
Review Article | DOI: https://doi.org/10.31579/2640-1053/193
*Corresponding Author: Ankita Pandey, Department of radiotherapy and oncology, PGIMER, Chandigarh, India.
Citation: Ankita Pandey (2024), Radiotherapy in Hepatocellular Carcinoma – A Review of Literature, J. Cancer Research and Cellular Therapeutics, 8(3); DOI:10.31579/2640-1053/193
Copyright: © 2024, Ankita Pandey. this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 April 2024 | Accepted: 22 April 2024 | Published: 29 April 2024
Keywords: hepatocellular carcinoma; radiotherapyo utcome
Our knowledge of how radiation affects primary and secondary liver tumours is still developing. Decades ago, radiation delivery methods that treated large numbers of patients also cautioned against using radiation for definitive and palliative care. Over time, the function of radiation therapy in the treatment of hepatocellular carcinoma has changed. New information regarding HCC therapy choices has been made possible by the capacity to administer a tumoradical dose to liver lesions while protecting the normal parenchyma surrounding them. The purpose of the review article is to cone down various treatment approaches that were traditionally used to treat hepatocellular carcinoma and the gradual adaptation of the radiation therapy to treat lesions that failed to respond to other therapies.
Cancer incidence rises dramatically with age, most likely due to an accumulation of risks for specific cancers that rise with age. The accumulation of overall risk is combined with the tendency for cellular repair mechanisms to become less effective as a person ages[1, 2]. The risk factors of cancer include tobacco use, alcohol consumption, poor diet, inactivity and air pollution are all risk factors for cancer and other non communicable diseases. Some chronic infections are cancer risk factors; this is especially prevalent in low- and middle-income countries. Carcinogenic infections such as Helicobacter pylori, human papillomavirus (HPV), hepatitis B virus, hepatitis C virus, and Epstein-Barr virus were responsible for approximately 13% of cancers diagnosed globally in 2018[3]. Between 30 and 50% of cancers can currently be prevented by avoiding risk factors and implementing existing evidence-based prevention strategies. The cancer burden can also be reduced through early detection of cancer and appropriate treatment and care of patients who develop cancer. Many cancers have a high chance of cure if diagnosed early and treated appropriately[4, 5] .
Liver cancer remains a global health challenge and its incidence is growing worldwide. It is estimated that by 2025 more than one million individuals will be affected by liver cancer annually. HCC is the sixth most common cancer and the fourth leading cause of death. One reason for the high mortality rate is the disease unknown pathogenesis as well as the lack of early diagnostic and prognostic biomarkers[6]. Hepatocellular carcinoma is one of the most common cancers in the world and it poses a significant global health-care challenge. Although viral hepatitis and alcohol continue to be risk factors for hepatocellular carcinoma, non-alcoholic fatty liver disease is quickly becoming the leading cause. The risk attributed to hepatitis C virus (HCV) infection has substantially decreased owing to patients achieving sustained virological response (SVR) with antiviral drugs. Nonetheless, patients with cirrhosis are still considered to be at high risk for HCC even after HCV clearance. Non-alcoholic steatohepatitis (NASH) is associated with metabolic syndrome or diabetes mellitus and is becoming the fastest growing aetiology of HCC, particularly in the West. Additionally, reports on mutational signatures have established aristolochic acid and tobacco as potential pathogenetic cofactors in HCC[7].
Hepatocellular carcinoma is one area of oncology warranting further investigation into its epidemiology. Although, HCC is one of the first cancers to be linked epidemiologically to a definite risk factor (hepatitis B virus in Taiwan); the explanation for what accounts for the incidence of this disease is less clear. Although liver cancer is the sixth most common neoplasm worldwide, it carries poor prognosis which makes it the third leading cause of cancer-related mortality and is responsible for nearly 600,000 deaths annually. In most countries, HCC accounts for 70%–85% of primary liver cancer cases, with the burden of disease expected to increase in coming years[8].
The molecular pathogenesis of HCC differs depending on the genotoxic insults and aetiologies. Despite advances in our understanding of disease pathophysiology and drivers, this knowledge has yet to be translated into clinical practise. Approximately 25% of HCC tumours have actionable mutations; however, the prevalence of most mutations is 10%, making proof-of-concept studies difficult. Indeed, TERT, TP53, and CTNNB1 remain unsolvable mutational drivers in HCC[9].
