
Research Article | DOI: https://doi.org/10.31579/2578-8868/285
Psychiatrists, Pole Grand Avignon Alpilles CH of Montfavet.
*Corresponding Author: Gabriel Ifeoluwa Makinde, Institutional affiliation: Department of Community Medicine, College of Medicine, University of Ibadan.
Citation: Obioma C. Uchendu, Gabriel Ifeoluwa Makinde, Hadiza Adeoti, (2023), Psychometric Properties of Patients' Health Questionnaire Assessed on Obstetric Fistula Patients in Northwestern, J. Neuroscience and Neurological Surgery, 13(5): DOI: 10.31579/2578-8868/285
Copyright: © 2023, Gabriel Ifeoluwa Makinde. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 27 June 2023 | Accepted: 20 October 2023 | Published: 24 October 2023
Keywords: Identity; migration; transculturality therapy
Nigeria is among the highest contributor to global prevalence of obstetrics fistula (OF) and weak health care policies and services have left the victims reeling in untold psycho-social and physical morbidities. This study was aimed at assessing the psychometric properties of a globally used Patients’ Health Questionnaire (PHQ-9) among these patients. A descriptive cross-sectional study design was employed to study the fertility desires, mental health and patients’ quality of life among women with obstetric fistula in three selected OF centers in Northwestern region of Nigeria. Using two-stage sampling technique four hundred twenty (420) OF patients were recruited into the study. Maximum likelihood (ML) factor analysis was deployed to produce latent factors from the responses to the PHQ-9 scale, internal reliability and construct validity were determined by Cronbach alpha values while comparative mean analysis was used to validate standardized scores of the derived PHQ-9 scale factors against socio-demographic and obstetric characteristics. Mean age and standard deviation of respondents were 26.4±8.4 years as 60% aged between 20-25 years. The married, divorced and those in polygamous were 45%, 47.1% and 73.6% respectively. More than half (55.5%) were traders while majority (89.8%) earned NGN4500 or less monthly. Three factors of somatic (r= 0.72-0.82; α=0.86), non-somatic (r= 0.64-0.76; α=0.77) and affective (r= 0.64-0.96; α=0.74) constructs emerged from the ML factor analysis. Patients of ages 20-25 years, divorced/single and widows, the formally educated and farmers significantly differed with high scores of the affective construct of the PHQ-9 scale. Those who had more than four pregnancies and greater than a single stillbirth significantly differed with affective symptoms (0.29±0.90; 0.69±0.9 The 15–17-year-olds at first birth and those who waited more than ten years for OF surgical repairs differed with non-somatic symptoms’ construct of the PHQ-9 scale (0.21±1.04; 0.31±0.87) significantly differed with affective factors. The PHQ-9 instrument exhibited possibility of being used to assess the quality of OF patients’ mental health. Future studies could expand the sample size to accommodate advanced inferential psychometric methods.
Obstetric fistula (OF) which could be vesico-vagina fistula (VVF) or recto-vaginal (RF) fistula is a devastating condition in which urine or faeces ceaselessly leak through an irregular opening between a woman’s vagina and bladder (de Bernis et al, 2007). Globally, not less than 2 million sufferers of the condition are existing at an annual incidence estimation of 50,000–100,000 cases (WHO, 2014). The incidence in Africa is about 2–5/1000 deliveries and 33,000 new cases occur annually in sub-Saharan Africa (Umoiyoho et al., 2011). West Africa alone records an incidence of 3 to 4 cases per 1000 deliveries (Mikah et al, 2011). According to the United Nations Population Fund (UNFPA, 2014) Nigeria account for an estimated of 12,000 new cases annually with a current estimated total of 150,000 cases (WHO, 2014). The actual prevalence of obstetric fistula may be higher due to the under-reporting of cases in Sub-Saharan Africa (Okoye et al, 2014). Obstetric fistula is an outcome of elongated obstructed labor unrelieved by Cesarean section. Neonatal Fetal/early mortality results in most obstetric fistula cases, and hemorrhage, infection and infertility are some of the evidenced clinical complications in patients (Wall, 2006). Women who experience fistula frequently becomes victims of stigma, social ostracism, and withdrawal owing to the stench from urine/feces leaking from the vagina (Engender Health, 2006; Ahmed et al., 2007; Gharoro et al., 2009). These negative societal perception and actions towards VVF patients have resulted into report of high rates of general mental health breakdown, extreme depression to the level of multiple suicide attempts, low self-esteem and poor quality of life (Gharoro et al., 2009; Weston et al., 2011; Pope et al., 2011). Currently, the mental health effect of