
Review Article | DOI: https://doi.org/10.31579/jsrbi.2021/005
1 Full Professor of Psychiatry University of Social Welfare and Rehabilitation Sciences (USWR) Razi Psychiatric Hospital Tehran – Iran
*Corresponding Author: Saeed Shoja Shafti, Full Professor of Psychiatry University of Social Welfare and Rehabilitation Sciences (USWR) Razi Psychiatric Hospital Tehran – Iran
Citation: Saeed Shoja Shafti, (2021) Psychosomatic Medicine: Reappraisal of a Concept in Developing Countries. J. Scientific Research and Biomedical Informatics, 2(1); Doi:10.31579/jsrbi.2021/005
Copyright: © 2021 Saeed Shoja Shafti, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 February 2021 | Accepted: 21 February 2021 | Published: 28 February 2021
Keywords: psychosomatic medicine; general hospital psychiatry; consultation – liaison psychiatry; consultation psychiatry; psychosomatic fellowship.
Consultation-liaison psychiatry is over 60 years old, and it emerged as an offspring of psychobiology, general hospital psychiatry, and psychosomatic medicine. While consultation-liaison psychiatry have played a major role in promoting the concept of integrated care, psychosomatic medicine continues as a science, studying the relationships between biological, psychological and social phenomena in health and disease, and the main promoters of the clinical application of the theories and discoveries of psychosomatic medicine are now the general hospital consultation-liaison psychiatrists and their allied health professional associates. Presently, a liaison service has become a recognized division of a general hospital psychiatric unit for the provision of psychiatric consultation and teaching to the non-psychiatric departments of academic hospitals. On the other hand, while in many developing countries the overall practice of consultation-liaison psychiatry remains quite basic, and it is mainly restricted to case-based consultation with other medical departments, it seems that psychosomatic medicine is not free from some sort of misperception, at least in some of the psychiatric departments in a number of developing countries. So based on the specific meaning of psychosomatic medicine in Diagnostic and Statistical Manual of Mental Disorders, and responsibilities of psychosomatic fellowship, which is determined by Accreditation Council for Graduate Medical Education, the concept of psychosomatic medicine has been reviewed once more, particularly from an educational perspective, and with respect to its current situation in developing countries.
Consultation-liaison psychiatry or general hospital psychiatry arose in the mid-1960s from the milieu of psychoanalytically oriented psychosomatic medicine. But, the influence of psychoanalysis and psychoanalytically trained academic psychiatrists slowly faded. On the other hand, the liaison part of consultation-liaison psychiatry wiped out in the early 1980s, and most consultation-liaison services are now primarily fine psychiatric consultation services. Accordingly, the consultation-liaison services at some academic centers have eliminated the term “liaison.” (1) Basically, the overall aim of psychosomatic medicine was to incorporate psychiatry into the whole of medicine. Moreover, consultation-liaison psychiatric services could provide better treatment opportunities in general hospitals for somatically ill patients with co-morbid psychiatric disorders. Hence, it has been suggested that consultation liaison psychiatry could be mixed with primary prevention in high-risk groups, such as accident victims, dialysis or transplantation patients. As a result, in some countries, growing attentiveness to psychiatric co-morbidity, especially in elderly general hospital inpatients, has led to increasing interest in integrated medical-psychiatric units [2]. In addition, psychosomatic medicine, also acknowledged as consultation-liaison psychiatry, received approval as a subspecialty field of psychiatry by the American Board of Medical Specialties in the spring of 2003. This denotes a vital step in the development of the field of psychosomatic medicine and recognition of its importance by leaders in the fields of medicine and psychiatry. The approval of subspecialty status for psychosomatic medicine could help to promote the psychiatric care of patients with complex medical, surgical, obstetrical and neurological conditions, along with promising further improvements in the quality of training and research in this important area [3]. From many years ago it was obvious that mental disorders may be both risk factors for