HCC is typically diagnosed using non-invasive criteria, though there is a growing need in clinical practise for molecular characterization of the tumour using tissue biopsies. In terms of prevention, in addition to HBV vaccines and anti-viral therapies for HBV and HCV infection, cumulative data support the preventive role of coffee and aspirin. HCC management has significantly improved since the early 2010. Curative treatments for HCC have traditionally included hepatic resection and liver transplantation. Patients with hepatocellular carcinoma have a variety of treatment options, including liver transplantation, surgical resection, percutaneous ablation, and radiation, as well as trans arterial and systemic therapies. Refinements in patient selection have resulted in enhanced surgical resection outcomes and remarkable 10-year post-liver transplantation survival rates for tumours down-staged beyond Milan criteria[10].
Local ablation with radiofrequency remains the backbone of image-guided ablation for non-surgical early-stage HCC, despite progress in other techniques. Adjuvant therapies to preclude relapse, following these potentially curative approaches, are an unmet medical need, as randomized controlled trials (RCTs) have so far yielded negative results. For intermediate-stage HCC, transarterial chemoembolization (TACE) has been the most widely used treatment and the standard of care over the past two decades. As a result, clinical decision making necessitates a multidisciplinary team that adapts the individual treatment strategy over time based on the patient's tumor stage, liver function, and performance status. The treatment landscape for advanced hepatocellular carcinoma is more diverse than ever, thanks to the approval of new first- and second-line agents, as well as the acceptance of immune checkpoint inhibitor-based therapies as standard of care[11].
A systematic literature search was undertaken using the PubMed data base and secondary references to identify peer-reviewed articles that reported clinical outcomes in HCC after external beam RT alone or in combination with other treatments. More than 70 articles were identified and collected for the review article to identify the probable outcome of unresectable HCC patients after RT.
Local liver RT in unresectable HCC
The role of RT in HCC has not been defined in curative setting due to low tolerance of liver in a range of 30-35Gy, which is much less than the therapeutic dose. This much dose can lead to hepatomegaly, ascites, elevated liver enzymes and is due to veno-occlusive disease secondary to the fibrosis[12]. Because of this reason, unresectable HCC are mainly treated with more efficacious treatment modality that includes TACE. However, single setting of TACE may be not sufficient to completely eradicate the tumor. Due to dual blood supply, these tumors may grow in between the TACE sessions that may lead to reduced efficacy of this most commonly used method for unresectable HCC. To address this issue Seong J et al in 1999, combined TACE with RT in these patients. They reported that this method is well tolerated and leads to substantial decrease in size of the tumor [13]. To further expand the role of RT, in 2000 the authors published their experience on Local radiotherapy for unresectable hepatocellular carcinoma[14]. The purpose of their study was to investigate the efficacy of local radiotherapy (RT) as a salvage treatment for unresectable hepatocellular carcinoma (HCC) patients who failed with transcatheter arterial chemoembolization (TACE). TACE failure was determined based on incomplete lipiodol-Adriamycin mixture tumour filling either on angiography or computed tomography (CT) scan. From January 1993 to December 1997, 27 patients who had UICC Stage III (17) or IVA (10) disease entered into this study. Local RT was delivered with a mean tumour dose of 51.8 ± 7.9 Gy, in daily 1.8-Gy fractions using a 6 - 10MV linear accelerator. 66.7% patients had objective response including one with complete response. Intrahepatic and extrahepatic metastasis was seen in 10 and 4 patients, respectively. Survival rates at 1, 2, and 3 years were 85.2%, 58.1%, and 33.2%, respectively, from the diagnosis and 55.9%, 35.7%, and 21.4%, respectively, from the start of RT. The median survivals were 26 months from the diagnosis and 14 months from the start of RT. Acute toxicity included changes in liver function tests in 13 patients and thrombocytopenia in 2 patients. Subacute and chronic toxicity involved gastroduodenal ulcer (3 patients) and duodenitis (2 patients). No treatment-related deaths were seen. Authors concluded that in local RT caused a significant tumour response of 66.7% in unresectable HCC patients who failed TACE, with a 3-year survival rate of 21.4% and a median survival period of 14 months.