living with obstetric fistula has been acknowledged and reported (Bashah et al., 2018; Goh et al., 2005; Wilson et al., 2015). The WHO has advocated the addition of psychosocial support in the care of obstetric fistula (WHO, 2006). However, few Nigerian studies have attempted to quantitatively investigate the psycho-social dimensions of the impact of obstetric fistula on women. (Raji et al, 2021; Nduka et al, 2023). Accurately assessing and comprehending the mental health state of fistula patients is essential to providing them with holistic relief. There are several quality-of-life tools that can be used to measure patients’ health and psychological state which is a function of their cultural and value orientation in relation to their life’s goals and expectations (WHO, 1998). One of such tools is a widely used and validated Patients' Health Questionnaire (PHQ), created by Kroenke et al. (2001) for mental assessment and diagnosis in a variety of non-communicable disease conditions (Ngo et al, 2013; Kiene et al, 2017) Some researchers in sub-Saharan countries have validated their country’s language version of the tool (Sibera et al., 2020; Ssebunnya et al., 2019; Adewuya et al., 2006). Although, the primary validation study of the PHQ-9 scale produced a single underlying construct of depression (Kroenke et al., 2001), however, subsequent investigations in the United States have reported mixed results regarding the scale's factor structure (Krause et al., 2010; Richardson and Richards, 2008). A single or two factor structure have been reported in a systematic review from 43% of validation studies of language-specific-version of PHQ-9 in LMICs (Carroll et al., 2020). Rigorous psychometric evaluation of PHQ of mental health issues in OF patients is warranted for reliability, validity, and its culturally suitability in Nigeria. This is because the psychometric properties are critical to public health planning and intervention efforts owing to its ability to precisely identify unobserved but inherent constructs of mental issues and their related sub-characteristics. Hence, this study aimed to investigate the psychometric characteristics of the PHQ 9 scale among patients of OF and to validate them against some externally influencing factors.
Methodology
This study was part of a cross-sectional study on determination of the fertility desires and mental health of patients with obstetric fistula in selected health facilities in North Western Nigeria
Sample size and sampling technique
The minimum sample size of 420 was estimated by Leslie Kish sample size formula for determining single proportion for descriptive studies. A two-stage sampling method was used to select the sample population at the centers. Firstly, three OF repair centers at Zaria, Gusau and Sokoto were selected by balloting from the pool of ten centers in the north western zone. From a register of patients’ record in the selected center, proportional sampling was conducted to produce an estimate of the number of patients to be interviewed in each fistula center. At each of the ward and clinics of the repair centers, systematic sampling was then used to determine the number of patients needed after identifying an appropriate sampling interval. A response rate of 100% from the 420 participants approached for the study The inclusion criteria used in recruiting participants are: fistula patients attending the clinic for consultation (prior to surgery); follow up fistula cases after repair surgery and patients on admission at the fistula rehabilitation centers.
Data collection procedure and instrument
Data collection was done using a pretested semi-structured questionnaire. The one-hundred (110) items questionnaire which was developed in English language and translated into Hausa language was interviewer administered between the months of September - November 2014.
Assessment of the mental state of the patients was determined by the PHQ-9 mental health questionnaire Kroenke et al. (2001). A four-point Likert scale options of , “Not at all”, “Several days”, “More than half the days” and “Nearly every day” were assigned to the items of the scale which were scored and coded as “0”, “1”, “2” and “3” respectively.
Data entry of collected questionnaire were entered into IBM SPSS packages that was also used in computing the comparative analysis. Maximum likelihood analysis was conducted in r-statistical packages on Varimax orthogonal rotation. Eigen values of factors greater than 1 were retained and their percentage and cumulative variances were recorded. For this study, the validity tests of measure sampling adequacy were first performed to confirm that collected data have patterned relationships. The factorability of data on these parameters particularly KMO(MSA) whose value range from 0 to 1 and significant value of 0.5.
