
Case Report | DOI: https://doi.org/10.31579/2693-2156/012
1 Resident, Cardio-Vascular Surgery Program, Pontificia Universidad Javeriana, Bogotá, Colombia.
2 Cardiovascular Surgery Unit, Hospital Universitario San Ignacio. Assistant professor, School of Medicine, Pontificia Universidad Javeriana, Bogotá, Colombia.
3 Head, Cardiovascular Surgery Unit, Hospital Universitario San Ignacio. Assistant professor, School of Medicine, Pontificia Universidad Javeriana, Bogotá, Colombia.
*Corresponding Author: Edgar Giovanny Ríos Dueñas, Resident, Cardio-Vascular Surgery Program, Pontificia Universidad Javeriana, Bogotá, Colombia.
Citation: Sergio Alzate, Edgar G. R. Dueñas, Juan R Correa (2020) Prosthetic endocarditis, clinical and surgical insights of life-threatening situations. J Thoracic Disease and Cardiothoracic Surgery, 1(3); DOI:10.31579/2693-2156/012
Copyright: © 2020 Edgar Giovanny Ríos, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 June 2020 | Accepted: 20 July 2020 | Published: 01 August 2020
Keywords: aortic valve prostheses; surgical aortic valve replacement; prosthetic endocarditis; postoperative complications; prosthesis-related infections
Prosthetic valve endocarditis (PVE) is a low incidence microbial infection complicating surgical valve replacements with a very high rate of early mortality. We present a series of 5 patients who required redo surgical interventions due to PVE as a complication within the first 3 postoperative months. Initial procedures included aortic valve replacement with valved graft conduit or supra-coronary graft, isolated or combined aortic and mitral valve replacements. The diagnosis was established by transesophageal echocardiogram and computed tomography angiography. Complex surgical procedures under hypothermic femoral access cardio-pulmonary by-pass techniques for prosthetic valvular replacements with homografts, biological or mechanical valves are described. Mortality was 40%.
Prosthetic valve endocarditis (PVE) is a rare surgical complication, its worldwide incidence ranges from 1% to 4% per patient year [1]. Despite improvements in various fields of cardiac surgery, PVE still poses a serious threat to life in cardiac valve surgery patients. PVE mortality rates increase as serious situations ensue along within the clinical spectrum of an ominous postoperative infection [2,3]. Heart failure is associated in up to a 56% of PVE cases, hemorrhagic stroke appears in 42% of patients with ictus [4,5] . PVE mortality rates soared 60% by 1970, by the beginning of the millennium declined to 22% and by 2017 it has been documented to be between 15% - 20%, one year mortality is 40% [3,6,7]. Bad prognosis risk factors include advanced age, diabetes, nosocomial origin of infection, Staphylococcus sepsis and intracavitary abscess [8].
The main clinical manifestation is fever in close to 90% of patients with PVE. At physical exam it is possible to hear a new appearance heart murmur, heart failure signs, AV conduction blockages and systemic arterial embolisms (AMI, stroke, splenic infarct, GI ischemic) [9,10]. Time from surgical procedure to clinical debut is variable. Early presentations (within the first year) happen in up to 77% of cases, these are associated to blood borne spread of intraoperative or early postoperative infection, later infections appear to be caused by invading microbes adherent to surgical sutures or devices [7, 11]. Most frequent causing microorganisms in early presentations are Staph. Aureus (15% - 36%), Coag. Negative Staph. Spp (17% - 45%), Enterococci spp (14%), Gram (-) bacilli (10%) and fungi (6%), later infections are caused most frequently by Streptococci spp [7,12].
Literature has shown that early surgical intervention is associated with a lower rate of further complications and a higher probability of preserving the prosthesis, nonetheless this approach will depend on a timely diagnosis not always available due to unclear clinical presentations. Late diagnosis is associated with higher probability of prosthetic valvar damage, annulus involvement with abscess and fistulae formation, septic embolism, and multiple organ failure and poor surgical results and prognosis [2, 13-15].
Diagnosis is based on documenting blood cultures (positive in 90% of cases not previously treated with antibiotics), presence of vegetations on echocardiogram, perivalvular abscess or leakage, dehiscent sutures, annular involvement, systemic emboli or multiorgan failure [2, 6, 16].
