
Research Article | DOI: https://doi.org/10.31579/2641-5194/028
1 Senior Resident of General Surgery, Marmara University Department of General Surgery. İstanbul, Turkey.
2 Professor of General Surgery, Marmara University Department of General Surgery. İstanbul, Turkey.
3 Senior Resident of Nuclear Medicine, Marmara University Department of Nuclear Medicine. İstanbul, Turkey.
4 Professor of Nuclear Medicine, Marmara University Department of Nuclear Medicine. İstanbul, Turkey.
5 PhD, Marmara University Department of General Surgery. İstanbul, Turkey.
*Corresponding Author: Ömer GÜNAL, Professor of General Surgery, Marmara University Department of General Surgery. İstanbul, Turkey.
Citation: Kara B., Gunal O., Özgüven S. , Erdim A.4, and Tanju Y. Erdim (2021) Rapıd Lıquıd Phase Gastrıc Emptyıng may be the Harbınger of Sustaıned Weıght Loss after Laparoscopıc Sleeve Gastrectomy. J. Gastroenterology Pancreatology and Hepatobilary Disorders 5(3) DOI:10.31579/2641-5194/028
Copyright: © 2021, Iqbal Akhtar Khan ,This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 May 2021 | Accepted: 10 June 2021 | Published: 29 June 2021
Keywords: gastric emptying; bariatric surgery; excess weight loss; laparoscopic; sleeve gastrectomy
Study Contextual: 15-20 % Of laparoscopic sleeve gastrectomy patients need revisional surgery after LSG, because of inadequate weight loss.
Aim: The aim of our study is, primarily to analyze the relationship between liquid-phase gastric emptying rate and weight loss, to find a parameter that may be the harbinger of successful weight loss after LSG.
Methods: Patient records who have undergone laparoscopic sleeve gastrectomy were examined retrospectively. 44 Patients were included in the study. Preoperative weight and BMI, postoperative weight loss at first, third, and sixth months, surgical operation reports, preoperative and postoperative liquid-phase gastric emptying study values were mainly collected.
Results: The male/ female ratio was 18/82. Mean age 38 (19-60), mean body mass index 48,1(40-66) kg/m² and mean (EWL%) 63,17±13,94 were found. Mean pre and post-operative gastric emptying half times were found to be (T½) 41,86 minute(min), T½ 6,82 min (p<0.0001). Significant correlation was found between patients’ post-operative third and sixth month EWL% and post-operative T½ (p=0,020, p=0,032). Patients who have post-op gastric T½ above 10 min had decreased sixth-month EWL% significantly (p=0.03).
Conclusion: Post-operative gastric emptying time (T½) may be a harbinger of weight loss after LSG.
Laparoscopic sleeve gastrectomy (LSG) has become a frequent procedure in bariatric surgery due to its simplicity and efficacy compared with the gastric bypass procedure [1,2] LSG has succeeded in becoming the sole procedure for the management of morbid obesity and its associated metabolic diseases [3].
Excess weight loss (EWL) with sleeve gastrectomy is approximately 60-70%, which is comparable with the gastric bypass procedure [1]. Casella et al reported a 67.3% EWL at six years [4]. Since the first report by Gagner in 2000 [5], LSG is increasingly gaining acceptance as a surgical treatment of morbid obesity. In 2009, LSG was approved as a primary bariatric
This operation comprises major gastric resection, which can be associated with motor gastric dysfunction due to the resection of a gastric pacemaker, which causes multiple neurohormonal changes [7]. Approximately 30% of patients after LSG start to regain their lost weight [8]. This weight loss failure is correlated with factors related to the operation technique and pre-and post-operative neurohumoral and motility changes. However, the major success measure of LSG is usually the excess weight loss percentage. The clinical significance of accelerated gastric emptying after LSG is controversial. In one retrospective study, rapid emptying was associated with improved weight loss; however, this finding has not been confirmed [9].
This study aimed to search for a relationship between gastric motility and the short-term effect of LSG on weight loss in obese patients. We also intended to show a correlation between pre-operative or early postoperative gastric emptying time and EWL % as a harbinger of bariatric surgery success.