The maximum likelihood factor analysis is an extraction method that allows for partitioning of the shared variance of a variable from its unique variance and error variance to reveal the underlying factor structure so that only shared variance appears in the solution (Olarenwaju et al., 2020).
Respondents’ sociodemographic characteristics
Respondents age range was between 13 to 55 years having a mean and standard deviation of 26.4±8.4 years and 60% ageing between 20-25 years. Those married had a 45% population while 47.1% were divorced and majority (73.6%) reported being in polygamous marriage union. More than half (55.5%) main occupation was trading and a vastly majority (89.8%) earned a living of NGN4500 or less monthly.
Result of factor analysis
The Kaiser-Meyer-Olkin Measure of Sampling Adequacy (MSA) analysis yielded 0.62 value and the ML analysis produced three factors that constitute 28.0%, 21.5% and 17.6% of the total variance of correlations which as well as 67.1% in aggregate cumulation. Fig 1.

Figure 1: Number of factors produced from the Patients’ Health Questionnaire (PHQ-9) factor analysis.
Internal and construct validity of the PHQ-9 scale
The first factor extracted by the analysis composed of four items of the PHQ-9 scale (Q57, Q59, Q60, Q61) which correspond to somatic construct of a factor correlation that ranged 0.72-0.82 and a Cronbach alpha reliability of 0.86. The second factor produced was non-somatic construct from three items of Q62, Q63 and Q64 which has a correlation range of 0.64-0.91 and Cronbach alpha reliability of 0.77. The third factor emerged from scale items of Q58 and Q65 having a factor correlation coefficient that ranged between 0.64-0.96 and a Cronbach alpha value of 0.74. The overall Cronbach of the scale is 0.66. Table 1.

Table 1: factor structure of PHQ-9 and constructs reliability coefficients
External validity
The standardized mean scores of domains of PHQ scales were assessed against independent variables of socio-demographic characteristics and
some obstetrics risk factors of study participants. Those who were greater than 25 years in age, the singles/divorce and widows had statistically significant difference with higher scores of the construct of affective construct of the PHQ scales (0.39±0.96; 0.11±1.03; 0.11±1.03). p<0>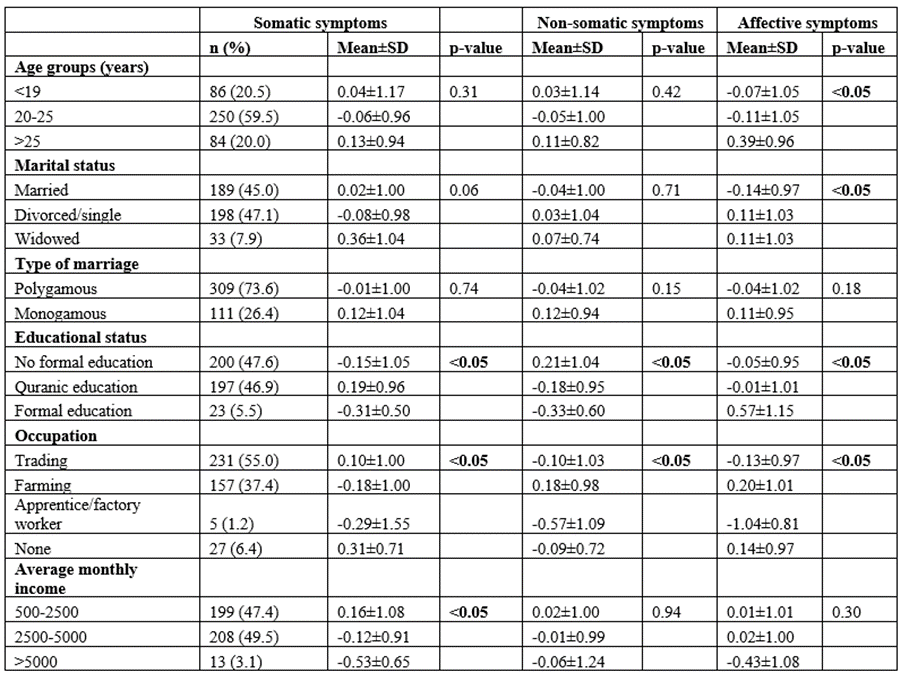
Table 2: Comparative mean analysis of socio-demographic characteristics of patients and the standardized mean scores of constructs in PHQ-9 scale
With respect to levels of education women who had no formal education had significant difference with high scores of PHQ scale construct of non-somatic symptoms (; those who had qur’anic education had statistical difference with the somatic l symptoms construct and those who had formal education statistically differed with life affective symptoms of the scale (0.21±1.04; 0.19±0.96; 0.57±1.15). p<0>
