
Case Report | DOI: https://doi.org/10.31579/2690-4861/166
1 Physician, Intensive Care Department. Hospital Nacional El Salvador.San Salvador-El Salvador.
2 Resident Physician, Intensive Care Department. Hospital Nacional El Salvador. San Salvador-El Salvador.
3 Infectology Service. Coordinator of the Antimicrobial Optimization Program Team, and Infection Control Coordinator Hospital Nacional El Salvador. San Salvador-El Salvador.
4 Epidemiologist. Expert Government of El Salvador. Official representative of the Government of El Salvador Global Initiative for Access to Vaccines (GAVI), WHO, PAHO and COVAX.
5 Physician, Head of Teaching and Research Department. Hospital Nacional El Salvador. San Salvador-El Salvador.
6 Director. Hospital Nacional El Salvador. San Salvador-El Salvador.
7 Physician, Head of the Intensive Care Department. Hospital Nacional El Salvador. San Salvador-El Salvador.
8 Student, fifth year medical degree. Universidad Jose Matias Delgado. San Salvador-El Salvador.
*Corresponding Author: Romina Georgina Bórtoli, Physician, Intensive Care Department. Hospital Nacional El Salvador.San Salvador-El Salvador.
Citation: Bórtoli RG, Goméz BCA, Ayala CEA, Cuellar AJD, Camputaro LA, et al. (2021) Pulmonary Candidiasis Associated with Severe COVID-19: Case Report. International Journal of Clinical Case Reports and Reviews. 9(1); DOI:10.31579/2690-4861/166
Copyright: © 2021 Romina Georgina Bórtoli, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 21 August 2021 | Accepted: 09 October 2021 | Published: 14 October 2021
Keywords: COVID-19 – Invasive Candidiasis; Fungal Infections; Pneumonia; Co-infections
Co-infections have been widely described in COVID-19 patients. Bacterial infections being the main cause but also have been reported fungal infections in up to 20 % of the cases. Candida species are the second most common fungi identified in pulmonary mycotic infections affecting hospitalized COVID-19 patients after Aspergillus. We present a case of severe COVID-19 associated with pulmonary candidiasis.
Co-infections have been widely described in COVID-19 patients. Bacterial infections being the main cause but also have been reported fungal infections in up to 20 % of the cases [1-2]. Candida species are the second most common fungi identified in pulmonary mycotic infections affecting hospitalized COVID-19 patients after Aspergillus [3]. We present a case of severe COVID-19 associated with pulmonary candidiasis.
Since the beginning of the COVID-19 pandemic co-infections have been frequently reported, mostly in hospitalized patients with moderate disease (2 - 27%), but also in patients with severe or critical COVID-19 (14 -58%), even more in the deceased (50%) [4]. Health-care associated infections are the cause of an increase in morbidity and mortality in patients with or without coronavirus infection.
The new coronavirus has caused an overload of the healthcare systems worldwide, initially all the effort was conducted to this new disease management. We adapted to this new situation by thoroughly research of the infection mechanisms and its complications, including bacterial and fungal co-infections.
Despite of advances in public health and hospital care, infections still emerge in hospitalized COVID-19 patients. Several microorganisms have been identified as co-pathogens, the bacteria are the most frequent isolated, and in less proportion fungal species. To date, the impact of the latter has not been entirely studied.
Patients with COVID-19 in the intensive care unit (ICU) are at high risk of developing healthcare-associated infections due to the requirement for invasive procedures. In these patients the main risk factors for developing invasive candidemia are: prolonged hospital stay, central venous catheters, surgical procedures and the use of broad-spectrum antibiotics [5].
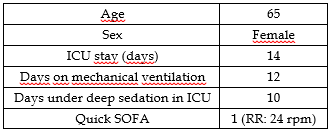
A 65-year-old female with previous diagnosis of diabetes mellitus, arterial hypertension and chronic kidney disease presented to a peripheral hospital in San Salvador with a 15-day history of fever, headache, dry cough, and progressive dyspnea. Upon admission SARS COV 2 pneumonia was diagnosed. Treatment was initiated according to the national protocol for moderate COVID-19, which at the time included: zinc, ascorbic acid, vitamin D, dexamethasone and anticoagulation with enoxaparin. Imipenem was also started due to a suspected co-infection. A positive urine culture for E. coli (sensitive to carbapenems, amikacin, ceftriaxone and levofloxacin) was reported, so a 4-days antibiotic treatment was completed.