and poor prognostic indicators in chronic medical illnesses such as diabetes, cardiovascular disease, and cancer. On the other hand, psychiatric morbidity is very common in patients with medical conditions, with a frequency ranging from around 20 to 65 percent, depending on the sickness. The practice of psychosomatic medicine has evolved noticeably since its early clinical origins and has come to focus on psychiatric disorders that occur in the setting of physical health care. Patients in the general hospital have the highest rate of psychiatric disorders when compared to community samples or patients in ambulatory primary care. For example, compared to community samples, depressive disorders in the general hospital are more than twice as common, and substance abuse is two to three times as common. Delirium, too, occurs in around 20 percent of inpatients. Psychiatric morbidity has serious effects on physically ill patients and is often a risk factor for exacerbation of their medical disorders. For example, it is well recognized that depression is both a risk factor and a poor prognostic indicator in coronary artery disease. Similarly, psychiatric disorder worsens cardiac morbidity and mortality in patients with a history of myocardial infarction, diminishes glycemic control in patients with diabetes, and decreases return to functioning in patients experiencing a stroke [4]. Additionally, depression and other mental disorders meaningfully impact quality of life and the ability of patients to adhere to treatment régimes. As a result, failure to identify, evaluate, diagnose, treat or achieve symptom resolution of psychiatric morbidity in medical care settings results in significantly increased service utilization. Therefore, the primary objective for psychosomatic medicine is the diagnosis and treatment of psychiatric ailments in patients with complex medical disorders. In addition to the care of specific conditions, psychosomatic medicine also includes a variety of other clinical accomplishments that occur in the medical setting, including evaluation of decision-making capacity, attention to quality of life and symptom management in chronic and terminally ill individuals, provision of liaison services to medical staff, and assistance with management of primary psychiatric conditions such as bipolar disorder or schizophrenia. In many settings, psychosomatic medicine psychiatrists function as part of multidisciplinary teams, which include psychiatry, psychology, nursing, and social work. In most cases, these teams work within medical specialty settings that provide care to special populations such as those with HIV, cancer, cardiovascular disease, transplant, and diabetes [4]. At this time, education and training in psychosomatic medicine are integrated throughout the psychiatry curriculum in medical schools and general psychiatric training. There are some curriculums, as well, that combine psychiatry with internal medicine, family practice, pediatrics, and neurology. The clinical activities in which psychosomatic medicine fellows must demonstrate competence have been indicated by the Accreditation Council for Graduate Medical Education (ACGME), which include a range of evaluative, diagnostic, therapeutic, educational, and collaborative responsibilities [4] (Table 1).
Background:
The term psychosomatic is derived from the Greek words psyche (soul) and soma (body). The term exactly refers to how the mind affects the body (5). Regrettably, it has come to be used, at least by the lay public, to describe a person with medical complaints that have no somatic cause and are “all in your head.” To some extent due to this misconceptualization, the American Psychiatric Association’s (APA) Diagnostic and Statistical Manual of Mental Disorders (DSM), in 1980, deleted the nosological term psychophysiological (or psychosomatic) disorders and replaced it with “Psychological Factors Affecting Physical Conditions” in DSM-5 [4]. The term psychosomatic medicine was first used by Felix Deutsch in the early 1920s. In 1968, John Schwab published the first consultation-liaison psychiatry textbook. The origins of consultation-liaison psychiatry fellowships can be traced to George Engel’s and John Romano’s fellowship program in psychosocial skills at Rochester University College of Medicine. This program, first offered in 1946, was offered to non-psychiatric physicians as well as psychiatrists. The Massachusetts General Hospital established its first consultation service in 1954. [6]. Consultation-liaison psychiatry (C-L psychiatry) was