There are statistical differences between the category of the women’s occupation and somatic symptoms domain scores of the PHQ scale among those not working (0.31±0.71). p<0>
There is an insignificant difference between increasing construct scores of somatic symptoms of the scale with women who either got pregnant once or had more than four pregnancies. p<0>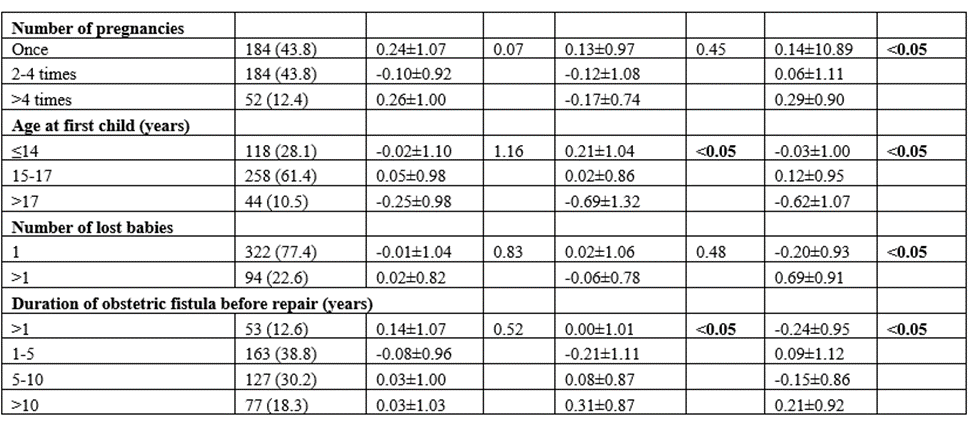
Table 3: Comparative mean analysis of socio-demographic characteristics of OF patients and the standardized mean scores of constructs in PHQ-9 scale
Women who had their first child under or at 14 years of age statistically differed with non-somatic PHQ-9 constuct while those who were between 15-17 years statistically varied with high scores of affective symptoms’ construct (0.21±1.04; 0.12±0.95). p<0>
This study psychometrically examined the quality of life of fistula patients using the patient health questionnaire tool.
Construct validity
This study reported three constructs of somatic, non-somatic and affective symptoms in the exploratory factor analysis of PHQ-9 instrument assessed on VVF patients. According to previous studies, items of the PHQ-9 tool having good internal reliability thematically coalesce under non-somatic and affective symptoms’ constructs (Nduka et al, 2023; Kayondo et al., 2011). However, the items aggregating under somatic construct were perhaps indirectly precipitated from the other factors of non-somatic and affective symptoms. This is because there is dearth of literatures supporting the somatic symptom items of the construct as correlates of experience of VVF patients. Although, general information regarding the potential impact of psycho-social problems on anorexia and insomnia may be available yet this may not be specific to VVF patients but can be relevant to understanding the broader context. It is important to note that while the factors inherent in mental health of VVF patients may impact their physical health, the specific relationship between these factors and anorexia and insomnia in VVF patients may vary depending on individual circumstances. Public health intervention based on the identified construct is highly recommended based on the fact that challenges associated with OF condition have an indelible effect on the mental health of patients even after surgical intervention. According to a study in Malawi, survivors still experience difficulty in proper communal reintegration, childbearing, conjugal relation, and community activity participation aspects (Singh et al, 2015). Hence, mental health rehabilitation of OF patients into their roles could be one of the critical avenues to restore women into their reproductive and family roles.
