
Review | DOI: https://doi.org/10.31579/2690-8794/235
Dokuz Eylul University, Faculty of Medicine, Department of Dermatology and Venereology, İzmir, Turkey.
*Corresponding Author: Sevgi Akarsu, Professor, Dokuz Eylul University, Faculty of Medicine, Department of Dermatology and Venereology, İzmir, Turkey.
Citation: Sevgi Akarsu, (2024), Pyoderma Gangrenosum Associated with Multiple Myeloma: a Paraneoplastic Syndrome or Paradoxical Skin Reaction, Clinical Medical Reviews and Reports, 6(9); DOI:10.31579/2690-8794/235
Copyright: © 2024, Sevgi Akarsu. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 October 2024 | Accepted: 24 October 2024 | Published: 14 November 2024
Keywords: pyoderma gangrenosum; multiple myeloma; paraneoplastic syndrome; paradoxical skin reaction
The aim of this perspective article is to discuss the pathogenesis and treatment of pyoderma gangrenosum (PG), which can be seen as a paraneoplastic and/or drug-induced skin disorder in patients with multiple myeloma (MM). PG, a rare inflammatory neutrophilic dermatosis, may be idiopathic or associated with hematological malignancies at a rate of 3.9-45.6%. Among hematological malignancies, plasma cell dyscrasias (mostly IgA gammopathy) such as monoclonal gammopathy of undetermined significance and MM are the most frequently associated with PG. It is necessary to suspect and take place further investigations in terms of hematological malignancies including MM in cases of multifocal and recalcitrant ulcerative PG. Although conventional treatment in PG includes the use of immunosuppressive agents, PG may also occur in the presence of immunosuppression. Therefore, it should also be kept in mind that PG lesions may develop paradoxically when administering anti-myeloma treatments.
One of the rare extramedullary manifestations of multiple myeloma (MM), a plasma cell dyscrasia, cutaneous involvement occurs in less than 1-2% of cases. Both the rarity of specific cutaneous involvement (plasmacytoma) and presence of mostly nonspecific dermatoses in MM pose a challenge for dermatologists to suspect MM in the presence of a skin lesion [1]. Therefore, a high degree of clinical doubt, detailed medical history and histopathological correlation are mandatory for early and accurate diagnosis and management [1-2]. The purpose of this perspective article is to discuss the pathogenesis and treatment of MM-associated pyoderma gangrenosum (PG), which may be a paraneoplastic and/or a drug-induced dermatosis.
PG is an extremely rare (3-10 cases/million people/year) inflammatory, non-infectious neutrophilic dermatosis. It is characterized by painful necrotic ulcers that typically begin as an erythematous papulopustular lesion and rapidly enlarge with an irregular, violaceous and undermined borders, subsequently heal to leave permanent cribriform scars (Figure 1-2).

Figure 1. Rapidly progressing painful ulceration with necrotic areas and elevated erythematous-violaceous undermined edges
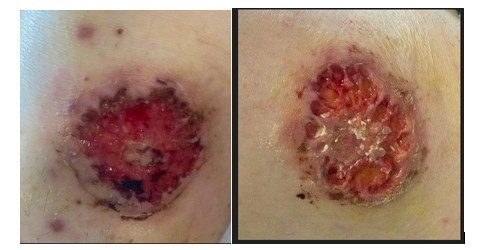
Figure 2. a) Erythematous papulopustular lesions, a round ulceration with violaceous and raised borders; b) subsequent healing with cribriform scars
Since there is no single pathognomonic finding, the diagnosis of PG is difficult and it can be confused with many conditions of circulatory, malignant or infectious origin. It is a diagnosis of exclusion with clinical presentation, compatible histopathology, negative cultures, positive pathergy, and even response to immunosuppressive treatment [2]. Diagnostic criteria for classic ulcerative PG were recently reported by the Delphi consensus of international experts [3].
Pyoderma gangrenosum as a paraneoplastic skin manifestation in multiple myeloma: PG, which can also be idiopathic, occurs in more than half of the cases in association with other conditions (inflammatory bowel disease, rheumatic disorders, hematological malignancies, respectively). The frequency of hematological malignancies associated with PG ranges from 3.9% to 45.6% [4-6]. In a systematic review examining 26 different diagnosis in 340 cases with PG-related hematological malignancies, myelodysplastic syndrome was observed most frequently, followed by monoclonal gammopathy of undetermined significance (MGUS), acute myeloid leukemia and MM. Of these cases, 22% were MGUS and 6.5% were MM, most of whom were IgA-type plasma cell dyscrasias [5]. When reviewing the literature, PG in some patients with plasma cell dyscrasia has been diagnosed before or concurrently with these hematological disorders [7-9]. In a recent population-based retrospective cohort study, it was shown that a previous history of hematological malignancy increased the likelihood of developing PG by approximately eight times. This association was reported most strongly for acute leukemia, MM, chronic leukemia, and non-Hodgkin's lymphoma. The highest rates of PG were observed in the first year following the diagnosis of hematological malignancy and gradually decreased thereafter. In this study, the risk of subsequent hematologic malignancy following PG diagnosis was not statistically higher than in the control group [6].