As the median dose of 51.8Gy was reported to be well tolerated in a mean tumor volume of 7.2±2.9cm, Laura A Dawson et al (2000) conducted research on Escalated Focal Liver Radiation and Concurrent Hepatic Artery Fluorodeoxyuridine for Unresectable Intrahepatic Malignancies[15]. In this phase I trial, the objective was to evaluate the response, time to progression, survival, and impact of radiation (RT) dose on survival in patients with intrahepatic malignancies. A total of 43 patients with either unresectable intrahepatic hepatobiliary cancer (HB; 27 patients) or colorectal liver metastases (LM; 16 patients) were treated with high-dose conformal RT with a median dose of 58.5 Gy (range, 28.5 to 90 Gy), 1.5 Gy twice daily, with concurrent continuous-infusion hepatic arterial fluorodeoxyuridine (0.2 mg/kg/d) during the first 4 weeks of RT. The median tumour size was 10 × 10 × 8 cm. Authors reported the response rate in 25 assessable patients to be 68% (16 partial and one complete response) and the median times to progression for all tumours, LM, and HB as 6, 8, and 3 months, respectively. The median survival times of all patients, patients with LM, and patients with HB were 16, 18, and 11 months, respectively. On multivariate analyses, improved progression-free and overall survival was associated with escalated RT dose. The median survival of patients treated with 70Gy or more was not reached (16.4+ months), while median survival in patients with lower dose RT was 11.6 months (p = .0003). Authors concluded that the excellent response rate, prolonged intrahepatic control, and improved survival in patients treated with RT doses of 70Gy or more motivate continuation of dose-escalation studies for patients with intrahepatic malignancies.
Cheng et al (2001) evaluated outcome, failure pattern and toxicity in patients with unresectable HCC treated with radiotherapy(n=9), TACE +RT (n=17) or TACE (n= 16) alone [16]. Mean RT dose was 46.9±5.8Gy in 1.8 to 2Gy daily fraction. TACE was performed using combination of lipiodal, doxorubicin, mitomycin C and cisplatin followed by Gelfoam or Ivalon embolisation. Worst survival was seen in RT alone group while TACE +RT and TACE treated patients had comparable 2 year survival rate of 58% and 56% respectively. Although intrahepatic recurrences outside the treated tumor were common and similar in these two groups, the extrahepatic progression free survival was significantly shorter in TACE+RT patients (2year rates: 36% in TACE+RT and 100% in TACE). One of the reason behind inferior outcome in RT alone patients were due to selection bias wherein advanced disease and compromised patients were included in this group. Authors concluded that local RT may be added to unresectable HCC that may result in control of progression of treated tumor even of larger size. Compared to previous two studies, the mean RT dose in this study was much lower.
Laura A Dawson and Chandan Guha (2004) in their review Hepatocellular carcinoma: radiation therapy[17] stated thatalthough whole liver tolerance to radiation therapy (RT) is low, hepatocellular carcinoma (HCC) can be treated with focal high-dose RT, using a variety of advanced and specialized treatment strategies like conformal RT planning, breathing motion management, and image-guided RT. Apart from this, use of charged particles that have a property of desirable dose distributions allowing tumoricidal doses to be delivered with sustained tumour control and little toxicity, even in the presence of Child-Pugh class B or C cirrhosis can also be used. Another strategy is hepatic arterial delivery of radioisotopes, such as microspheres tagged with yttrium-90. Hence, a more advanced form of RT techniques can help to deliver high dose to tumor with reduced and manageable radiation induced liver injury.
Similar study evaluating role of RT in HCC with portal vein or inferior vena cava tumor thrombi was conducted by Zhao Chong Zeng et al in 2005[18]. Forty-four patients received local limited EBRT (in addition to other treatment modalities) to a total radiation dose of 36-60 Gy (median, 50 Gy) and was focused on the tumour thrombi. One hundred fourteen patients with HCC who did not receive EBRT were classified as the non-EBRT group, and were treated with transarterial chemoembolization or resection, based on the patients' status. Of the 44 patients who received EBRT, 15 (34.1%) showed complete disappearance of tumour thrombi, 5 (11.4%) were in partial remission, 23 (52.3%) were stable in their tumour thrombi, and 1 (2.3%) showed disease progression at the end of the study period. The median survival was 8 months and 1 year in EBRT and non- EBRT group, respectively. In the EBRT group, poorer prognosis was significantly related to intrahepatic multifocal or diffusion lesions, and the most common reason for death was liver failure caused by uncontrolled intrahepatic disease. They concluded that although EBRT is palliative in intent, it is preferred for prolonging survival in the treatment of tumour thrombi.