Four days after hospitalization she was referred to our institution and admitted to the ICU due to severe respiratory failure. The patient required oxygen support with a high-flow nasal cannula to achieved an improvement in oxygen saturation and respiratory mechanics.
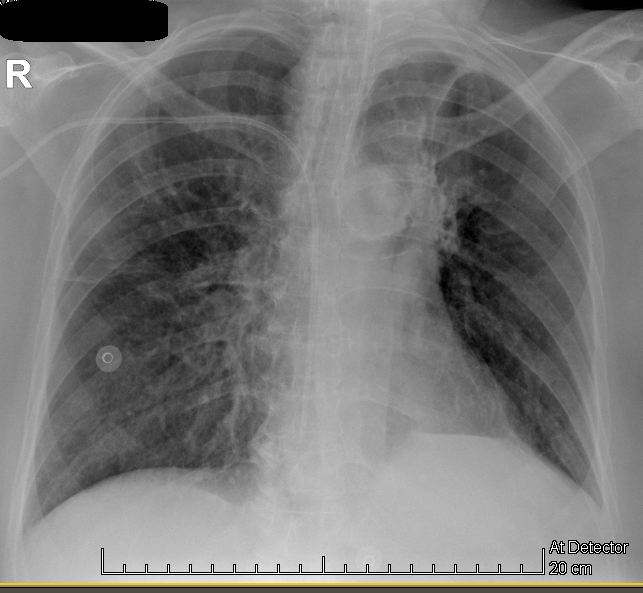
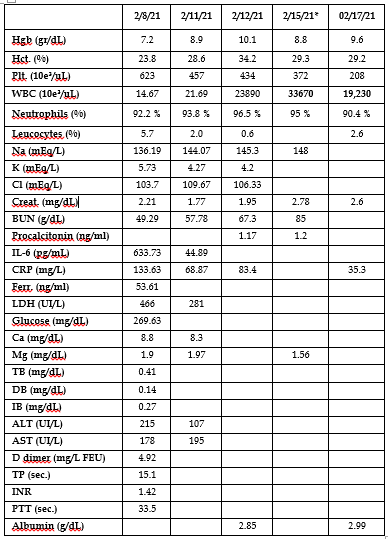
Laboratory exams on admission presented anemia, leukocytosis with neutrophilia, renal failure, elevated D-dimer and positive non-quantitative troponin (see Table 2). Chest X-ray showed diffuse interstitial-alveolar infiltrates, mainly localized in right lung apex and inferior lobe, without presence of consolidations or evidence of pleural effusion. (Figure 1)
Treatment according to the national protocol for COVID-19 was continued in our institution. Antibiotic therapy with levofloxacin was started for persistent suspicion of sepsis secondary to bacterial co-infection; antiviral treatment with remdesivir was also added.

The third day of hospitalization in our institution the patient had a 7 minutes cardiopulmonary arrest (CA). Non-ST segment elevation acute coronary syndrome was determined as probable CA cause by reason of the multiple cardiovascular risk factors. Post-CA studies showed acute ischemic changes in ECG with positive troponins, for which medical treatment was initiated. In the post-CA care, the patient required invasive mechanical ventilation and sedation analgesia; no need of vasopressors support as the patient present hemodynamic stability. In laboratory exams presented an increased in leucocytes account, suspecting a new nosocomial septic event could be another determinant of the clinical deterioration therefore antibiotic therapy was switch to piperacillin / tazobactam.
The following days, the patient present persistent increase in leukocytosis and required vasopressors as an evidence of organ dysfunction progression despite the use of broad-spectrum antibiotics. Given these clinical findings, an infection resistant to the antibiotics used so far was suspected and treatment with imipenem and vancomycin was started.
Despite broad-spectrum antibiotic treatment, covering possible gram-negative and positive bacteria, radiological deterioration was evidenced as a right apex consolidation, and increase in inflammatory markers in laboratory exams (Figure 2). After receiving a positive result in bronchial aspirate culture for Candida sp, the Infectious Disease Department suspended the antibiotic therapy and started treatment with fluconazole.

Forty eight hours after starting fluconazole, a clinical improvement was evidenced, presented decrease of inflammatory markers and a significant reduction of norepinephrine dose. Furthermore, radiological and oxygenation recovery allowed to reduced mechanical ventilation support. (Figure 3).