External validity
This study found respondents of 25 years and above to have significantly rising scores of the affective construct of the PHQ scale. Affective symptoms could arise in individuals with VVF due to the significant impact the frequent occurrence of the condition is having on their quality of life and self-esteem. Regarding the rising ages of greater than 25 years, it's important to note that VVF can occur in women of any age, but certain factors may increase the risk. These factors include prolonged obstructed labor during childbirth, particularly in areas with limited access to medical care or skilled birth attendants. In such cases, older women may be more prone to VVF due to factors like age-related changes in the pelvic anatomy, reduced tissue elasticity, or pre-existing medical conditions (Gharoro et al, 2009; Delamou et al, 2021). In this study the single/divorced women as well as widows reported significant correlation to high scores of the affective symptoms’ construct of the PHQ. The clinical issues associated with fistula such as urine leakages, offensive odour and childlessness could make women to remain single or become divorced (Nweke et al, 2017). High rate of divorce due the condition of VVF have been reported in studies conducted in Zambia and Nigeria (Goh et al, 2005; Ibrahim et al 2000). The fact that this present study found divorced participants to have higher scores of affective disorders than the married is supported by previous findings of Weston et al (2005) and Zeleke et al (2000). The psychological condition may be triggered by a combination of social and domestic stigma as well perceived inability to accomplish marital obligations (Ahmed et al. 2007; Nweke et al, 2017).
Respondents who had Quranic education and those who had no formal education were found to consecutively and significantly correlate with somatic and non-somatic constructs of the PHQ scale. The extensive diversity in the quality of education across sub-Saharan Africa implied that women who develop fistula belong to the most socio-economic and educational disadvantaged in a society (Maheu-Giroux et al, 2016). The correlation between those who had formal education with the affective symptoms construct could be explained by the issue of early marriage among VVF patients; a common phenomenon to the location of respondents in this study. The variables of occupation and monthly income had statistical contrast with the PHQ scale’s derived factors. Respondents who are jobless, those into farming and those earning ≤2500-naira monthly’s significant differences with at least one construct of the PHQ scale in this study underscore the fact that poor socio-economic characteristics of rural women are risk factors for VVF. A study conducted in Northern Nigeria identified low socioeconomic status as one of the underlining factors that characterize VVF patients (Melah et al, 2007). A Tanzania study also reported that VVF patients are essentially farmers who would be 50% more economically impoverished by losing their job after sustaining the injury (Wall, 2006; Pope et al, 2011). This study found significant differences between characteristics of age at first birth, number of pregnancies and number of children birthed with the domains of the PHQ scale. Those who had first child at 14 years had higher scores of non-somatic. The 15-17 years old respondents, those who had more than four pregnancies and those who had greater than one stillbirth had higher scores in affective symtpoms construct of the PHQ scale. Early marriage is a predisposing factor in unfavorable maternal and infant outcomes due to biological, economic social unpreparedness of very young mothers to handle parental responsibilities. Child marriage and childbearing at a young age are drivers of outrageously high incidence of obstetric fistula and it’s attending mental issues (Bello et al, 2020). Africa owns a record of 42% of married under 18 girls whilst Nigeria account for the highest girl-bride population of 23 million in the world leading to sexual experience and activity for a very immature group of persons (UNICEF, 2018). The often-predictable consequences of pregnancy, deaths during childbirth, stillbirth and living with VVF and its psycho-social complications in Nigeria as a whole are associated with being married at an early age in Northwestern and Northeastern regions (NPC, 2019; UNICEF; 2018; UNICEF, 2015; Erulkar, 2007).Women who had reparative surgery more than ten years after occurrence of fistula statistically differed with raised scores of non-somatic and affective symtoms constructs of the PHQ survey. The delay in having fistula repair has been attributed to a current huge backlog of women requiring fistula repair due to limited number of fistula surgeons and delay in training programs of others (UNFPA, 2003). This could worsen VVF patients physiological and mental related symptomatic experience. There are evidences of inequitable allocation of social resources for women, access to maternal health care and reproductive rights which combinedly constitute fundamental factors in the cause of obstetric fistula prevention. These were because of the gap in the commitment of the Nigerian constitution, justice environment National obstetric fistula policy of 2011-2015 (Amodu et al, 2018).
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
