
case report | DOI: https://doi.org/10.31579/2690-4861/595
1Departments of General surgery Chi-Mei Medical Center, Tainan, Taiwan.
2Department of Nursing, Meiho University, Pingtung, Taiwan.
*Corresponding Author: Han-Kun Chen MD, Departments of General surgery Chi-Mei Medical Center, Tainan, Taiwan.
Citation: Han-Kun Chen, (2024), Protective Ileostomy Complicated by Diffuse Pneumatosis Intestinalis of the Gastroenteritic Tract: A Case Report, International Journal of Clinical Case Reports and Reviews, 19(5); DOI:10.31579/2690-4861/595
Copyright: © 2024, Han-Kun Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 28 October 2024 | Accepted: 13 November 2024 | Published: 18 November 2024
Keywords: Ileostomy; pneumatosis intestinalis; portal venous gas; bowel ischemia
Pneumatosis intestinalis (PI) with portal venous gas (PVG) are unusual gas in the bowel wall and hepatic portal venous system. They are rare conditions and usually mean ischemia bowel disease. Therefore, abdominal surgery (such as exploratory laparotomy or laparoscopic surgery) is highly suggested for both examination and treatment effect. A 47-year-old woman here underwent low colorectal surgery with protective ileostomy. Diffuse PI and portal venous gas were found at postoperative day 9. The non-operative therapy was done and she was discharged without abnormal abdominal lesions 12 days after admission. That PI could be ileostomy-stimulated was proved herein. Additionally, conservative treatment alone could be considered alternative on account of likely lesion resolution.
Ileostomy is a common method in colorectal surgery for temporary fecal diversion if the anastomotic leakage probability is high [1] and, nonetheless, not absolutely safe. The severity of ileostomy-connected complications, such as bleeding, retraction, prolapse, stenosis, skin excoriation, parastomal hernia and electrolyte imbalance, in the literatures [2,3,4] is from slightly morbid to life-threatening. The infrequent complication, diffuse gastroenteritic tract Pneumatosis intestinalis (PI) after the protective ileostomy, was indicated hereby, besides the pathogenesis, management and prevention for this complication.
A female aged 48 years underwent neoadjuvant radiotherapy for the rectal adenocarcinoma preoperatively and low anterior resection for the tumor one month afterward after complete radiotherapy. Because of the very low colonic anastomosis and the previous radiotherapy, the ileostomy coincided for fecal diversion. Primarily, her postoperative recovery was smooth. After her oral intake without any discomfort, she was discharged after post-op day 7. Withal, she returned to our hospital due to persistent vomiting, progressive abdominal pain and abdominal bloating after she discharged 2 days afterwards. Physical examination averred abdominal bloating and hypoactive bowel sound but no peritoneal sign. Notwithstanding the severely edematous ileostomy, no gangrene change existed; sepsis, leukocytosis (WBC: 19400/mL), metabolic acidosis, and elevated lactate levels (7.5 mmole/L) were evinced. The abdominal computed tomography (CT) from the stomach to the small bowel denoted diffuse dilatation (Figure 1) and pneumatosis intestinalis (PI) and portal venous gas (PVG) (Figure 2, 3). Owing to these symptoms, she was admitted in our intensive care unit for advance treatment. Non-operative treatment because there was no peritoneal sign and the ileostomy was still in good appearance. Those treatments covering nasogastric tube (NG) for gastrointestinal (GI) tract decompression, large amount fluid supply (3000ml/day) and antibiotics (ceftriaxone 1gm Q12H and metronidazole 500mg Q8H) was for her sepsis status. Her abdomen and ileostomy conditions scrutinized could be contributed to emergent operations if getting worse. The edematous ileostomy started to improve two days subsequently. The ileostomy-made flatus and stool passage were on readmission day 5. The oral liquid diet ingestion began; the transfer to the general ward was on re-admission day 7. Attributed to no abnormal abdominal lesion, the soft diet was applied. Eventually, she was discharged on re-admission day 12. Till present, no other abdominal lesion was identified in out-patient department follow up.
