
Re-Print-Research Article | DOI: https://doi.org/10.31579/2641-0419/045
1 The Heart and Vascular Institute, Germantown – USA
2 Autonomic Laboratory, Department of Cardiology, Drexel University College of Medicine, Philadelphia – USA
*Corresponding Author: Gary L. Murray, The Heart and Vascular Institute, Germantown - USA
Citation: Gary L. Murray., Colombo J. (2020) Ranolazine Improves Autonomic Balance in Heart Failure when added to Guideline-Driven Therapy. Clinical Cardiology and Cardiovascular Interventions, 3(2); Doi:10.31579/2641-0419/045
Copyright: © 2020 Gary L. Murray, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2020 | Accepted: 28 January 2020 | Published: 04 February 2020
Keywords: cardiovascular autonomic neuropathy; congestive heart failure; major adverse cardiac events; parasympathetic function; patient outcomes; ranolazine, sympathetic function
Background: The effect of ranolazine (RAN) on cardiac autonomic balance in congestive heart failure (CHF) was studied.
Methods: Fifty-four CHF patients were randomized to (1) open-label RAN (RANCHF) added to usual therapy vs.
(2) usual therapy (NORANCHF). Parasympathetic and sympathetic (P&S) measurements were taken at baseline and at 12 months.
Results: A total of 16/27 (59%) patients in both groups had initially abnormal P&S measures, including high sympathovagal balance (SB), cardiovascular autonomic neuropathy (CAN) or both. High SB normalized in 10/12 (83%) RANCHF patients vs. 2/11 (18%) NORANCHF patients. SB became high in 5/11 (45%) NORANCHF vs. 1/11 (9%) RANCHF patients. CAN improved in 4/6 (67%) RANCHF patients vs. 5/7 (45%) NORANCHF patients. CAN developed in 1/11 (9%) RANCHF vs. 4/11 (36%) NORANCHF patients. Since improved P&S in RANCHF patients seemed independent of improved brain natriuretic peptide and impedance cardiography (BioZ) measurements, 5 day RAN was given to 30 subjects without CHF but with high SB or CAN. P&S improved in 90% of these subjects.
Conclusions: RAN improves unfavorable P&S activity in CHF possibly by a direct effect upon autonomic sodium channels.
In congestive heart failure (CHF), there is an increase in the myocardial late sodium current (INa) leading to an intra- cellular calcium (Ca++) overload that causes diastolic dysfunc-tion, microvascular ischemia and early after-depolarizations, increasing the risk of sudden death. In therapeutic concen- trations, ranolazine (RAN) decreases the rate of INa by 50%, thereby improving this Ca++-related mechanical and electrical dysfunction [1]. Therefore, RAN potentially could improve the mechanical and electrical dysfunction of CHF. Since neuronal sodium channel 1.7 (Nav1.7) is blocked in its open state in a strongly use-dependent manner by RAN at therapeutic con-centrations (2-6 μM) via the local anesthetic receptor [2, 3], it is possible that RAN can directly alter the function of the parasympathetic and sympathetic (P&S) branches of the au- tonomic nervous system (ANS). Consequently, an additional potential benefit of RAN in CHF could be improvement in the damaging autonomic dysfunction that it accompanies. This is the first study on changes in P&S measures in CHF patients treated with RAN added to guideline-driven therapy.
In 2006, 54 patients treated for CHF according to ACC/AHA guidelines [4] were randomized to (1) open-label RAN added to usual care (RANCHF, n = 27) or [2] continued usual care (NORANCHF, n = 27) (Table 1). Since patients were on maximally tolerated doses of beta-blockers and angiotensin-converting enzyme (ACE) inhibitors or angiotensin receptor blockers (ARBs), only the diuretic dose was adjusted if needed. Diastolic CHF was defined as CHF with a left ventricular ejection frac- tion (LVEF) ≥0.40. At baseline, 2D echocardiograms, impedance cardiograms (BioZ, Cardio Dynamics, San Diego, CA) and brain natriuretic peptides (BNPs) were obtained. P&S function was assessed noninvasively using the ANSAR Medical Technologies, Inc. (Philadelphia, PA) software (ANX 3.0 autonomic function monitor) which computes simultaneous, independent mea- sures of P&S activity (P&S monitoring) based on continuous, Time–frequency analysis of heart rate variability (HRV) with concurrent, time–frequency analysis of continuous respiratory activity (RA). The following variables were recorded: seated resting (5 min) P&S