MM-associated PG is most commonly seen in the ulcerative type, shows a multifocal distribution, and has been found to be related with IgA kappa-type monoclonal gammopathy [5,10-12]. It has been demonstrated that bone marrow stromal cells secrete significantly higher levels of IL-8, and subsequent NF-kB activation increase the survival of MM cells [8,13]. Moreover, IgA may play a role in the pathogenesis of PG by increasing NF-kB activity, IL-8 production and neutrophil recruitment [14]. The significance of the predominance of IgA monoclonal gammopathy in patients with PG is unclear. Although the mechanism of this relationship is not fully understood, IgA paraprotein may contribute to the pathogenesis of PG and impaired skin healing by blocking the surface receptors of neutrophils or monocytes, reducing neutrophil chemotaxis and delaying leukocyte migration [10].
As known, PG treatment can be challenging. The mainstay of treatment is usually long-term immunosuppression, but it is widely stated that control of underlying diseases can lead to improvement of PG [2]. In these cases, surgery should be avoided because of the pathergy phenomenon or the development of new PG lesions (25-50%) even in minor trauma areas such as surgical incisions and venipuncture [15-16]. There is no specific treatment option for direct PG, and the aim is to control inflammation, reduce pain and accelerate healing. For this purpose, in addition to local wound care and treatments, oral dapsone, colchicine, systemic corticosteroids, cyclosporine, various immunosuppressive/immunmodulatory agents (e.g. methotrexate, thalidomide) and biologics (e.g. tumor necrosis factor‑alpha inhibitors) are recommended depending on the severity of the lesions and the comorbid conditions of the patient [2]. It has been found that some MM-related PG cases were resistant to steroids, various immunosuppressive agents, apremilast, rituximab, IVIG and other biological treatments despite variable responses, and responded to oral proteasome inhibitors (often bortezomib, alternatively the new agent ixazomib) [11,17].
Pyoderma gangrenosum associated with anti-myeloma treatments: Although PG is generally classified as a paraneoplastic skin finding in patients with MM, it may also occur in association with some anti-myeloma agents [4,18-19]. While the conventional treatment of PG includes the use of immunosuppressive agents, interestingly, it has been observed that PG can develop in the presence of immunosuppression. In the literature, PG development has been reported in cases where immunosuppressive treatments were used after solid organ and allogeneic stem cell transplantations [20-24]. Additionally, there are conflicting results regarding the efficacy of thalidomide and its derivatives (immunomodulatory agents used in MM) in PG (25-29). Although the usefulness of thalidomide has been reported in some articles [25-26,29], cases with newly developed or recurrent PG lesions with lenalidomide have also been reported [8,26]. Interestingly, lenalidomide-induced PG lesions were observed to regress with pomalidomide, which belongs to the same pharmaceutical class [7]. Besides that, although TNF-alpha inhibitors and rituximab are recommended in the treatment of PG, paradoxical PG has also been observed in patients using these biological agents for other reasons [19]. There are also conflicting reports regarding the effect of TNF-alpha inhibitors on MM [30-31]. It has been found that TNF-α-neutralizing antibodies or infliximab increase the cytotoxic effect of anticancer drugs by suppressing the TNF receptor/mTOR/NF-kB pathways [31]. However, progression to MM was observed with the use of infliximab in a patient with coexistence of PG and MGUS [30].
In routine practice, treatment is not recommended in asymptomatic silent plasma cell dyscrasias such as MGUS and smoldering MM, unless there is a progression to symptomatic MM. However, it has been observed that PG accompanying such asymptomatic plasma cell dyscrasias is resistant to dermatological managements and responds to early anti-myeloma treatments (bortezomib+dexamethasone±cyclophosphamide) [32]. Indeed, satisfactory results have been obtained by performing MM treatments in patients with monoclonal gammopathy who are recalcitrant and progress with diffuse and aggressive PG lesions [33].
As we know, it is necessary to suspect and take place further investigations in terms of hematological malignancies including MM in cases of multifocal immunosuppressive/immunmodulatory and biological agents also have conflicting effects on PG and MM. Therefore, it should also be kept in mind that PG lesions may develop paradoxically when administering anti-myeloma treatments.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