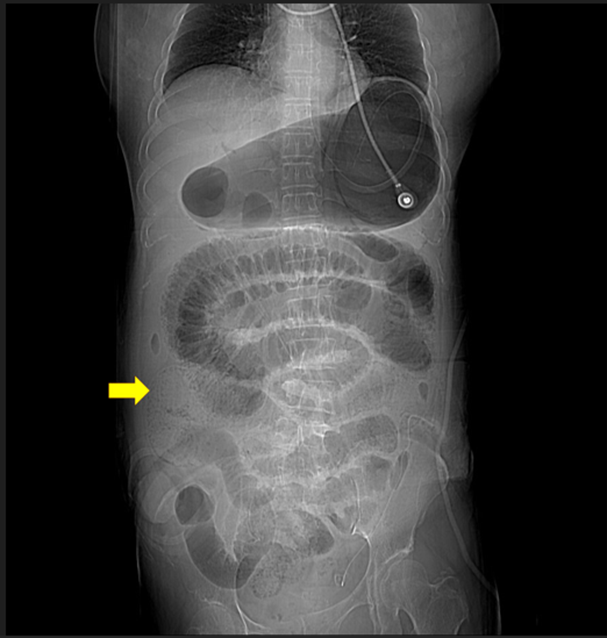
Figure 1: Diffuse dilatation from stomach to small bowel, the dilation of bowel end at ileostomy (arrow)
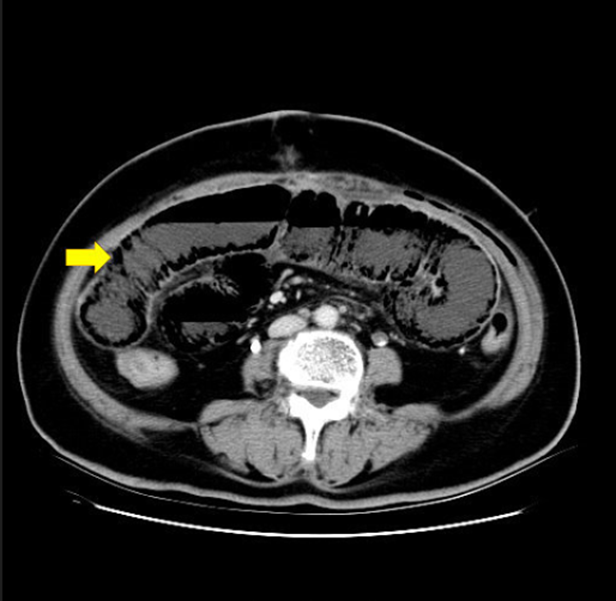
Figure 2: Dilated bowel with intra-mural gas (arrow)
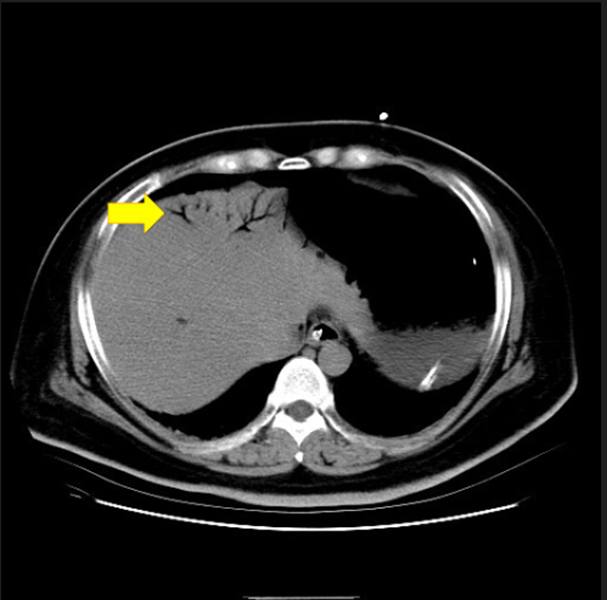
Figure 3: Portovenous gas (arrow)
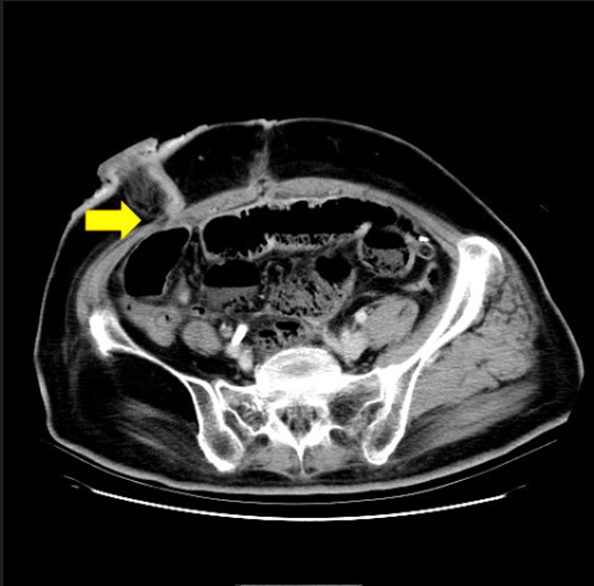
Figure 4: Narrowing orifice of fascia at ileostomy (arrow)
Ileostomy, an important procedure in emerging and electric colorectal surgeries [2], could be temporary or permanent treatment for bowel decompression or fecal diversion; a routine fashion for protecting a distal colonic anastomosis [1]. Still, some complications such as bleeding, retraction, prolapse, parastomal hernia, skin excoriation, stenosis, electrolyte imbalance and death were declared [3,4]. Our patient had a rare complication related with severe PI and PVG. PI, a specific radiology phenomenon, was Lerner and Gazin-described first in 1946 [5]. Two mechanisms supposedly increased intralumenal pressure and mucosal injury were supposed [6]. The former in view of bowel obstruction, paralysis, or iatrogenic trauma induced that gas dissected into the bowel wall from the intestinal lumen. The latter was in virtue of bowel ischemia, inflammatory, infection, graft-versus-host disease, connective tissue diseases, radiochemotherapy or emphysema [6,7]. Loosely, PI related bowel damage could be classified: non bowel damage (emphysema), slight mucosal injury (enteritis) and severe bowel damage (ischemia or necrosis) [8, 9]. Some reports mention that PI combined PVG associated with transmural bowel infarction and high mortality rate [10]. Because severe bowel damage is life-threatening, it is necessary that well differential diagnosis and applicable therapy for PI. Most surgeons agree the surgical management in severe bowel damage. Greenstein [11] proposed a management algorithm by a retrospective study. If symptoms of obstruction, leukocytosis, sepsis, and PVG and high lactate levels appear, surgery is highly recommended. This patient had obstructive signs, sepsis, high lactate levels, and PVG-combined PI; hence the surgical intervention was Alexander’s management algorithm-announced. However, we found that bowel dilatation was terminated at the ileostomy (Figure. 