This study was performed to investigate the relationship between gastric emptying function and excess weight loss after laparoscopic sleeve gastrectomy. Our study is planned as a retrospective cross-sectional analysis of LSG patients who were operated on by one senior surgeon (ÖG). Institutional review board approval has been obtained. 117 Patients who have undergone LSG at a University Education and Research Hospital have been retrospectively scrutinized concerning the EWL and gastric emptying function. We have obtained 42 patients which were providing the inclusion criteria.
Inclusion and Exclusion Criteria:
Patients between 18-60 years of age, with a BMI >40 kg/m2, a BMI between 35-39,9 with comorbid diseases (e.g., hypertension (HT), diabetes mellitus (DM), hyperlipidemia (HL), and obstructive sleep apnea syndrome (OSAS)) were included. Patients who have pre-operative and post-operative gastric emptying studies were included. Patients who have undergone LSG and provided informed consent were included.
Patients who have undergone other abdominal surgery and patients who were lacking values in the post-operative follow-up records and without informed consent were excluded from the study.
The patient’s demographic data were recorded. Gastric emptying times which have been able to be reached were collected. Patients were also sub-grouped into good - excellent and poor weight loss patient groups, as suggested by Pereferrer et al.’s [10] He has classified his study group into three weight loss success groups (inadequate ≤50 EWL%; good = 51-65 EWL%; excellent ≥66 EWL%, respectively) according to their EWL% at post-operative three-month control examination.
Five trocars (two 15 mm, two 5 mm, one 10 mm) were employed in all operations. After greater curvature devascularization, which starts from the pylorus until the angle of His next to the esophageal wall, LSG was performed using a laparoscopic linear cutter. A 38 Fr bougie was employed in all gastrectomies. Gastrectomy was performed as close as possible to both the pylorus and gastroesophageal junction. The gastrectomy line was covered with a fibrin glue injection. A closed suction drain was placed through the area of gastrectomy to the left sub-diaphragmatic area. All operations were performed by a senior general surgeon (ÖG).
Calculations and Comparisons:
The “ideal body weight” (IBW) was calculated according to the ideal BMI of 25. The excess weight (EW) was calculated by subtracting the IBW from the actual weight of a patient. The percentage of excess weight loss (EWL %) was calculated by dividing the weight that was lost (WL) at the control time by the pre-operative excess weight.
EWL %=WLEW

X100
WL =Weight lost at any time point
EW= Pre-operative excess weight calculated according to the upper limit of 25 of a normal BMI
Gastric Emptying Study (GES):
All patients have undergone GESs at postoperative 1st month. Radionuclide studies of gastric emptying and motility are the most common physiologic studies of gastric motor function. This type of study is noninvasive, uses a physiologic meal (solids or liquids), and is quantitative [11]. All patients have undergone a liquid-phase gastric emptying study with the following technique:
Radiopharmaceutical and Liquid Meal:
All GESs were performed at the Nuclear Medicine Department of the Marmara University School of Medicine using a Siemens Symbia E (Erlangen, Germany).
All patients fasted for a minimum of six hours before the gastric emptying scan and were instructed to drink 200-300 cc of orange juice mixed with 99 m Tc-diethylene triamine penta acetic acid (DTPA). To clear the residual activity in the esophagus after ingestion of radiolabeled orange juice, a small amount of unlabeled water was given.
Image Acquisition:
Immediately after ingestion, dynamic images were recorded in the supine position at a framing rate of 60 seconds for 60 minutes in anterior and posterior projections. The oral cavity, proximal esophagus, thorax, and abdominal cavity were obtained in the field of view. Scintigraphic images were acquired with a gamma camera that was equipped with a low-energy high-resolution collimator with photopeak settings of 20% at 140 keV in a 128×128 pixel matrix.
The region of interest (ROI) was manually drawn over the entire stomach in the first frame image and applied to all dynamic images. The time-activity curve was generated by computer analysis from the counts displayed in the ROI. The data were corrected for radioactive decay. The rate of gastric emptying and retention were calculated at the end of the scanning. The time required for the maximum measured count to decrease to its half value ‘‘gastric emptying half time’’ (T1/2) was automatically calculated by a data processing unit. In cases in which half gastric emptying did not occur during 60 minutes of dynamic scintigraphic imaging, the ‘gastric emptying half-time’ was exponentially calculated by a ‘time-activity curve’.