founded in the USA in the 1930's as a clinical pendant of psychosomatic medicine, and has now become an integrated part of the health care system in the North America and many of European countries (7). Besides, in 2003, the American Board of Medical Specialties and the American Board of Psychiatry and Neurology approved the specialty of psychosomatic medicine [8]. Historically, Walter Cannon and later Hans Selye explained the physiologic response to general stress. George Engel, as well, developed a stress theory based on conservation-withdrawal and helplessness. The concepts of alexithymia and Type A Behavior were also developed as contributing factors to disease. On the other hand, it became increasingly difficult to differentiate “psychosomatic medicine” from such fields as psychoneuroendocrinology and psychoimmunology. So, Engel proposed the Biopsychosocial Model as an alternative to the Biomedical Model prevalent in medicine [9]. Historically, psychosomatic medicine was known as consultation-liaison psychiatry, and it represented the care delivered by psychiatrists to patients with co-occurring medical and psychiatric problems who were treated primarily in medical settings [10]. In 1967, Zbigniew Lipowski formulated two most common diagnostic questions, which usually asked for psychiatric consultation: 1) Is this particular bodily complaint (or set of complaints) explicable as an expression of psychological ill-health, that is, is it partly or wholly psychogenic? 2) Is the inner experience of psychic change reported by the patient or his observable behavior explicable as the direct results of, or a psychological reaction to, organic disease? However, reasons for requests for help in patient management have extended since Lipowski’s formulation, and can be catalogued like this: 1) Suicidal attempt or threat, 2) Grossly disturbed behavior, such as, delirium and psychosis, 3) Excessive emotional reactions, such as, depression and anger, 4) Refusal to coöperate, 5) Delayed convalescence, 6) Conflict between patient and personnel, 7) Patient with psychiatric history, 8) Psychiatric side effects of drugs, 9) Selection and/or preparation of patients, such as, for surgery, 10) Disposition [4]. Therefore, consultation-liaison psychiatry, which is being practiced by general psychiatrists or psychosomatic fellows in general hospital settings, attempts to understand the biological and psychosocial aspects of patients including the role of genes, early environment, stress, and resilience in illness and health [9]. Current clinical trends in psychosomatic medicine include epigenetics, shortening and lengthening of telomeres, integrated care, placebo effect, etc. (11). In general, epidemiologic and clinical epidemiologic studies, mechanistic studies, treatment studies, and service delivery studies constitute the main field of investigations in psychosomatic medicine [4]. The approval of the subspecialty was both a response to and an opportunity for the field to highlight and expand the foundation in clinical care, research, teaching, and other scholarly activities related to the care of this special patient population. In this regard, the health psychology section of the American Psychological Association has over 3,500 members. In addition, social workers and nurses participate in care for these patients [4]. There has been an important development of consultation-liaison psychiatry in the last fifty years. Psychosocial factors and psychiatric symptoms which can be present in many somatic diseases have been considered as deserving of more specialized care. This could be achieved by a multidisciplinary team with the presence of a psychiatrist either permanently (consultation-liaison psychiatry) or episodically (psychiatric consultation). The said field is also involved with research and medical education. There is a general agreement that psychiatric care in a general hospital brings obvious benefits to the patient, to the psychiatrist, to non-psychiatric physicians, and to other team members, not only in terms of developing new professional opportunities, but also in terms of broadening the research field and improving medical education [12]. On the other hand, consultation-liaison psychiatry has had to reassess its priorities with the change in health care economics in the 80 s, and a need for focusing on cost-effectiveness of liaison services [13,14]. Now, psychiatric education in medical schools often includes a few months’ rotation to consultation-liaison service, which is now a need in psychiatry residencies [11].