The importance of a timely diagnosis relies on prompt specific antimicrobial therapy in order to prevent the aforementioned complications, in most cases it is highly recommended to maintain it up to six weeks8. Opportune surgical intervention is indicated in patients presenting with valve dysfunction, heart failure, emboli generating or bulky vegetations, quick abscess formation, persistent positive blood cultures or uncontrolled sepsis often caused by Staph aureus or fungi. Mainstay of surgical intervention is removal of all potentially colonized prosthetic tissue (valve prostheses, grafts, sutures) along with ample debridement followed by adequate prosthetic valve substitution and continued antimicrobial therapy [18, 19]. Should other systemic abscesses of embolic origin be present, they must be addressed before or at the time of the cardiac procedure.
Thirty-day mortality has been reported to range from 13% in rather benign situations and could raise up to 30%-40% in patients with multiple risk factors. Additional 26% mortality is added for the first year of follow up [20]. The benefit of septic control by type of the new prosthetic replacement device used is highly debatable but homografts and stentless bioprostheses may provide with less frequent evidence of continued infection [21].
Followed, we summarize insight related to presentation, surgical and medical management and outcome in five PVE cases since 2017. These patients developed valve graft endocarditis as an early complication (within 3 months after surgery) after procedures such as aortic replacement with valved conduits and reimplantation of coronary arteries, single aortic and mitral valve replacements and mitral valve replacement along with ascending aorta Dacron graft interposition plus two vessel myocardial revascularization at a Latin-American university hospital.
Case 1.
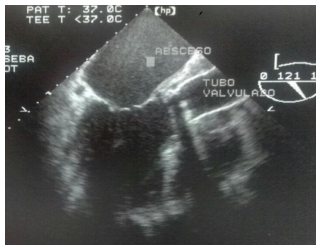
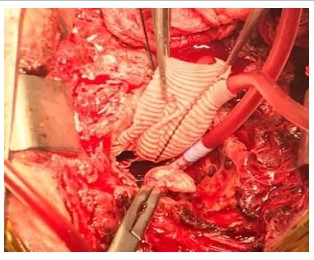
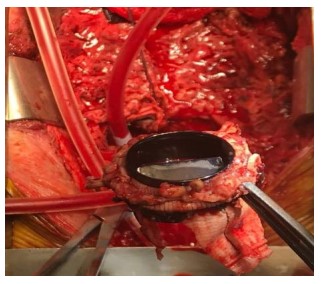
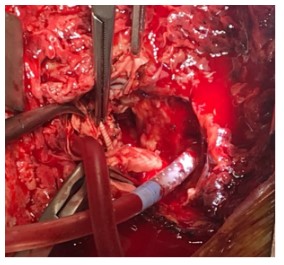
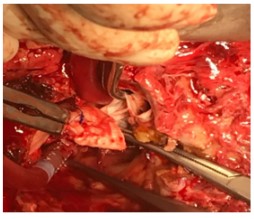
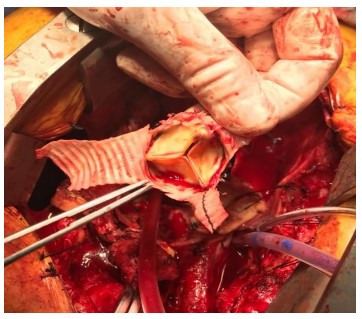
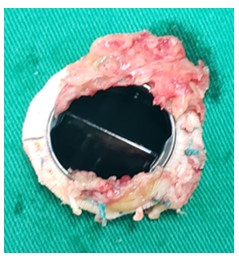
A 42-year-old male patient with Marfan’s syndrome was admitted to the hospital due to heart failure and echocardiographic evidence of ascending aortic aneurysm and severe aortic valve regurgitation, his BMI was 37 at admission. He underwent an uneventful seven-day hospital stay aortic valve replacement with a 25-mm bileaflet mechanical valve conduit along with coronary ostial reattachment. At two weeks after the operation he presents redness, swelling in the sternotomy wound and low-grade fever. After obtaining a non-relevant trans-thoracic echocardiogram he was placed in oral cephalosporin with a superficial wound infection diagnosis. Two months later he is admitted with a rampant febrile course, Staph. Aureus MSSA and an unclear thickening around the vascular graft and a normal echocardiogram. He received specific oral antimicrobial therapy. Three weeks later he developed a rapid onset septic shock requiring inotropic and vasopressor therapy along with mechanical ventilatory support. Thoracic Angio CT revealed a frank collection surrounding the aortic graft, prosthetic valve annular leak and a distorted mobile graft. On TEE a 30% circumferential dehiscent valve was found (Fig 1). Emergency reoperation was performed by femoral vascular access on-pump sternotomy at moderate hypothermia. Aortic cross clamping was made possible and selective ostial Bretschneider´s cardioplegia delivered. Preoperative findings were confirmed with massive annular infective destruction (Fig 2-3). Homografts were unavailable at the moment of the operation. Decision was made for the use of a new 25-mm mechanical bileaflet valved conduit with redo coronary reimplantation. Independent prosthetic valve pledgeted sutures needed to be mattressed against a Dacron felt along de right ventricle edge of the aortic annulus. At weaning from CPB with acceptable ventricle function dire efforts to stop bleeding were made but progressive dehiscent right ventricle outflow tract stitches made it irretrievable. Patient was pronounced dead at OR.