Data Processing:
Pre- and post-operative gastric emptying studies were retrospectively reevaluated, and two more values were obtained from the audit of previous gastric scintigraphic studies. The gastric emptying rate (GEMR) was calculated as the emptying halftime of a gastric liquid meal (T½). We also calculated the 100% gastric emptying times (T0). Investigators were blind to GES results during the follow-up period.
Statistical Methods:
Parametric values were presented as the mean±standard deviation (SD), and nonparametric or categorical values were presented as the median (range of values). Numeric values with a normal distribution range were compared with the results (paired sample) of a Student's t-test. The Wilcoxon Test (paired sample) and Kruskal Wallis Test were performed for the values with non-normal distribution.
Non-parametric values were compared with the results of the Mann-Whitney-U test. Categorical variables were compared with a chi-squared test. The correlation between gastric emptying time and EWL was analyzed with Spearman’s correlation analysis. A linear correlation between the values was searched, and the degree of relation was presented as the “r” correlation coefficient. The coefficient interval was assumed to range between -1 and +1. The results fell within the 95% confidence interval. P values less than 0.05 were considered to be significant. An analysis of the outcome measures was performed with Statistical Package for Social Sciences 23,0 (SPSS version 23,0).
Patient Cohort:
This observational study was accomplished at the Marmara University Pendik Education and Research Hospital. This study was approved by the institutional review board. Hundred and seventeen patients who have undergone sleeve gastrectomy due to morbid obesity were evaluated retrospectively. Seventy-five patients have not included in the study, because they have one or more exclusion criteria. Forty-two patients' records that are suitable to inclusion criteria were evaluated.
Patient Characteristics:
The records of forty-two patients completely satisfied the inclusion criteria. The male: female ratio was 6/36. The mean age was 38, 27 years (19-60 years). Twelve (27%) of the patients have type II diabetes who were taking an oral antidiabetic or undergoing SC insulin therapy. Patient demographic data were presented in Table-1.
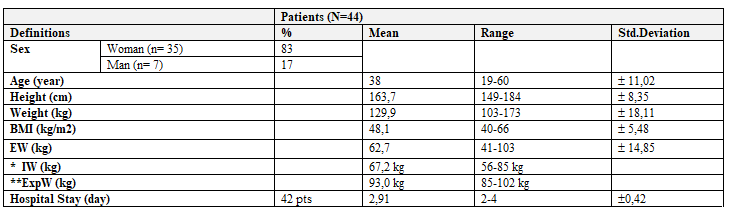
*Ideal weight: Calculated assuming BMI=25.
**Expected weight: Calculated assuming BMI=30.
Patient records were screened, and the post-operative first, third, and sixth month’s weight loss values were obtained. On physical examinations at each post-operative control period, excess weight loss (EWL) values and excess weight loss percentages (EWL %) calculated are presented in Table-2

Pre-operative and Post-operative GEMRs:
When the patients’ data were screened according to the inclusion criteria, 42 patients were determined to be eligible for the study. As a measure for the GEMR, T½, T0 (100% emptying time) were obtained from patients’ records. The post-operative GEMR significantly increased compared with pre-operative T½ (p<0>(Table-3).
Relationship between Pre-operative and Post-operative GEMRs and EWL %.
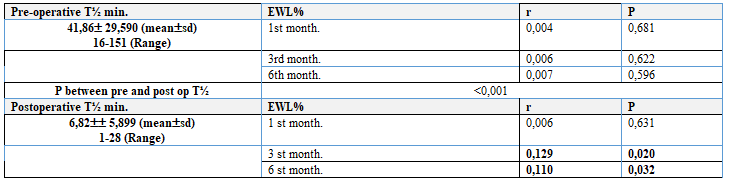
No relationship between the pre-operative T½ and the 1st, 3rd, and 6th-month EWL% values were found (p>0.05) (Table-4).
When the relationship between the 1st, 3rd, and 6th-month EWL% and post-operative T½ was compared, a significant correlation between the post-operative T½ and 3rd and 6th-month EWL% (p=0.02, r=0.129 and p=0.032, r=0,110, respectively) was observed (Table-4).