As result of the patient clinical condition improvement, progressive sedation de-scalation was performed until suspension, maintaining fentanyl at an analgesic dose. After sedation weaning it was possible to perform a complete neurological examination and a poor neurological response was evidenced (FOUR scale: 5) without sings of focal alterations. In consequence, the mechanical ventilation weaning turned out to be difficult. Unfortunately, the patient died a week after due to complications of post cardiac arrest syndrome.

Invasive Candidiasis in COVID-19
Microorganism of the Candida genus are part of the resident microbiota of the genitourinary and gastrointestinal tracts. However, when an imbalance in the ecological niche occurs, they can cause infections. Candidiasis is the most common invasive fungal infection associated with medical care, with recent global estimates reporting 750,000 cases of invasive candidiasis (IC) per year and more than 50,000 deaths. [6]
Clinical expression of Candida species infection varies from localized symptoms of the mucous membranes to generalized spread with multisystemic organ failure. [7]. Invasive candidiasis is a rare disease but is associated with a 30-day mortality rate over 35% in critically ill patients.
Primary Candida pneumonia is an extremely rare disease, described in less than 1% of cases [8]. Its pathophysiology is not well known, but it is likely associated with hematogenous spread rather than direct contamination due to aspiration. In a monocentric study of patients with mechanical ventilation, only 8% of the tracheal aspirate samples were positive for Candida, considering that 92% was colonization thus the colony count did not exceed the diagnosis threshold for mechanical ventilation associated pneumonia [9].
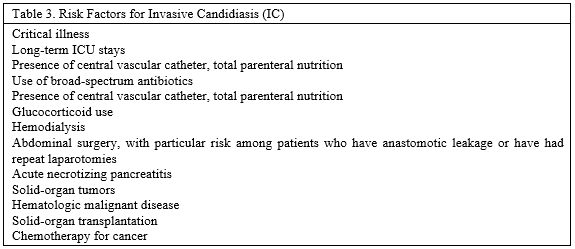
The incidence of candidemia is related to age, with the highest rates observed at the two ends of life. Various risk factors for the development of candidemia have been identified, allowing for the development of scores to determine the possibility of presenting a candida infection. (Table 3) [6].
The regulation of the host's immune response to the virus is one of the main pillars of COVID-19 treatment, as well as one of the potential risk factors for candida infection in these patients. Some of these treatments include immunosuppressive drugs as glucocorticoids, which have shown to decrease mortality, and also drugs that inhibit IL-6 action. Furthermore, critically ill patients require: prolonged hospitalization, central venous catheters and broad-spectrum antibiotic therapy, which at the beginning of the pandemic was excessive many of the protocols initially included antibiotic coverage at admission], all of these are risk factors for developing invasive infections caused by diverse Candida species [5].
The reported incidence of invasive candidiasis [IC] in COVID ranges from 0.7 to 23%. The pathophysiological mechanisms of COVID-19 are not fully understood, making it difficult to establish the pathogenesis of associated candida infections. The immunocompromise state caused by the coronavirus does not appear to be related to the immunity pathways intervening in candida infections, an example is the lymphopenia found in severe COVID patients, which is not associated to invasive candidiasis. Therefore, the incidence of candida infections is related to the usual risk factors and not to a specific immunocompromise state [5].
Primary Candida pneumonia is considered a rare disease at present, being little information regarding its pathophysiology available, hence the importance of reporting this clinical case. Colonization of the airway by Candida increases with the duration of mechanical ventilation, being 20% in the first 48 hours. Up to 90% of COVID patients who require hospitalization receive antibiotic therapy, which can increase the rate of colonization. Damage to the lung epithelium by viral invasion and the inflammatory response could facilitate the passage of candida into the bloodstream. Another possibility is Candida translocation from the gastrointestinal tract in patients who develop sepsis or septic shock [10].
The diagnosis of invasive Candida infections is challenging, specific characteristics of this type of infection such as transient fungemia, low fungal load in cultured tissues, not using specific culture media for fungi routinely or the need of invasive procedures for taking samples, makes it difficult to achieved microbiological isolation.
A positive blood culture is considered the Gold Standard for the diagnosis of candidemia. [11], but is a low sensitivity method, which varies from 21 to 71
Candida pneumonia is a rare complication in hospitalized patients. The importance of this pathology and others invasive candidiasis in outcomes y mortality in COVID-19 patients is matter of further study.
The authors declare that they have no conflicts of interest.
The publication of the case report was approved by the Committee of Ethics in Investigation Hospital Nacional El Salvador.
Funding
This case report did not have financial support.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