Case 2.
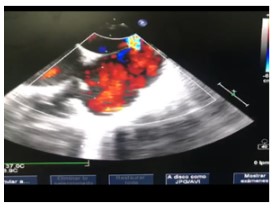
A 32-year-old dysmorphic 1.5m2 BSA woman with severe dysplastic AS underwent a 21-mm mechanical valve replacement. Genetic workup ruled out 45-X chromosome deletion. She had a six day course unremarkable hospitalization. At two weeks postoperative, erythema, heat and watery discharge was observed in the lower third of the sternotomy wound. An unrevealing TTE was obtained and MSSA was isolated from wound secretion. She was given oral dicloxacillin and ambulatory wound care management. Three weeks later she is admitted to the emergency room with a severely bleeding dehiscent sternal wound. Angio-CT and TEE showed fluid collection anterior to the distal ascending aortic wall along with an extensive substernal hematoma. Blood cultures revealed MSSA. Surgical management was planned so a redo sternotomy was made under femoral access hypothermic cardiopulmonary by-pass. After a difficult evacuation of a massive mediastinal hematoma and liberation of adhesions two aortic rupture sites were identified. Original aortic cannulation site and aortotomy closure suture line were dehiscent. Distal ascending aortic cross clamping was achieved and selective ostial Bretschneider´s cardioplegia was given. The valve leaflet appearance and mechanics, annulus and sutures were observed without any abnormalities, so no valve prostheses replacement was considered. A supra-coronary ascending aortic replacement was performed using a Dacron graft (Fig 4-5). Open chest packing for coagulopathic state was made and sternal closure was done at 48 hs. She had an initial fair course for the following six weeks under IV antibiotics to be discharged in good condition. Two months later she presented to ER with embolic left hemispheric stroke, admitted to ICU in vasoplegic shock. Angio-CT and TEE reveal a 2 cm aortic prosthetic vegetation at the ventricular side along with a lesser size vegetation at the interatrial septum left atrium. Due to cerebral hemorrhagic transformation immediate third time operation was deemed unadvisable. After six days under IV antibiotics, inotropic/vasopressor support, mechanical ventilation and brain preserving measures a rather stable course with normal left ventricular function, shock control was obtained. TEE reveals persistent vegetations and a LV to RA fistula was observed (Fig 6). Reoperation was decided. A hostile mediastinum was approached via femoral cannulation on-pump moderate hypothermic sternotomy. An acquired infective LV to RA fistula was confirmed along with prosthetic vegetations. Extensive debridement including the affected septal wall and prosthetic valve excision was done. Reconstruction was obtained by using a Dacron patch for repairing the septal defect and a 21-mm bovine pericardium bioprostheses for valve replacement. A new aortic Dacron graft was interposed. The patient was weaned from CPB and taken to ICU under open-chest-packing low vacuum assisted wound coverage. After a week with four chest debridement/lavages mediastinal samples kept MRSA growing along with blood cultures with Acynetobacter baumanii and Candida albicans which prompted a use of wide range antibiotic and antifungal association. The patient evolved towards a poorly controlled septic shock. Without certainty about her CNS prognosis, humanitarian end of therapeutic effort was advised and followed by her relatives.


Case 3.