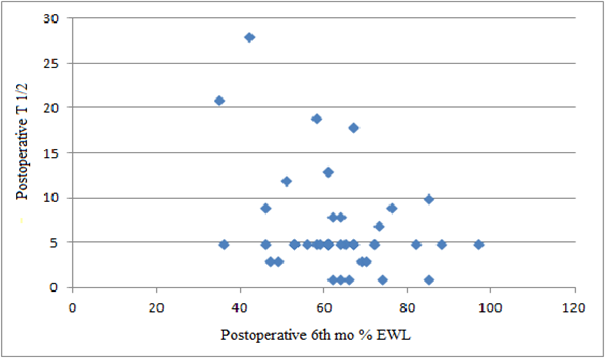
When we scrutinized the scattergram of the T½ and 6th-month EWL%, we noticed four patients who have T½ over 10 min. with weight losses <60>
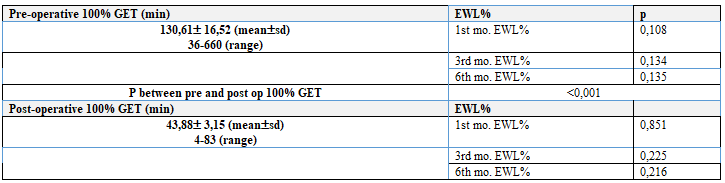
Relationships Between EWL% and 100% Gastric Emptying Time (GET), EWL%:
When pre-operative and post-operative T0 are compared, a significant decrease in T0 in the post-operative period (p<0>0.05) (Table-4).
The sixth-month EWL% values of 42 patients, which were included in the study, were grouped according to weight loss performance. The EWL% values of less than 50%, between 50-65%, and greater than 65% were considered to be the “inadequate", "good", and "excellent” weight loss groups, respectively. Eight (19%), 17 (40, 5%) and 17 (40, 5%) patients were in the “inadequate” weight loss group, “good” weight loss group and “excellent” weight loss group, respectively. The median EWL% values in each weight loss performance group were 44,6% (35,24-49,73), 61,1% (51,47-64,98), and 72,9%(65,74-97,74). The EWL% values of patients in the “good” and “excellent” groups were significantly higher than the EWL% values of patients in the “inadequate” group (p<0>
The post-operative T½ of the “inadequate” weight loss group was 10, 85±9,70 min. The post-operative T½ of the “good” and “excellent” groups was 5, 94±4,20 min. When a correlation analysis was performed between the T½ and EWL% of the groups, the post-operative T½ was significantly elevated in the “inadequate” weight loss group (p=0,034, r=0,108), as shown in Table-3, Figure-1.
Morbid obesity is increasingly becoming a visible reason for preventable death in both the adult population and childhood population. Bariatric surgery remains the most effective treatment modality of the morbid obesity and comorbid conditions that accompany this surgery. LSG is one of the most frequently performed bariatric surgical procedures in the world; in the USA, it became a widespread operation in 2014 at a rate of 51, 4% [12, 13]. Although this procedure has gained widespread acceptance, it has some drawbacks, such as the failure of EWL. According to data from Gagner et al, 3±6,3% of patients need secondary bariatric redo operations after LSG [14]. Rosenthal reported 30% of patients [15]. The success of surgery requires knowledge about the individuals who will join this population before inadequate weight loss or regain. Thus, we intend to evaluate the relationship between the EWL % and the GEMR (such as T½, T100%) with some causative factors to develop a harbinger of failed EWL or successful WL.
One of the mechanisms that is responsible for weight loss after LSG may be the altered GEMR. Until studies by Melissas et al [16, 17], LSG was considered to be an effective procedure for weight loss solely based on its gastric restrictive effect. However, in two patient series—11 and 14 patients—Melissas demonstrated that LSG increased GER in 2007 and 2008 that caused weight loss effect [16, 17]. Bragehetto et al. reported a significantly increased GEMR after LSG compared with the normal population [18]. Although the healthy population has a liquid phase GEMR (T½) of 34,9 minutes, morbidly obese patients have increased gastric emptying T½ (13,6 minutes) values (p<0>
Kandeel et al investigated the pre-operative and early post-operative (2nd week and 3rd week, respectively) liquid phase GEMR in a similar patient population. In this study, they observed a significantly increased GEMR after sleeve gastrectomy [2]. Shah et al. investigated the GEMR in diabetic patients. They compared pre-operatively diabetic patients (n=23) with pre-operatively non-diabetic patients (BMI<25 n=24)>33 of diabetic patients (n=20). They discovered that the solid phase GEMR was significantly high in the sleeve gastrectomized group compared with the non-diabetic group and diabetic group [19]. In our study, we observed a similar increase in the GEMR after LSG, which is consistent with the literature.