activity (respiratory frequency area (RFa) and low-frequency area (LFa), respectively) was computed from P&S Monitoring [5-9]; exhalation/inhalation (E/I) ratio and RFa were computed in response to 1 min of deep breathing (paced breathing at 6 breaths/min) [9]; Valsalva ratio and LFa were computed in response to a series of short Valsalva maneuvers (≤15 sec); and BP, LFa, RFa and 30:15 ratio were computed in response to 5 min of head-up postural change (quick stand fol- lowed by 5 min of quiet standing). Sympathovagal balance (SB) is computed as LFa/RFa (reported means are averages of ratios, not ratio of averages). Cardiac autonomic neuropathy (CAN) was defined in standard fashion [10], reflecting very low para- sympathetic activity (RFa <0.1 bpm2). Parasympathetic activity (RFa) was defined as the spectral power within a 0.12 Hz-wide window centered on the fundamental respiratory frequency (FRF) in the HRV spectrum [5-9]. FRF was identified from time– frequency analysis of RA. Effectively, FRF is a measure of Vagal outflow, as it effects the heart. Sympathetic activity (LFa) was defined as the remaining spectral power, after computation of RFa, in the low-frequency window (0.04-0.15 Hz) of the HRV spectrum [5-9]. This method is valid regardless of challenge or patient state or history. Normal SB is 0.4< SB <3.0. High SB (>3.0) and CAN define high mortality risk, including silent myo- cardial infarction and sudden cardiac death [11-14]. The 30:15 ratio is the ratio of the 30th R-R interval after a quick head-up postural change (standing) to the 15th R-R interval after stand- ing. The 30:15 ratio reflects the reflex bradycardia upon stand- ing that is dependent upon sympathetic vasoconstriction. The Valsalva ratio is the ratio of the longest R-R interval to the short- est R-R during a 15 sec Valsalva maneuver. The E/I ratio is the ratio of the heart beat interval during peak exhalation over that during peak inhalation during paced breathing. The E/I ratio is a measure of, more or less, Vagal (parasympathetic) tone, as are the 30:15 and Valsalva ratios.
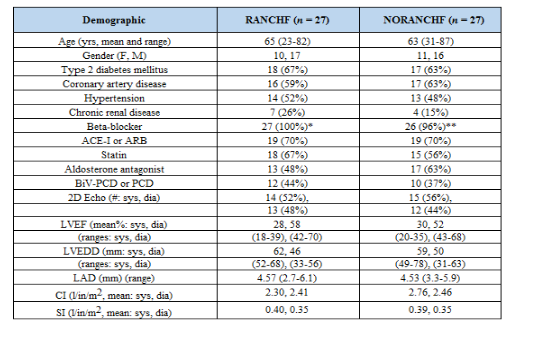
Table I lists the demographics of the RANCHF and NORANCHF populations. These two populations were well matched. CHF management guidelines [4] were strictly fol- lowed. Almost 100% of the patients were prescribed beta- blockers, 91% of the patients without chronic renal disease were prescribed an ACE inhibitor or ARB and 76% of the sys- tolic CHF patients had defibrillators. Over 60% of these popu- lations are diagnosed with diabetes.
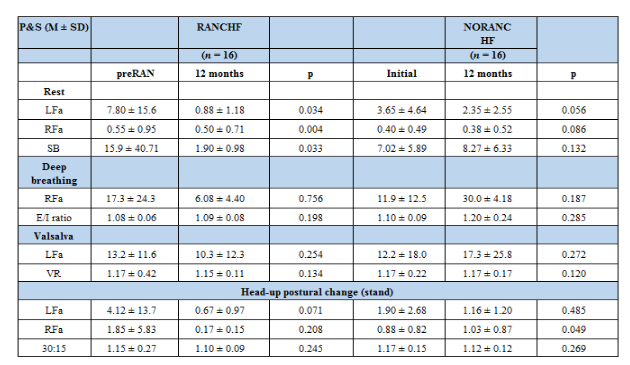
Average changes in abnormal P&S measures in RANCHF vs. NORANCHF patients are presented in Table II. Individually, 16/27 RANCHF patients (59%, including 9 systolic and 7 diastolic CHF patients) had abnormal baseline P&S responses: 10 patients (37%) demonstrated high SB, 4 patients (15%) demonstrated CAN and 2 patients (7%) demonstrated both Of the NORANCHF patients, 16/27 (59%) had abnormal base- line P&S responses, 9 patients (33%) demonstrated high SB, 5 patients (19%) demonstrated CAN and 2 patients (7%) demonstrated both. Fifteen of 16 RANCHF patients (94%) with initially abnormal P&S responses improved, and 14/16 patients (88%) normalized high SB and corrected CAN as compared with only 7/16 NORANCHF patients (44%) (p = 0.0330). On average (Table. II), the RANCHF patients demonstrated a significant improvement in SB (from 15.9 to 1.90, p = 0.0330), indicating a relative reduction in sympathetic activity. This is not the case for the NORANCHF patients (SB from 7.02 to 8.27, p = 0.130), whose SB remained high, indicating a persistent relative, rest ing sympathetic excess. Only 8/16 NORANCHF patients (50%) with abnormal baseline P&S improved (p = 0.0560). Individually, of the NORANCHF patients, only 2/11 (18%) normalized their high SB, as compared with 10/12 RANCHF patients (83%, p = 0.0130). Four NORANCHF patients (15%) demonstrated SB responses that became abnormally high during the 12 months of no RAN therapy. Individually, of the NORANCHF patients, 5/7 (71%) corrected their CAN as compared with 4/6 (67%) RANCHF patients. On average (TABLE. II), the resting parasympathetic response (RFa) for the RANCHF patients was higher (0.50 bpm2) than that for the NORANCHF patients (0.38 bpm2, p = 0.0040).