1). In outward appearance, the ileostomy became edematous. By the digital examination of the opening of the ileostomy and the CT finding (Figure. 4), the proximal opening of ileostomy narrowing was noted. Meanwhile, her dehydration was caused by large amount watery-content stool via the ileostomy. These appearances led to GI tract obstruction, increasing intra-luminal pressure, decreasing the bowel wall blood supply and diffuse PI with PVG formation finally. Wolthuis et al. affirmed a similar case with local PI-associated post needle catheter jejunostomy (NCJ) [12]. The non-operative methods styles such as the NCJ removal, NG decompression and broad-spectrum antibiotics were provided. In our patient, the protective ileostomy could not be removed by non-operative method. Because the ileostomy is the end of the bowel with PI, its mucosa appearance can be used to observe the bowel conditions. So we closely follow the ileostomy condition and used non-operative management as Wolthuis’ method. After the ileostomy edema reduced and flatus passed, her abdominal problems were recovered. After the ileostomy edema reduced and the flatus passed, her abdomen recuperated. The outcome was good after this non-operative management.
The diffuse PI is a rare complication of ileostomy, which could be induced by inordinate narrowing of the ileostomy orifice; accelerated by much watery stool via the ileostomy. Conservative treatment comprising NG for decompression, large amount fluid supply, broad-spectrum intravenous antibiotics for sepsis, and closely monitoring the ileostomy and abdominal condition could be regarded as optional by reason of plausible lesion resolution.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