Discussion:
Presently, a liaison service has become a recognized division of a general hospital psychiatric unit for the provision of psychiatric consultation and teaching to the non-psychiatric departments of the hospital [15]. Consultation-liaison psychiatry is over 60 years old. It emerged as an offspring of psychobiology, general hospital psychiatry, and psychosomatic medicine [18]. As is known, a third of medical and surgical out-patient clinic attendees have a psychiatric disorder. Half of these have depressive and anxiety disorders, and the rest have somatoform disorders. So, adequate recognition and treatment of their psychiatric disorder should be an integral part of management, since this has been shown to improve outcome. As said before, depression is a common cause of apparent worsening of a medical condition and panic disorder is an important cause of medically unexplained symptoms such as chest pain, dizziness and tingling. About 20% of medical and surgical in-patients have a depressive or anxiety disorder coexisting with their medical disease, 10% have a significant alcohol misuse problem and a third of elderly in-patients have an episode of delirium. Some patients with severe somatoform disorders get admitted and undergo multiple investigations and even surgery before the diagnosis is made. Psychiatric symptoms may be a response to the physical disease. For example, depression associated with cancer; sexual dysfunction after myocardial infarction; a body image disturbance after limb amputation. Moreover, there may be a shared cause, such as a major life event precipitating both a stroke and depression. The coexistence of a psychiatric disorder and a medical disorder is clinically important because it magnifies suffering and disability, prolongs medical care and increases overall health costs, and worsens outcome. For example, the mortality of heart disease, cancer or stroke is higher in those with a comorbid depressive disorder [17]. According to a study with respect to demographic and clinical characteristics of psychiatric referrals to psychiatric consultation - liaison service at a university hospital, the most common patient to be referred was a middle-aged woman. Internal medicine consistently accounted for almost one-third of all referrals, followed by neurology. The most prominent reasons for bio-psycho-social referrals were any signs of abnormal mood, behavior, psychotic symptoms or cognitive impairments. The most common mental disorders according to ICD-10 were adjustment disorders, depressive disorders, and delirium. Psycho-pharmacotherapy and combined psychotherapy and pharmacotherapy were the most frequent actions in both surveys, followed by bio-psycho-social evaluation pre-transplant [18]. Accordingly, psychosomatic medicine is the area of psychiatry concerned with the psychobiological care of the medically ill. This patient population includes people of all ages and those cared for in specialized locations such as surgery, internal medicine, organ transplantation, and many others. Psychosomatic medicine specialists, along with providing proficient formal psychiatric consultation to medical and surgical patients in the general hospital, specialized hospitals and outpatient clinic locations, also train psychiatrists and non-psychiatrist healthcare providers (e.g., neurologists, internists, surgeons, physician assistants, nurses) in the recognition of normal and abnormal reactions to disease and proper psychological care of patients with such reactions. Thus such a service functions both as a consultant and as part of the primary medical/surgical treatment team. By means of conjoint rounds and teaching sessions, formal consultations, and involvement in inpatient treatment and discharge planning, the psychosomatic medicine service provides a comprehensive approach to the behavioral, cognitive, and emotional needs of the patient [19]. Therefore, consultation-liaison psychiatry and general hospital psychiatry have played a major role in promoting the concept of integrated care. Due to the ageing population there is greater awareness of the importance of comorbidity and more support for the concept of integrated care. These changes will promote the further development of general hospital psychiatry [20]. Besides, there is a need for a valid taxonomy that addresses the most common form of psychiatric presentation in the community, the item of physical/psychiatric co-morbidity, and the outcome studies based on such taxonomy. Consultation-liaison psychiatrists need to inform their associates about the changes in concepts and terminology [21]. Therefore, generally, the major clinical problems in psychosomatic medicine include: psychiatric symptoms secondary to a medical condition, psychiatric symptoms as a reaction to medical condition or treatments, psychiatric complications of medical conditions and treatments, psychological factors contributing to medical symptoms, medical complications of psychiatric conditions or treatment, co-occurring medical and psychiatric conditions, and finally, psychiatric/psychosocial assessment. Psychosomatic medicine, whether as an