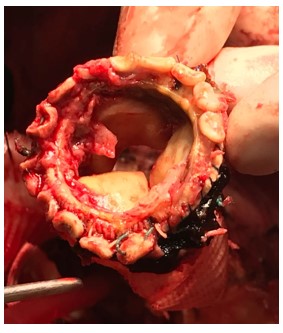
A 61 year-old malnourished male presented to ER with chest pain due to a Stanford A acute aortic dissection involving the left iliac artery. An ascending aortic and valve replacement was performed with a 23-mm mechanical valve conduit under right femoral access hypothermic CPB. Open distal ascending aortic anastomosis was carried out under retrograde cerebral perfusion. He developed a postoperative complete AV block prompting implantation of a permanent bicameral pacemaker. At two weeks from the initial procedure he developed a febrile course. As blood cultures were positive for E. coli and Strep. faecalis he was placed on IV specific antibiotics for 6 weeks and discharged with a normal echocardiogram. Three months later he is readmitted with a rapidly evolving febrile course towards a septic shock. Angio CT-scan and echocardiogram showed peri-aortic collection connecting with the ventricular cavity along with a huge annular abscess, peri-valvular leak and pacemaker lead vegetations. Blood cultures were positive for AmpC Serratia spp. So specific antibiotics were started. Reoperation was advised immediately. Redo sternotomy was performed under ready right femoral access cannulation. A nearly 50% circumferential annular dehiscence of the valve prostheses was found feeding a large septic pseudo-aneurysm (Figs 7-8). Distal graft cross clamping was secured to achieve HTK cardioplegia delivery and hypothermic arrest in order to perform open distal anastomosis. The entire conduit was removed and thorough debridement of inflammatory tissue performed. Suitable homografts were unavailable at the time of the operation. A 23-mm diameter new mechanical valve conduit was interposed along with coronary reattachment. Open chest strategy was used and after four surgical lavages in alternating days the sternum was closed. The patient exhibited a tortuous evolution due to septic shock tan granted IV antibiotics for 8 weeks until full recovery. He was discharged on day 64. At one year postoperative follow up control shows no clinical nor echocardiographic evidence of continued PVE.
Case 4.
A 67 year-old male otherwise health patient complaining of shortness of breath was referred to our unit with evidence of aortic valve stenosis/regurgitation, aortic root dilatation, severe mitral regurgitation, chronic AF and LVEF 29%. He underwent ascending aortic and valve replacement with an in-site tailored 25-mm bovine pericardium valved conduit and a 29-mm porcine prosthetic mitral valve replacement. At second postoperative week, he was readmitted with evolving evidence of deep wound infection and bacteremia due to Strep. faecalis and AmpC pattern M. morgagnii. After obtaining irrelevant angio CT and echocardiogram he was placed on IV antibiotics for 28 days. At two months postoperatively he is brought back continuously hyperthermic. A new set of angio CT-scan and TT echo were obtained without disclosing any graft or prosthetic issues. Antibiotics are advised to be prolonged for 8 more weeks. A PET CT-scan performed a week after angio CT-scan and TT echo revealed enhanced activity at sternum, mediastinum around graft areas and aortic annulus. A new TE echo revealed an annular detachment of the aortic graft prostheses with systolic collapse and a normally functioning mitral valve prostheses. Angio CT confirms a severe annular leak and pseudo-aneurysm. Surgical plans included homograft interposition. Operation included redo sternotomy under CPB via femoral cannulation under moderate hypothermia. A severely damaged Dacron graft and a detached valve prostheses were found (Figs 9-10). Aortic cross clamping granted HTK cardioplegia delivery and on-clamp distal anastomosis of a 24-mm aortic homograft along with a coronary reimplant were accomplished (Fig. 11). The mitral valve was inspected and found to be free on inflammatory process. At CPB weaning evidence of cardiogenic shock and EKG abnormalities lead to diagnosis of right coronary ostial damage, a proximal saphenous vein graft interposition was made. Open sternal strategy with low vacuum assisted wound coverage and sequential lavages granted thoracic closure at eighth postoperative day. After six weeks of ICU management under IV antibiotics he was transferred to surgical ward where he received rehabilitation therapy to be discharged on day 78. At one year postoperative follow up this patient has no clinical, bacteriological nor imaging evidence of homograft/mitral prostheses endocarditis.

Case 5.
A 43-year-old malnourished woman under chronic steroid usage for advanced RA became symptomatic for heart failure. Severe aortic valve insufficiency and a 48-mm dilatation of the tubular portion of the ascending aorta were diagnosed. A 25-mm mechanical valve and 28-mm Dacron supra-coronary aortic graft interposition were performed. After a prolonged hospital stay due to superficial sternal wound dehiscence, she was discharged on P.O. warfarin. Three months later she is admitted in septic shock due to MSSA. Angio CT-scan and TE echo revealed a peri-prosthetic abscess surrounding the graft and vegetations impinging on valve mechanism. Surgical intervention was recommended, and homograft availability obtained. CPB via femoral access cannulation was established and temperature lowered to 24 Celsius. Aortic cross clamp and HTK cardioplegia followed. Half circumferential proximal anastomosis suture line dehiscence and valve septic thrombi were found (Fig 11). Valve prostheses and Dacron graft were totally removed. Coronary ostia were prepared for direct implantation and a 24-mm aortic homograft was placed. Open mediastinum and low vacuum wound coverage/surgical lavages strategy was followed. After 8 days sternal closure was completed with negative wound/blood cultures. IV antibiotic therapy was continued during six additional weeks to be discharged home on day 75. At nine postoperative months she continues with no evidence of valve endocarditis.
