
Case Report | DOI: https://doi.org/10.31579/2641-0419/189
Department of Interventional Cardiology, Nepal Mediciti Hospital, Lalitpur, Nepal
*Corresponding Author: Anish Hirachan, Department of Interventional Cardiology, Nepal Mediciti Hospital, Lalitpur, Nepal
Citation: Anish Hirachan, Ranjit Sharma, Prabace Neupane, (2021) Rare Case of Dual Right Coronary Artery Intervention Presenting as Acute Coronary Syndrome. J. Clinical Cardiology and Cardiovascular Interventions, 4(16); Doi:10.31579/2641-0419/189
Copyright: © 2021 Anish Hirachan, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 31 May 2021 | Accepted: 02 August 2021 | Published: 06 August 2021
Keywords: acute coronary syndrome; right coronary artery; echocardiogram
Dual right coronary artery (RCA) is a very rare coronary anomaly. This anomaly is often undetected and may be totally asymptomatic to presenting as acute coronary syndrome.
Here , we present a young diabetic male who presented with acute onset severe chest pain of 30 minutes duration which was managed as acute coronary syndrome ( NSTE-ACS). His urgent coronary angiogram revealed single ostial origin of right coronary artery (RCA) with total occlusion from proximal segment followed by double right coronary arteries with their respective distal branches.
A 41 year old male presented to the emergency department with history of severe retrosternal discomfort of 30 minutes duration radiating to neck and jaw which was associated with nausea and profuse sweating. His general examination was within normal limits. His BP was 130 /70 mmHg, with HR of 56/min and was clinically afebrile.
Medical History:
He was a chronic smoker and diabetic on oral hypoglycaemic agents including oral metformin and glimipride daily. He had no know allergies, no thyroid disorders, dyslipidemia or any cardiovascular illness prior to admission.
Investigations:
After admission to the ER, urgent EKG done showed normal sinus rhythm with T wave inversion in lead III, I, and AVL with Mobitz Type II AV block. His biochemical parameters were within normal limits except for a rise in troponin level (8.5 ng/ml). His bedside echocardiogram showed no regional wall motion abnormalities with ejection fraction of 60 %, no effusion, normal aortic root dimension and no dissection. His Chest Xray was also normal. In the background of ECG changes and typical angina symptoms, he was preloaded with tablet ecospirin 300 mg, clopilet 300 mg and Atorvastatin 40 mg and shifted to cardiac catheterization lab for primary coronary intervention after a proper informed consent.
Management:
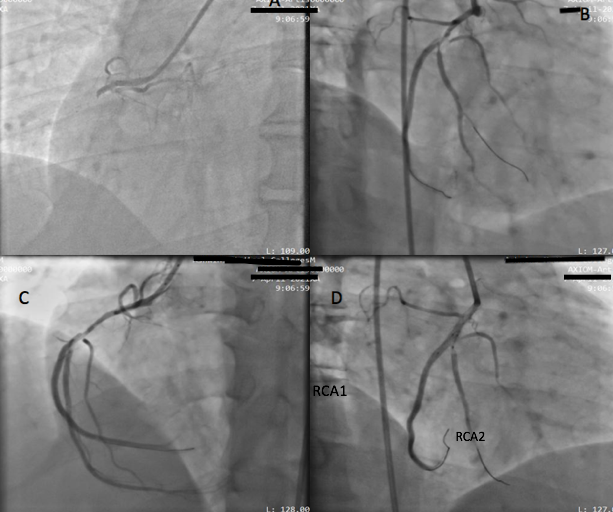
Urgent coronary angiogram done via right radial route showed normal origin, flow and caliber in left anterior descending artery (LAD) and left circumflex artery (LCX). Right coronary artery was originating from right sinus and had total thrombotic occlusion from proximal segment (Figure A). Further, coronary wiring was done with Sion Blue 0.014”
(ASAHI INTEC, Japan) wire through the lesion which revealed tight occlusive lesion at the proximal RCA after pre-dilatation with 2.0x12 mm non-compliant balloon at 13 atmospheric pressure (atm). Repeat angiogram in left anterior oblique (LAO) view and right anterior oblique view (RAO) showed single proximal RCA which bifurcated into two major RCA branches almost parallelly into giving separate distal branches with tight 90 % stenosis in proximal part of first RCA ( RCA1 ) and 70-80 % stenosis in the ostioproximal segment of the second RCA ( RCA2 ) ( Figure B and C ) . The coronary wire was re-parked into the larger RCA branch (RCA1) and the lesion was stented across with a Xience Xpedition 3X38 mm
( Abbot , USA ) drug eluting stent followed by a simultaneous kissing balloon inflation in both the stented segment and the ostioproximal segment of RCA 2 with 3x15 mm and 2.0 x 15 noncompliant balloon( NC) ( Figure D ) . No periprocedural complications noted and with residual less then 20 % -30 %stenosis in the second RCA branch (RCA2) (Figure E) . His hospital stay was uneventful with no peri and post procedural complications. He was discharged with dual antiplatelet, high dose statin and beta blockers and oral hypoglycemic agents and advised for a regular follwup at the cardiology clinic.

Various coronary anomalies are often incidentally detected on coronary angiogram. Double right coronary artery (RCA) is a very rare coronary anomaly, whose true definition and correct diagnosis remain controversial. [2] The first report about double RCA anomaly in the literature was by Barthe et al [3] where they observed double RCA originating from one ostium. Double RCA though being a relatively rare entity, it is not necessarily benign, as it has been associated with atherosclerosis, life-threatening arrhythmia and even myocardial infarction. [4-6] In the absence of atherosclerotic stenosis, ischemia can be a result of anatomical malformations, including an acute takeoff angle of the anomalous vessel, myocardial squeezing, vasospasm and a small artery. [7]
Some authors have claimed that it is very difficult to distinguish double RCA with single orifice, from RCA which has a high take- that off of a large right ventricular artery, solely by coronary angiography. Nevertheless, they have mentioned that right anterior oblique (RAO) view provides better demonstration of artery courses and may be helpful in differentiating double RCA from a large right ventricular branch. 8 Our index case had a thrombotic occlusion of the proximal right coronary artery which after pre-dilatation of the occluded segment revealed dual right coronary artery branches (RCA1, RCA 2) which were of equal caliber and coursed parallel and gave equal posterior descending branches towards the inferior myocardium. Further, the case was associated with a tight stenosis in the proximal RCA1 branch (posterior) as well as tight ostioproximal stenosis in the RCA 2 origin (anterior). Coronary angioplasty and stenting was done across proximal RCA to RCA 1 branch followed by simultaneous kissing balloon inflation across both the major RCA branches. Being an acute coronary syndrome with thrombotic occlusion, double stenting strategy was deferred despite of significant lesion across the proximal RCA 2 branch to keep the procedure quick and less complicated.
In most of the reported double RCA cases with atherosclerosis, the atherosclerotic segment is usually in the proximal part of the RCA that courses on the atrioventricular (AV) sulcus or in the posterior branch of the RCA going to the AV sulcus. [9] Similarly, our case had an acute thrombotic occlusion in the proximal RCA segment which underwent successful angioplasty
Follow-up:
The patient was symptomatically better and no fresh complaints at first follow up at first month after discharge.
Conclusion:
Double RCA though can be a very rare anomaly, every interventionist must be well familiar with this anomaly so as to make a proper examination and plan intervention accordingly.
Funding Support and Author Disclosures
I the principal author – Dr Anish Hirachan have no funding support or any grants as well as no disclosure to make. All other authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