Hani Soliman (2013) in Toronto evaluated the feasibility and response of liver radiotherapy (RT) in improving symptoms and quality of life in patients with hepatocellular carcinoma (HCC). Forty-one patients (30 men and 11 women) with HCC (n = 21) or liver metastasis (n = 20) with an index symptom of pain, abdominal discomfort, nausea, or fatigue were included in the trial. The Brief Pain Inventory (BPI), Functional Assessment of Cancer Therapy–Hepatobiliary (FACT-Hep), and European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire C30 (EORTC QLQ-C30) were completed by patients at baseline and each follow-up. The primary outcome was the percentage of patients with a clinically significant change at 1 month in the BPI subscale of symptom on average in the past 24 hours. Secondary outcomes were improvement in other BPI subscales and at other time points, FACT-Hep and EORTC QLQ-C30 at each follow-up, and toxicity at 1 week. At 1 month, 48% had an improvement in symptom. Improvements in the FACT-G and hepatobiliary subscale were seen in 23% and 29% of patients, respectively, at 1 month. There were also improvements in EORTC QLQ-C30 functional (range, 11% to 21%) and symptom (range, 11% to 50%) domains. Authors concluded that improvements in symptoms were observed at 1 month in a substantial proportion of patients[19].
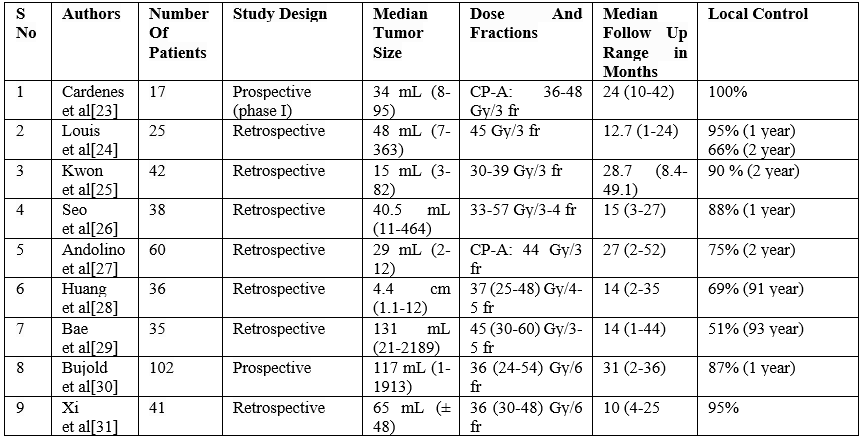
Table 1: Other Similar Studies In role of Stereotactic Body Radiotherapyin Hepatocellular cancer
Palliative Radiotherapy in Hepatocellular Carcinoma
External beam radiation therapy (EBRT) has historically only been used to treat HCC metastases that cause bothersome symptoms. External beam radiation therapy has been reported to be successful in treating metastases to the bone, lymph nodes, and soft tissues. For a very long time, HCC has been regarded as a radioresistant cancer[20]. Given that radiation-induced liver damage begins at a dose of 30 Gy, the whole liver could not receive more than this from traditional external beam radiation therapy. This dose level, however, is significantly lower than the typical doses of tumour radicals for the majority of solid cancers. Dose escalation is now possible thanks to technological advancements in radiotherapy precision delivery and normal tissue sparing. Regardless of the location of the tumour, radiation therapy is becoming more and more popular in the treatment of patients with advanced-stage HCC, and the outcomes are encouraging. Stereotactic body radiation or conformal high dose radiation therapy, has become a viable local treatment option for unresectable hepatocellular carcinoma. Numerous studies showed that the majority of patients had tumour control at one and two years. However, many patients are not appropriate candidates for high dose radiation due to the severe liver involvement associated with malignancy, borderline liver function, and/or the existence of extra-hepatic metastases. Radiotherapy has long been utilised to treat painful symptoms resulting from HCC metastases in a palliative situation. The most typical locations of extrahepatic metastatic
HCC include the lung, the abdominal lymph nodes, and the bones. There have also been reports in the literature of unusual metastatic locations, like the central nervous system[21]. HCC lymph node metastases are sensitive to EBRT within a dose range of 8-60 Gy. A dose of 50 Gy in 25 fraction was shown to be an effective palliative treatment for lymph node metastases in the Zeng et al series; nevertheless, survival declines with increasing lymph involvement distance from the liver due to the normal flow of lymph. The incidence of death resulting from lymph node-related complications was lower in the EBRT group in comparison to patients not receiving RT[22].
The use of radiation therapy to treat hepatocellular carcinoma has changed over time. The capacity to administer a tumoradical dosage to liver lesions while preserving the normal parenchyma around them has opened up new avenues for HCC treatment. Despite the long-held belief that HCC is a radioresistant cancer, the evidence supports the effectiveness and safety of radiation therapy for this condition. In terms of local control and survival, radiation treatments—either used alone or in conjunction with other local therapies like radiochemoembolization—show encouraging results. After a successful shift from radiotherapy's palliative role in HCC, we are now in a new era when patients who are not candidates for other therapeutic techniques can benefit from radiotherapy as an effective treatment.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