PVE is a rare complication that may appear early or late after surgery. In our 3-year case series, we identified five cases resulting in a 3.2 patient/year incidence, similar to that reported in the literature. All cases were early PVE presentations. Some cases may clearly relate to predisposing preoperative factors such as malnourishment and immunosuppression. Although congenital syndromes and malformations are not clearly associated as a predisposing factor for postoperative infections we registered two patients with phenotypical abnormalities.
Angio CT-scan and transesophageal echocardiography are reported as first choice for diagnosis, albeit TSE sensitivity (82-95%) and specificity (94%) along with CT sensitivity (88-97%) and specificity (95%),6,27 they may not reveal clear findings due untimely use in a highly rapid evolving situation. In the reported cases, both diagnostic studies allowed the confirmation of the diagnosis at different times from onset of symptomatic infective state and detailed structural compromise of the valve and the grafts, extension of the infection, myocardial function and allowed to define surgical planning.
The most common isolated microorganism was MSSA Methicillin-sensitive Staphylococcus aureus (60%) and it is associated with findings of catastrophic valve damage such as annular detachment or leakage, which enforces surgical management for its resolution. Although there are some reported case series of conservative management in patients with prosthetic valve endocarditis, the rates of therapeutic failure are higher when the affected valve is the aortic or when Staph. aureus is the causing organism23,24.
Treatment should be individualized according to each patient´s clinical condition. The mainstays are prompt specific antibiotic management against culture isolated germ and rapid hemodynamic stabilization of heart failure. Aiming to obtain best possible clinical condition at time of surgery is highly desirable but not always possible. The identification of non-cardiac involvement such as stroke, escalates mortality to unacceptable limits. Risk assessment by STS and EuroScore II ratings are essential in advanced cases. Multidisciplinary evaluation (cardiologist, intensivist doctor, infectologist, neurologist and cardiovascular surgeon) is a must to define surgical indication22.
In the present series mortality rate is 40% due to intraoperative or early postoperative causes. Massive bleeding due to irreparable surgical injury or tissue destruction and poor neurological prognosis associated with uncontrolled extracardiac sepsis and stroke were the causes of death. Surgical management with CPB approach thru peripheral cannulation and hypothermia allows entry to a hostile mediastinum cautiously foreseeing bleeding from ruptured pseudo-aneurysms. This approach is considered a standard in all our PVE cases. Two cryopreserved homografts were used for the reconstruction of the aortic root, these allow a larger surface coverage and fitment on thoroughly debrided sites of the affected tissue and may also offer some protective effect in controlling infection25. A viable alternative is the use of bioprostheses which may present a low risk of recurrence of endocarditis26.
Hospital stay for survivors should be expected to be prolonged. In our series an average 72 days included IV antibiotic treatment for at least 6 weeks and associated medical management for other medical conditions as well as for initial rehabilitation purposes.
PVE at a university hospital in Bogota is 3% for the previous 3 years to this report. Five adult cases were registered in three men and two women with ages ranging from 32 to 67 years. All cases included aortic valve replacement and early presentation (earlier than 3 postoperative months). Two patients had predisposing factors for operative infection such as malnourishment and immunosuppression (40%), Marfan´s syndrome and a non-classified dysmorphic trait (40%). Three (60%) patients had superficial wound infection, 1 (20%) deep wound infection and 1(20%) bacteremia as causative event.
Most frequent microorganism was Staph. aureus (MSSA) in three out of five cases, Serratia spp in one, multi-bacterial in one and associated fungi in one. In all patients confirmatory findings of PVE were established by TE echo and angio CT. Those findings encompass peri-valvular leaks, abscess, pseudo-aneurysms, annular dehiscence and vegetations.
Surgical management was performed by redo sternotomy access under femoral cannulation or ready to cannulate, moderate or deep hypothermia, HTK single dose antegrade cardioplegia. All patients required aortic prosthetic replacement: two homografs, two bioprostheses and one mechanical valved conduit. 30-day mortality was 2 patients (40%) due to uncontrollable hemorrhage and septic shock along with severe stroke. Average hospital stay for survivors was 72 days.
Prosthetic valve endocarditis (PVE) affecting grafts is a rare complication, however, it persists as one with a very high mortality risk, besides it poses an immense therapeutic challenge. Early diagnosis and prompt individualized medical and surgical management must be made in each patient.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