Due to the lack of receptive relaxation after fundus resection and alterations in gastric contractile activity after gastric pace-maker excision, shortening of the T-lag phase was assumed to be responsible for the increased gastric motility [16, 17]. Yehushua et al demonstrated that the increased intragastric pressure was the responsible factor for the elevated GEMR [20].
Regarding the LPGESs in the literature, Sista et al obtained a pre-operative T½ of 26,7±23 min (48 h) and post-operative (3rd mo.) T½ of 15, 2±13 min. in their 26 patient series [21]. Kandeel et al. obtained a pre-operative T½ value of 25,3±4,4 min and post-operative (3rd week) T½ value of 11,8±3,0 min. (2). Pre-operative mean±sd T½ value was 41, 86±29, 59 min in our obese patient series that seemed to be significantly increased concerning values in the above-mentioned series. Our study group's mean post-operative T½ value was 6, 82±5, 89 min., which seemed to be even faster than the results in the literature (Table-3).
We have not encountered a study that analyzed the relationship between the GEMR and EWL%. Our study is a peerless study from this point of view. Although the relationship between the pre-operative GEMR and EWL% was not significant, we have discovered a statistically significant relationship between the post-operative T½ and post-operative 3rd and 6th-month EWL%s (Table-4). Elevated GEMRs in the early postoperative period (postoperative 1st month) have significantly correlated with the postoperative 3rd and 6th-month EWL percentages. We explain the lack of a relationship between the first month EWL % and postoperative GEMR (T1/2) by the inefficient nutrition of patients during the early postoperative period.
The overall 6th mo. EWL% was 63, 17±13,94%. However, when patients with post-operative T½ values > 10 min were considered, the mean EWL% was 52,7±12,1%(n=6). The EWL%s of patients who have gastric T½ values of greater than 10 min. were significantly decreased when compared with the EWL% of patients who have less than 10 min gastric T½ values (p=0,03) (Figure-1).
When we sub-grouped the patients into good - excellent and poor weight-loss patient groups as suggested by Pereferrer et al.’s, the patients in the poor weight loss group have significantly less weight loss. This group contains eight patients (18%), which is convenient with the literature. Pereferrer et al reported this rate as 20% at the end of the first postoperative year [10]. We also have discovered that post-operative T½ values significantly increased in the inadequate weight loss group compared with the T½ values in the good-excellent weight loss groups. The mean T½ value of 10, 85±9, 70 min. in the inadequate weight loss group is consistent with the finding that the significantly increased post-operative T½ was observed in the inadequate weight loss group. (Figure-1) We note that six patients in the scattergram have T½ values greater than 10 min. and 6th-month EWL %s lower than 60%. The detection of these patient groups, which are not prone to good and/or excellent weight loss, should be performed with precautions and dietetic measures, such as following patients with more frequent intervals and requiring stricter diet regimens and behavioral therapy for these patients.
Ece et al. (n=402) reported a 53, 1±16, 1% EWL at the 6th month. Yardimci et al obtained a BMI of 32, 6±6, 2 kg/m² at the seventeen-month after LSG [22, 23]. Our patient population has gained a better sixth month EWL % (63, 17±13, 94%) than that of Ece at al series and similar BMI (34, 15±5, 17 kg/m²) with which Yardimci et al seventeen-month values. These authors have not linked the data with the gastric emptying function of the stomach.
The small number of patients (42) and a short follow-up period (6 mo.) may be considered limitations of our study. However, an engrossing aspect of our study with its short follow-up is the early measurement of GEMR at first month. EWL failure has been diagnosed as early as possible by this timely GEMR measurement and EWL% evaluation.
Despite this drawback of our study, the reverse correlation between the post-operative T½ and EWL % at the 3rd and 6th months presumed that the increased early post-operative liquid phase GEMR. T1/2, less than 10 min may be the indicator of fast excess weight loss. However, we need to perform long-term follow-up evaluations to determine the long-term weight loss effects of GEMR alterations after LSG.
Postoperative gastric emptying time (T½) may be a harbinger of sustained weight loss after LSG. Gradually increasing liquid phase gastric emptying T½ during postoperative follow up may be the forerunner of weight regain.
Authors declare that they have no conflict of interest with any institution or product related to this study
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