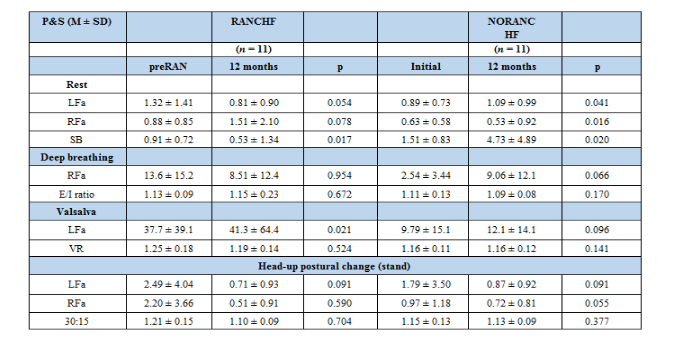
As a control experiment, we investigated changes in ini- tially normal P&S measures in RANCHF vs. NORANCHF patients
(TABLE. III). Individually, 11/27 patients (41%) from both RANCHF and NORANCHF populations demonstrated normal, baseline P&S responses. However, only 1/11 RANCHF patients (9%) de- veloped high SB as compared with 5/11 NORANCHF patients (45%, p = 0.0170). Similarly, 1/11 RANCHF patients (9%) devel- oped CAN as compared with 4/11 NORANCHF patients (36%, p = 0.0160). On average (TABLE. III), RANCHF patients demon- strated a decrease in resting, sympathetic activity at 12-month follow-up (p = 0.0540) as compared with an increase in the resting, sympathetic activity in the NORANCHF patients (p = 0.0410). Conversely (TABLE. III), the RANCHF patients dem- onstrated an increase in resting, parasympathetic activity at 12-month follow-up (p = 0.0780) as compared with a decrease in resting, parasympathetic activity in the NORANCHF patients (p = 0.0160). The resulting average SB for RANCHF patients de- creased (p = 0.0170), as compared with an increase in average SB for the NORANCHF patients (p = 0.0200).
Changes in BioZ and BNP measures in RANCHF patients with initially abnormal P&S responses are presented in Table IV. The hemodynamic responses to RAN were not uni- form. In the initially abnormal P&S response for RANCHF patients, no improvement in BioZs and BNPs was found in 7/17 patients (41%). Importantly, despite this, abnormal P&S responses improved equally well as in the RANCHF pa- tients whose BioZ and BNP responses improved, suggesting a possible direct effect on nervous system Nav channels. To investigate this possibility (TABLE. V), 30 subjects without CHF or an indication for RAN who had “CHF-like” high SB or CAN were given RAN. On the 5th day of treatment, P&S responses improved in 27/30 of the subjects (90%), normalizing in 20/30 subjects (67%). Isolated high SB normalized in 16/25 subjects (64%). The one subject with CAN demonstrated an increase in resting parasympathetic activity, relieving the CAN. For 3/4 subjects (75%) demonstrating both high SB and CAN, both P&S measures normalized. After discontinuing RAN, P&S responses returned to baseline levels.

The patient populations have significant subpopulations diagnosed with diabetes. This reflects the general population of Memphis, TN, the region of our clinic. It is one of the most obese populations in the United States. While diabetic auto- nomic neuropathy (DAN) is a well-known precursor to CAN and may affect P&S measures, including SB, P&S measures are similarly effected in patients not diagnosed with diabetes prior to CAN. The precursor to CAN in nondiabetic patients is advanced autonomic dysfunction (AAD). AAD carries the same P&S criteria as DAN: abnormally low P&S activity at rest, with p≥0.1 bpm2, with similar symptoms.
RAN affects cardiac Nav function by binding to Nav ami- no acid F1760 [1]. The late INa is reduced by 50%. Since RAN blocks open neuronal Nav 1.7 in a strongly use-dependent manner via the local anesthetic receptor [2], RAN could have direct effects upon ANS Nav channels.
