
Case Report | DOI: https://doi.org/10.31579/2641-0419/130
*Corresponding Author: Atul Kaushik, Department of Cardiology, All India Institute of Medical Sciences, Basni Industrial area Phase II, Jodhpur, Rajasthan, India.
Citation: Vimal K. Yadav., Shailesh Jhanwar., Brij Mohan Goyal., Surendra Patel., Atul Kaushik., (2021) Pulmonary Artery Pseudsoaneurysm due to Mycobacterium Tuberculosis Managed Successfully by Transcatheter Coil Embolization. J. Clinical Cardiology and Cardiovascular Interventions, 4(4); Doi:10.31579/2641-0419/130
Copyright: © 2021 Atul Kaushik, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 January 2021 | Accepted: 15 February 2021 | Published: 22 February 2021
Keywords: mycobacterium tuberculosis; pulmonary artery pseudoaneurysm; transcatheter coil embolization; hemoptysis
Pulmonary artery pseudoaneurysm due to mycobacterium tuberculosis is a rare clinical entity. A 29 years old female presented to us with hemoptysis. She was a known case of pulmonary tuberculosis and was on antitubercular treatment. Emergency transcatheter coil embolization of the neck of the sac of pseudoaneurysm arising from the right descending pulmonary artery was done. At 6 months of follow up, the patient was asymptomatic. We are reporting this case due to a rare presentation of pulmonary artery pseudoaneurysm due to mycobacterium tuberculosis and pulmonary artery as an unusual source of hemoptysis instead of the bronchial artery.
Learning objectives
Pulmonary artery pseudoaneurysm due to Mycobacterium tuberculosis although rare but it's a potential life threatening situation, however early detection and prompt management may prevent fatal complications. Thus, the treating physician should keep this as a differential diagnosis whenever a patients presents with a massive hemoptysis.
Pulmonary artery pseudoaneurysms are uncommon but potentially life-threatening clinical entity since they are at high risk of rupture. Common causes includes infections (mycotic aneurysms), primary or secondary neoplasm, trauma, iatrogenic causes, pulmonary hypertension, and vasculitis [1, 2]. Patients usually present with hemoptysis, cough and shortness of breath [2]. The patient may presents with massive hemoptysis due to rupture of pseudoaneurysm and has a very high mortality rate [3]. Timely diagnosis and prompt intervention either transcatheter or surgical reduces the morbidity and mortality significantly. The present report highlights a case of right descending pulmonary artery pseudoaneurysm due to mycobacterium tuberculosis in a young female, which was managed successfully by transcatheter coil embolization.
Case presentation
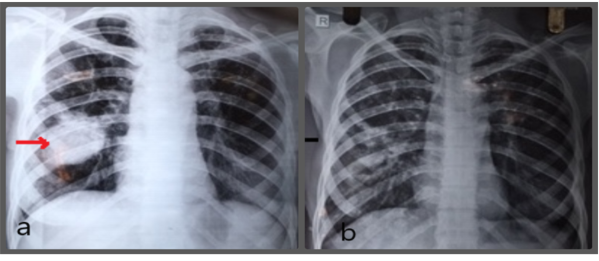
A 29-year-old female presented to us with recurrent episodes hemoptysis and shortness of breath for the last 4 weeks. Initially, hemoptysis was small in amount around 5-10 ml per day which increased to around 50-100 ml per day for the last 2-3 days. She was a known case of pulmonary tuberculosis and was on anti-tubercular therapy (ATT) for the last 6 months. On examination, the patient had a sinus tachycardia, blood pressure was 90/60 mm of mercury, mild tachypnea was present (respiratory rate 22/minute), and clinically pallor was present. Haematological and biochemical tests were within normal limits except for iron deficiency anaemia (haemoglobin was 7.2 gram/dl). A chest X-ray was done which showed a perihilar opacity which was extending towards right lower lobe [Figure 1a and 1b].
A computed tomography (CT) scan of the thorax was done, which showed a large (approximately 50x55 mm size) pseudoaneurysm arising from the right descending pulmonary artery. The patient was initially resuscitated with transfusion of 1 unit of packed red blood cells (PRBC). The emergency transcatheter procedure was planned.
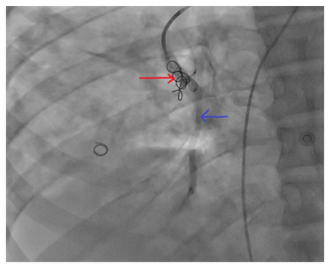
To find out the source of bleeding first, descending thoracic aortogram was done which showed that bronchial artery was not a feeding vessel of the pseudoaneurysm. After that pulmonary angiogram was performed via trans-femoral venous access. The pulmonary angiogram showed a large pseudoaneurysm originating from the right descending pulmonary artery, about 2-3 cm distal to the origin of the right middle lobe artery [Figure 2]. Embolization of the neck of the pseudoaneurysm sac was done with two 8x12 mm complex helical coil, one 3x5 mm cook coil, and two 4x5 mm cook coil. After the procedure, the pulmonary angiogram showed that there was no contrast leak into the sac of pseudoaneurysm and distal right lower lobar branches showing normal contrast opacification [Figure 3]. The postoperative recovery was uneventful and at 6 months of follow up the patient was asymptomatic and a chest x-ray was improved showing no residual pseudoaneurysm.

In the present era, the pulmonary artery pseudoaneurysms (PASA) are rarely reported due to the introduction of effective and potent ATT [1]. Mycobacterium tuberculosis affects the lung parenchyma in variety of pathological mechanisms including formation of tuberculoma, cavity formation, and erosion of tubercular cavity into adjacent pulmonary vessels resulting in pseudoaneurysm formation (Rasmussen's aneurysm) [4]. In most of the patients, the source of bleeding is bronchial arteries or non-bronchial systemic arteries. The pulmonary artery is a source of bleeding in less than 10% of the patients [5]. Our patient presented with hemoptysis and shortness of breath and had a history of pulmonary tuberculosis for the last 6 months and was on ATT. Probably, the tubercular lesion had eroded the pulmonary artery resulting in the formation of the pseudoaneurysm.
Transcatheter coil embolization of the bronchial artery or pulmonary artery pseudoaneurysm is the preferred approach, as this can be done easily in emergencies with massive hemoptysis [2, 6]. Sbano et al. reported that sometimes hemoptysis is not completely resolved in isolated bronchial artery embolization and requires coil embolization of the pulmonary artery pseudoaneurysm itself [6]. The open surgical technique involves thoracotomy with the removal of the involved lobe of the lung (lobectomy or sometimes pneumonectomy) for control of bleeding. As the open surgical technique has high morbidity and mortality in emergencies, it is reserved for stable patients or patients with failed transcatheter procedures [7].
In our patient, pulmonary artery was a source of bleeding which is quite uncommon. Transcatheter coil embolization of the pseudoaneurysm sac was done successfully and at 6 months of follow up, the patient remained asymptomatic.
Conclusion
Pulmonary artery pseudoaneurysm due to Mycobacterium tuberculosis is a rare clinical entity, which may present as massive hemoptysis that can be life threatening. However, early detection and prompt management via transcatheter technique may prevent mortality and further complications.
Acknowledgment: None
Financial disclosures: None
Conflict of interest: All the authors have no conflicts of interest to declare.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
