retroperitoneal/presacral space markedly displacing and compressing the
urinary bladder (UB) and prostate anteriorly (fig. 2a), inferiorly it was seen extending downwards at the left ischiorectal fossa, markedly compressing and displacing the rectum to the right side, also this lesion was seen herniating through the left pelvic floor muscles (left levator ani muscle) into the left ischio-anal fossa, displacing the anal canal to the right side and protruding outwards in the perineum (figure 2b). This lesion displayed predominantly hyperintense signal on T1 and T2 WIs that was suppressed in most of the lesion on STIR WIs (figure 3a, b, c). On post contrast images it showed heterogenous enhancing soft tissue components and thick internal septations (figure 4).
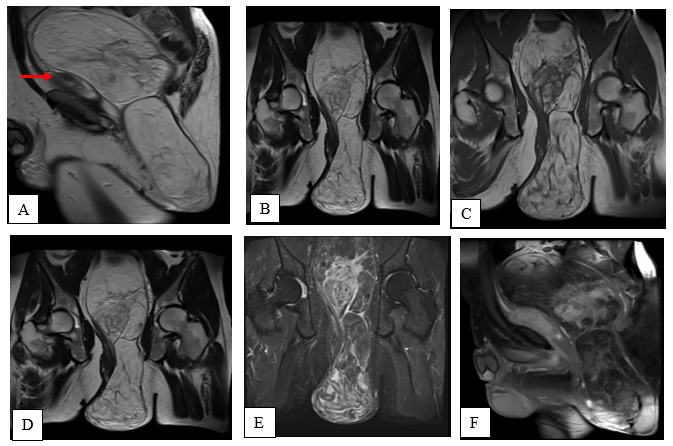
Figure 2: MRI examination of the mass
(A) Sagittal T2WIs shows a large dumbell shaped soft tissue lesion seen filling the presacral space and extending downwards into the perineal region. The prostate is seen markedly displaced and compressed anteriorly (red arrow). (B) Coronal T2 WIs revealed large lesion een extending from the retroperitoneal region inferiorly in the left ischiorectal fossa then through the left pelvic floor muscles (left levator ani muscle) downwards
in the left ischio-anal fossa, to protrude through the perineum.(C) Coronal T1 WIs (D) coronal T2WIs, (E) STIR WIs revealed large soft tissue lesion displaying hyperintense signal in T1 and T2 WIs, most of the lesion is seen suppressed in STIR WIs with internal hyperintense soft tissue components and internal septations. (F)Post contrast MRI images of the lesion: Sagittal T1 fat suppressed post contrast images showed internal heterogeneously enhancing soft tissue components and thick enhancing septations.

Figure 3: The mass post-surgical excision
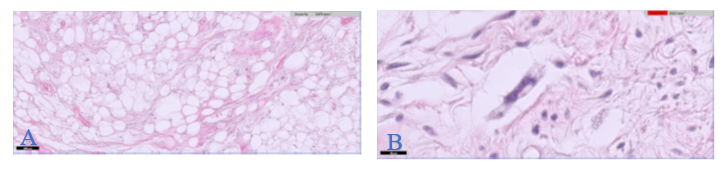
Figure 4: The histopathology of the excised maas show:
A) well-circumscribed hypocellular tumor composed of mature fat plus variably sized adipocytes and fibro-myxoid spindle cells. B) fibrous tissue septae are present containing spindle cells and highly pleomorphic cells, some nuclei have sharply outlined vacuoles (Lochkem) with very few lipoblasts.
The patient was prepared for surgery. On pre-operative assessment, according to The American Society of Anesthesiologists (ASA) classification the patient was ASA1, Exploration laparotomy was through midline incision, the small bowel loops were retracted upwards, the sigmoid colon and rectum were pushed to the right side. Opening of the posterior parietal peritoneum was done and the mass was localized and dissected after securing both ureters laterally. The herniated part was pushed up into the pelvis through retroperitoneal blunt dissection until the mass was completely excised. Hemostasis and then close of the peritoneal defect were done, intra-abdominal suction drain was inserted then the incision was closed in layers (figure 5).