integrated concept or divided impression, seems that is not free from some sort of misperception, at least in some of the psychiatric departments in a number of developing countries. Separating, scholastically, psychosomatic concept from consultation-liaison or consultation psychiatry, instituting indistinct psychiatric wards, designated as neurotic divisions, which involve a mixture of non-psychotic, non-suicidal, non-aggressive, non-addictive psychiatric patients, or wards involving neuropsychiatric cases, like epileptic patients with psychiatric comorbidities, are among the misapprehensions that may drive from the label of ‘psychosomatic’. Considering a specific clinical ward for psychosomatic patients in psychiatric hospitals, instead of general hospitals, is an incorrect perception that roots in old-fashioned dichotomy of soul and soma, mental and physical, or psyche and body, while supposing, unconsciously, psychosomatic equal to psychological. According to such out-of-date implication, treatment of each component’s ailment can be undertaken separately, without any precedence about the existent conditions. So, management of a patient with mild to moderate major depressive disorder, who may have an anemia, infection, or endocrine disorder, too, which has been detected during regular checkups, can be accounted as management of a psychosomatic case. So, it realizes the concept of psychosomatic in reverse, and wishes to treat a physical problem, which was not ever the main reason of reference, parallel to the management of primary psychiatric disorder, which was the foremost motive for seeking help, whether out-patiently or in-patiently. The case is more complicated when there is any suspect about the etiological role of medical illness in inducing psychiatric problem. The same problem, also, is true with respect to neuropsychiatric cases, where the same pathogenesis can be assumed about creation of both of physical ad psychiatric illnesses. Though all the said cases can be directly or indirectly, in the sphere of consultation psychiatry, psychosomatic medicine has its specific meaning: “Psychological Factors Affecting Other Medical Conditions”; a characterization that is specified in DSM-5 [22]. As stated by DSM-5, the essential feature of psychological factors affecting other medical conditions is the presence of one or more clinically significant psychological or behavioral factors that adversely affect a medical condition by increasing the risk for suffering, death, or disability. These factors can adversely affect the medical condition by influencing its course or treatment, by constituting an extra well-established health risk factor, or by influencing the underlying pathophysiology to precipitate or exacerbate symptoms or to cause medical attention [22]. Psychological or behavioral factors include psychological distress, patterns of interpersonal interaction, coping styles, and maladaptive health behaviors, such as denial of symptoms or poor adherence to medical recommendations. Many different psychological factors have been demonstrated to adversely influence medical conditions—for example, symptoms of depression or anxiety, stressful life events, relationship style, personality traits, and coping styles. The adverse effects can range from acute, with immediate medical consequences, to chronic, occurring over a long period. Many differences between cultures may influence psychological factors and their effects on medical conditions, such as those in language and communication style, explanatory models of illness, patterns of seeking health care, service availability and organization, doctor-patient relationships and other healing practices, family and gender roles, and attitudes toward pain and death [22]. Psychological factors affecting other medical conditions must be differentiated from mental disorder due to another medical condition, adjustment disorders, somatic symptom disorder, and Illness anxiety disorder [22]. So, primacy is in connection with the medical conditions, which are typically in the general hospitals or the associated facilities. In such a situation, the psychological factors may act as triggering or aggravating causes, which thus may demand supplementary psychotherapeutic or psychopharmacologic interventions, in addition to the current medical treatments. Such an intervention is asked by medical doctors and specialists, who feel or diagnose psychological problems in some of their medical patients. Accordingly, the later perspective, which recognizes mind and body as a cohesive entity that requests synchronized management, is different from the earlier outlooks, which habitually differentiates between mind and body and find the psychiatric problem as the main subject, by taking into consideration that patients who are admitted in the psychiatric hospitals or districts suffer from primary psychiatric disorders. Hence, psychosomatic ward does not have any working implication in the psychiatric hospitals. On the other hand, responsibilities of psychosomatic fellowship, which is determined by the related authentic experts, are clearly comprehensible (Table 1).