High sympathetic activity and CAN have been associated with major adverse cardiac events (MACE), including sudden death [5, 11, 12]. Since structural abnormalities also increase MACE [13], baseline 2D echocardiograms were obtained. In our systolic CHF patients, structural findings were consistent with high MACE risk. Mean values for left ventricular end dia- stolic diameter (TABLE. I) and left atrial diameter were 61 mm and 45 mm, respectively. CAN is associated with very low resting parasympathetic activity. In this study, the RANCHF patients demonstrated more parasympathetic activity (TABLE. II). More sympathetic activity is known to increase cardiovascular risk [14]. More parasympathetic activity at rest is cardioprotective [15]. These effects of RAN are borne out in the control patients. The RANCHF control patients demonstrated a decrease in ab- solute resting sympathetic activity and an increase in absolute resting parasympathetic activity, with a decrease in SB. The converse is true for the NORANCHF patients (TABLE. III).
Despite aggressive CHF management, 32/54 (59%) of our CHF patients had initially high SB, CAN or both (TABLE. II). Ninety- eight percent of patients were on a maximum tolerated dose of beta-blocker. That 23/54 (43%) of the CHF patients’ base-line P&S responses demonstrated high SB is consistent with the prevalence of adrenergic escape in systolic CHF cited in a recent 415 patient study [16]. RAN improved abnormal P&S measures in our CHF patients, including an average 88% re- duction in SB (TABLE. II, p = 0.0330), and SB normalized in 10/12 (83%) of baseline high SB RANCHF patients. CAN improved in 5/7 (71%) of the RANCHF patients.
Although P&S measures change with changing hemody- namics [17-19], RAN was associated with P&S changes even when no definite changes in BNP or BioZ measures were found. Although the mechanism is unknown, a direct effect on nervous system Nav channels is possible. This is supported by the results in the 30 subjects with “CHF-like” P&S responses who had neither CHF nor an indication for RAN. Five days of RAN improved high SB and CAN in 27/30 (90%), normal- izing SB and CAN in 20/30 (67%) of subjects (TABLE. V). P&S re- sponses returned to baseline after discontinuing RAN. That P&S function can change independently of hemodynamics has been established. For example, diabetes control [20] and alpha lipoic acid [21] affect P&S and HRV measures. Notably, despite the favorable hemodynamic effects of renin-angio- tensin-aldosterone antagonists in CHF, their impact on HRV measures has been mixed [11]; however, this may be due to the mixed nature of HRV as a P&S measure calculated from 24-hour Holter monitors.
As expected, hemodynamics did affect P&S function in our CHF patients. On average, cardiac index (CI) was lower in the initially abnormal P&S response group (2.35 l/mim/m2) than in the initially normal P&S response group (2.66 l/min/m2). However, resting hemodynamics could not always predict abnormal P&S responses, as NORANCHF patients with ini- tially abnormal P&S responses had higher CI and lower BNPs than RANCHF patients with normal P&S responses (2.55 vs.2.35 l/min/m2 and 293 vs. 480 l/min/m2, respectively). That RAN improved hemodynamics more in our diastolic CHF than systolic CHF patients is consistent with RAN’s proposed mechanism of action (1), and suggests RAN could impact greatly the dyspnea of diastolic CHF. Our diastolic RANCHF patients (LVEF 41-54%) typically had a ≥10 LVEF unit (EFU) increase by 12 months and 45% of RANCHF patients (both systolic and diastolic) increased LVEF by at least 6 EFUs, some doubling their baseline LVEF.

Whether improved P&S measures in CHF patients are a surrogate for reduced risks of sudden death, disease progres- sion and hospitalizations remains to be determined. Toward these ends, preliminary evidence from a 3-year study in our laboratory, focused on echocardiographic changes in 54 RANCHF patients (41 systolic, 13 diastolic) vs. 55 NORANCHF patients (43 systolic, 12 diastolic), revealed that 21/55 (38%) NORANCHF patients had 35 MACE (hospitalized for CHF, had pacing cardiac defibrillator therapy for VT/VF or died), as com- pared with 17/54 (31%) RANCHF patients having 21 MACE (p = 0.0614). Of these 109 patients, 95 were successfully test- ed for P&S function. RANCHF patients and patients from both groups without MACE had lower SB; the RANCHF group also had higher parasympathetic modulation (RFa).
Despite aggressive guideline-driven therapy in CHF pa- tients, a significant number have unfavorable P&S profiles, even while taking up to 50 mg Carvedilol bid, or 200 mg Metoprolol daily. RAN causes a dramatic improvement in abnormal P&S measures, apparently independent of the CI or BNP responses. This suggests a possible direct effect on autonomic Nav channel function. RAN blocks neuronal channel Nav1.7. Worsening P&S responses appear to predict MACE. Therefore, P&S monitoring could become an important management tool in CHF. Current management of CHF does not include P&S measurements, so that the effect of beta-blockers and ACE inhibitors or ARBs upon the neurohumoral paradigm of CHF in our patients is never quantitated.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