Transversus abdominus Plane (TAP) block was given at the end of operation and before awaking the patient for post-operative pain relief. Reverse given to awake the patient by Sugammadex. No mishaps during the time of anesthesia. After operation the patient was shifted to recovery room for 30 minutes, then admitted to ICU for monitoring of the patient vital signs as he had major surgery and to check his CBC, PH level, ABG and he spent 24 hours there. Histopathology of the excised mass confirmed the diagnosed of well differentiated liposarcoma (fig 6). The patient came for follow up in the surgery clinic which revealed complete disappearance of the large perineal mass. MRI assessment was done one month after surgery which revealed post-operative seroma with no sizable residual tumoral tissue
The current case represents one of the rare tumours - giant retroperitoneal well-differentiated liposarcoma that measured 30 cm in the maximal dimension -. Most retroperitoneal liposarcomas are large at presentation; nearly 50% of retroperitoneal sarcomas are greater than 20 cm at diagnosis [7]. Obstructive complications and organ displacement are the most prevalent symptoms that they manifest later [8]. According to the WHO 2020 classification, there are five main subtypes of liposarcomas: atypical lipomatous tumor (ALT)/well-differentiated liposarcoma (WDLPS), dedifferentiated, myxoid, pleomorphic, and myxoid pleomorphic [9]. All subtype of liposarcoma develops in the retroperitoneum. Most of them are dedifferentiated subtypes and well-differentiated liposarcomas. In the retroperitoneum, pleomorphic and myxoid liposarcomas are uncommon. Well-differentiated liposarcoma (ALT/WDLPS) is a mesenchymal tumor that is locally aggressive but does not spread. It is mostly composed of adipocytes and stromal cells, and it has focal nuclear atypia in both of these cell types [10]. Approximately 40–45% of all liposarcomas are ALT/WDLPS. The deep soft tissue of the trunk and proximal extremities is where it most usually manifests. Moreover, the retroperitoneum is frequently affected as in the present case. WDLPS is a synonym for ALT. Tumor location and resectability are the main factors that determine whether to use either term [10]. Retroperitoneal tumors are extremely difficult to completely excise and are best categorized as WDLPS. Three subtypes of ALT/WDLPS are distinguished histologically: (1) adipocytic (lipoma-like), (2) sclerosing, and (3) inflammatory [11]. The presence of more than one morphological pattern in the same lesion is common, particularly in retroperitoneal tumors. [12]. Dedifferentiated liposarcoma (DDLPS) is an ALT/WDLPS that progresses to a varied histological grade of sarcoma, typically non-lipogenic, either in the primary or recurrent phase [13]. A well-differentiated component may not be found. The high-grade component could sporadically be lipogenic. Roughly 90% of cases arise de novo, while 10
Retroperitoneal liposarcomas are rare soft tissue tumors, Familiarity with different imaging findings of liposarcomas and its rare presentations as a hernia through different hernial orifices is critical to ensure accurate preoperative diagnosis as well as proper treatment and surgical planning.
(KSA) kingdom of Saudi Arabia, (MRI) Magnetic resonance imaging, (CT) computerized tomography, (US) ultrasound, T1 time 1, T2 time 2, (STIR) short tau inversion recovery, (ASA) American Society of Anesthesiologists, (TAP) Transversus abdominus plane, (ALT/ WDLPS)) atypical lipomatous tumor/well-differentiated liposarcoma, Dedifferentiated liposarcoma (DDLPS), pleomorphic liposarcoma (PLPS), Myxoid liposarcoma (MLPS), malignant peripheral nerve sheath tumors (MPNSTs), solitary fibrous tumor (SFT), Arterial blood gases (ABG), Anteroposterior (AP), Complete blood count (CBC), craniocaudal (CC), Liposarcoma (LPS), Transverse (Tr). Retroperitoneal sarcoma (RPS). Weighted images (WIs).
This study was approved by the Research Ethics Committee of the Hayat National Hospitals, the requirement for written consent was waived in this case report and discussed and approved by the ethical committee.
Not applicable.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
The authors declare that they have no competing interest.
No Funds, sponsorship or financial support to be disclosed
For the collaborative group including:
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