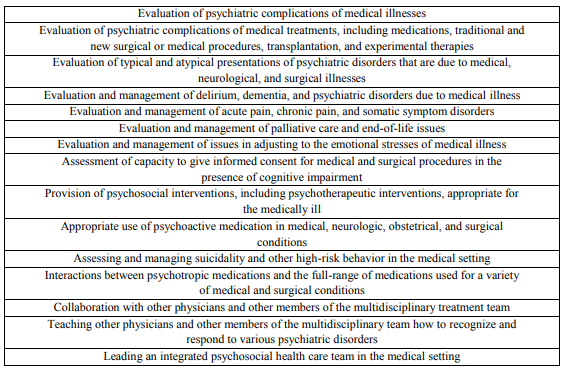
Adapted from Accreditation Council for Graduate Medical Education (ACGME) Program Requirements for
Graduate Medical Education in Psychosomatic Medicine. Available at
http://www.acgme.org/Portals/0/PFAssets/ProgramRequirements/409_psychosomatic_med_2016_1-
YR.pdf
Such group of tasks is not workable except than in general hospitals. By considering the other correlated terms, like general hospital psychiatry or psychological medicine, the necessity of implementation of consultation - liaison psychiatry in general hospital, as a mission that is set up by psychosomatic standpoint, becomes more palpable. On the other hand, while institution of psychiatric wards in general hospitals can be considered as part of a national mental health policy for academic integration of psychiatry into medicine, or as an administrative and remedial strategy with respect to deficiency of public psychiatric beds, labeling it as psychosomatic division is not sensible at all, because while the admitted patients in such kind of districts are generally acute primary psychiatric patients, psychosomatic medicine is typically with respect to chronic medical (physical) disorders. Also, since the psychiatric consultation is the backbone of contemporary psychosomatic medicine, without general medical wards undertaking such a mission is not attainable in a pure psychiatric hospital. As has been said by Jianlin et al [23], consultation-liaison psychiatry can be acknowledged as the clinical pendant of psychosomatic medicine, and no psychosomatic patient is plausible, independently, out of the aforesaid formulation.
Establishment of pure psychiatric wards, whether neurotic or else, under the name of psychosomatic division, without clarification of prime planning or obligation, may inspire an incorrect impression in the apprentices or ensuing psychiatrists, who may repeat it incorrectly in future. Though such a psychiatric ward can be helpful, educationally or clinically, it should have its own identification physiognomies, with no needless cover-up; if not, it is a contrived ward with deceitful messages. Since psychosomatic medicine, largely, take account of ‘cardiovascular disorders’, including coronary artery disease, congestive heart failure, arrhythmias, hypertension and stroke, ‘gastrointestinal disorders’, including inflammatory bowel disease and irritable bowel syndrome, ‘obesity’, ‘respiratory disorders’ including asthma, chronic obstructive pulmonary disease and interstitial lung disease, ‘diabetes’, ‘endocrine and metabolic disorders’, ‘psycho-oncology’, ‘end-of-life and palliative care’, ‘stress’, ‘psychiatric morbidity following critical illness’, ‘psycho-cutaneous disorders’, ‘organ transplantation’, ‘psychiatric care of the burned patient’, ‘management of chronic pain’ including migraine, tension-type headache, cluster headache, chronic daily headache, fibromyalgia, low back pain, phantom limbic pain, orofacial pain, and Parkinson disease, perplexing them with psychiatric disorders is a wrong attitude that may root in lack of insight as regards the philosophy of psychosomatic medicine. On the other hand, in many developing countries the overall practice of consultation-liaison psychiatry remains quite basic, and it is mainly restricted to case-based consultation with other medical departments (21). Anyhow, psychosomatic medicine continues as a science, studying the relationships between biological, psychological and social phenomena in health and disease, and the main promoters of the clinical application of the theories and discoveries of psychosomatic medicine are now the general hospital consultation-liaison psychiatrists and their allied health professional associates. Psychosomatic medicine is practiced in a variety of settings and comprises a mixture of consultative, treatment, and liaison undertakings. Historically, the most of this work has occurred within the general hospital setting. However, as more illnesses become chronic (e.g., HIV and cancer), there has been an increase in delivery of psychosomatic medicine services in outpatient settings as well. Regardless of where care is delivered, the basic approaches are similar: To conduct a psychiatric assessment, provide psychotherapeutic, behavioral, or pharmacologic interventions to patients, and to work thoroughly with other medical experts in a liaison dimension [4].
Conclusion
While psychosomatic medicine is a broad idea, for psychiatric assessment, management and collaboration with other medical specialists, its clinical, therapeutic, or investigational aims for further enhancement of care of medical patients with co-morbid psychiatric disorders is manageable only in the milieu of general medical hospital or related out-patient service area.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
