
Case Report | DOI: https://doi.org/10.31579/JHV-2021/007
*Corresponding Author: Stephane Leung Wai Sang, Division of Cardiothoracic Surgery, Spectrum Health Meijer Heart Center, Michigan St NE, Grand Rapids, MI 49503.
Citation: Nathan D. DeBruine and Stephane L. W. Sang (2021) Quadricuspid Aortic Valve by Transesophageal Echocardiography. J, Heart and Vasculature 1(3); DOI: 10.31579/JHV-2021/007
Copyright: © 2021, Stephane Leung Wai Sang, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 01 March 2021 | Accepted: 02 April 2021 | Published: 11 May 2021
Keywords: quadricuspid; aortic; valve; echocardiography; transesophageal
Quadricuspid aortic valves (QAVs) are a rare congenital anomaly associated with increased risk of aortic insufficiency. This case presents the incidental finding of a quadricuspid aortic valve on intraoperative transesophageal echocardiography after going undetected on transthoracic echocardiography multiple times, suggesting that transesophageal echocardiography may be a superior imaging modality for the identification of this defect. This patient with a history of coronary artery disease presented with sudden onset moderate to severe aortic insufficiency and required subsequent AVR.
A 65-year-old female was found to have hypertensive urgency and diagnosed with pulmonary embolism shortly after undergoing a mandibulectomy for squamous cell carcinoma. She was found to have an acute coronary syndrome and subsequent transthoracic echocardiogram revealed an LVEF of 35%, though the quadricuspid aortic valve was not readily visualized. She then underwent left cardiac catheterization which demonstrated severe aortic insufficiency and 80% stenosis of the RCA. Her aortic root measured 33mm on preoperative CT angiography with the ascending aorta measuring 29mm. Patient was taken to the operating room and underwent single coronary artery bypass grafting and aortic valve replacement.
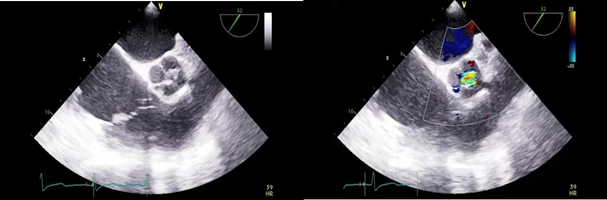
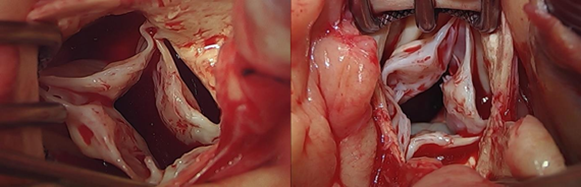
During this procedure, transesophageal echocardiography revealed the patient to have a four-leaflet aortic valve as shown in Figures 1a and 1b. The valve had four equal-sized cusps, as shown in Figures 2a and 2b, consistent with type A on Hurwitz and Roberts classification system.1 Aortic valve replacement was performed with a bovine pericardial tissue valve. The patient was discharged home without associated complication on postoperative day 20.
Quadricuspid aortic valves are a very rare congenital cardiac anomaly that usually present in isolation, but occasionally present with other defects. The bicuspid aortic valve is the most common aortic anomaly, present in 2% of the population, followed by the unicuspid aortic valve.2,3 QAVs have an estimated prevalence of 0.008–0.033% by autopsy and 0.013–0.043% by echocardiography.1,4 The first QAV was incidentally discovered in 1862 and less than 300 cases have been described since this time.5
Studies on Syrian hamsters have suggested that QAVs arise from an extra partition in one of the three mesenchymal swellings that form cusps during early development [6, 7]. Other studies propose that the anatomy of malformed semilunar valves tends to suggest an alteration later in development, such as further septation of a normal valve cushion, as opposed to a malformation.8 Embryological formation of QAVs remains largely unknown.
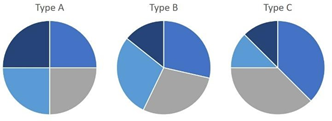
QAVs are classified into seven different types based on a schematic devised by Hurwitz and Roberts. Of these, Type A (four equal cusps), type B (three equal cusps and one smaller cusp), and type C (two equal larger cusps and two equal smaller cusps), are the most common presentations of QAV as shown in Figure 3.5 Our patient demonstrated a type A QAV based on this classification system, composed of four equal-sized cusps.
QAVs were historically detected primarily during surgery or at autopsy. They are now most often detected via echocardiography, followed by surgery, at autopsy, and by other diagnostic means such as computed tomography angiogram or magnetic resonance imaging. Transthoracic echocardiography is used as a primary screening tool, however the advent of transesophageal echocardiography has enabled increased diagnostic accuracy [9, 10]. TEE gives the transducer better access to image the aortic valve with less structures between it and the valve, as opposed to TTE which must penetrate lung and chest wall tissue [10]. This study provides one example of TTE failing to detect a QAV which was then detected on TEE. Screening with TEE rather than TTE may increase diagnosis of QAVs, ultimately improving patient outcomes without requiring magnetic resonance imaging or computed tomography angiograms [5].
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
