
Research Article | DOI: https://doi.org/10.31579/2768-2757/045
* Center for Advanced Thoracic Surgery, Global Robotics Institute, Advent Health Celebration, University of Central Florida.
*Corresponding Author: Farid Gharagozloo, M.D., FACS, Center for Advanced thoracic Surgery. 400 celebration Place, Celebration, 34786, Florida.
Citation: Farid Gharagozloo and Mark Meyer. (2022). Proposed Pathogenesis for a Subgroup of Patients with Neurogenic Thoracic Outlet Syndrome. J Clinical Surgery and Research, 3(4); DOI:10.31579/2768-2757/045
Copyright: © 2022, Farid Gharagozloo. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 07 March 2022 | Accepted: 16 March 2022 | Published: 24 March 2022
Keywords: : neurogenic; thoracic outlet syndrome (TOS); bony tubercle; first rib; robotic first rib resection
Most patients with Neurogenic Thoracic Outlet Syndrome (TOS) have upper extremity pain and paresthesia with normal neurologic examination and objective tests. The purpose of this study was to determine the pathologic nature of the resected first ribs in a subgroup of patients TOS who experienced resolution of symptoms postoperatively.
Methods: In a retrospective study, we compared normal human cadaver first ribs (control, C) with first ribs from patients with proven NTOS (N). Ribs were examined for anatomic features. Preoperative and postoperative dynamic Magnetic Resonance Angiograms (MRA) of the affected and contralateral upper extremities were examined.
Results: There were 41 first ribs from patients with DNTOS and 12 normal first ribs from human cadavers. In all patients (100%) with DNTOS there was a bony tubercle which corresponded to the area of subclavian vein groove in the normal ribs.
Conclusion: A bony tubercle at the site of the subclavian vein groove in patients with DNTOS may be the pathologic entity which causes extrinsic compression of the subclavian vein at rest. The neurologic symptoms resolve following disarticulation and resection of the medial aspect of the first rib. In a subgroup of patients, NTOS may be the manifestation of venous ischemia of the nerves of the upper extremity as opposed to nerve compression.
Type of Research: Single-center retrospective cohort study.
Key Findings: A bony tubercle at the site of the subclavian vein groove in a subgroup of patients affected with DNTOS is the pathologic entity which causes extrinsic compression of the subclavian vein at rest. In these patients the neurologic symptoms resolve following disarticulation and resection of the medial aspect of the first rib.
Take Home Message: A subgroup of patients with Disputed Neurogenic Thoracic Outlet Syndrome may have neurologic symptoms caused by venous ischemia of the upper extremity which is caused by extrinsic compression of the subclavian vein by a bony tubercle on the first rib at the costo-sternal joint.
Table of Content Summary: This retrospective study compared normal human cadaver first ribs with first ribs from patients with proven NTOS (N). Proof of NTOS was symptom resolution following resection of the medial aspect of the first rib. The study suggests that in a subgroup of patients with Disputed Neurogenic Thoracic Outlet Syndrome, neurologic symptoms caused by venous ischemia of the upper extremity which is caused by extrinsic compression of the subclavian vein by a bony tubercle on the first rib at the costo-sternal joint
In 1956, a group of diverse patients with symptoms in the shoulder, neck, and the upper extremity who presented with pain, numbness, tingling, and swelling, were placed under the umbrella of “thoracic outlet syndrome” (“TOS”) [1]. Since that publication, Thoracic Outlet Syndrome has been classified as Neurogenic, Venous (Paget Schroetter Syndrome), and Arterial varieties. In the past six decades TOS has been characterized by confusion about the actual pathophysiology of the disease, the appropriate diagnostic tests, and the appropriate therapeutic interventions [2, 3]. As a result, further subtypes have been proposed: True neurogenic TOS, Disputed Neurogenic TOS (DNTOS), Traumatic neurovascular TOS. It has been postulated that the common pathologic feature of these conditions is the compression of the brachial plexus and/ or subclavian vessels just above the first rib. Although the role of the first rib seems to be a unifying feature of TOS, the exact mechanism by which the first rib results in compression, and specifically what is compressed, has remained unclear. Furthermore, given the fact that in the absence of rarely seen cervical rib or cervical bands, anatomically the first rib is not in the vicinity of the brachial plexus, the exact role of the first rib in the majority of patients with “Neurogenic” TOS (Disputed Neurogenic TOS) has been an enigma.
Based on the comparison of the resected first ribs from patients with Venous TOS, or Paget Schroetter Syndrome (PSS) and normal first ribs, Gharagozloo et. al. proposed that an abnormal bony tubercle at the costo-sternal joint of the first rib is the pathologic entity [4]. The hypothesis was tested in 83 patients who underwent transthoracic robotic resection of the medial aspect of the rib and disarticulation of the costo-sternal joint with relief of the extrinsic compression of the subclavian vein [5,6]. Two years after robotic resection of the offending portion of the first rib and obtaining patency of the SV, all patients remained asymptomatic and had full function of the affected upper extremity. Unexpectedly, detailed preoperative assessment in these patients revealed a significant history of unrecognized upper extremity neurologic symptoms which predated the clotting of the subclavian vein and onset of Paget Schroetter Syndrome. The neurologic symptoms resolved after undergoing resection of the first rib for PSS. Therefore, it was hypothesized that in a subgroup of patients with DNTOS neurologic symptoms may be a manifestation of compression of the subclavian vein, venous congestion resulting in venous ischemia of the upper extremity nerves which lead to diffuse neurologic symptoms unrelated to nerve compression.
In order to test the above hypothesis, the present study compared the anatomic features of the first rib in normal individuals to the first ribs resected from a subgroup of patients with DNTOS who experienced postoperative symptom relief following the resection of the costo-sternal joint and the medial aspect of the first rib resection.
This study is a retrospective analysis comparing normal human cadaver first ribs (Control, C) with first ribs from a subset of patients affected with “Neurogenic” TOS (N).
First ribs from human cadavers were obtained from individuals without an ante-mortem history of upper extremity symptoms or pathology.
Neurogenic TOS was suspected in patients who had a clinical history of upper extremity, shoulder, and neck pain in whom cervical spine disease, shoulder disease, and other orthopedic conditions were ruled out. Preoperative diagnosis of DNTOS was made after all specific localizing diagnostic findings were ruled out. All patients underwent robotic transthoracic resection of the medial aspect of the first rib with disarticulation of the costo-sternal joint. Definitive diagnosis of DNTOS was made only after the patient experienced complete resolution of symptoms on postoperative follow-up. Only the rib specimens from patients who experienced complete resolution of their neurologic symptoms were included in this study.
The study included postmortem (C group) or postoperative (N group) pathologic anatomic observations, review of the preoperative and postoperative MRA, and review of video recording of the operation. For each rib, the following anatomic observation points were recorded: 1) width of the rib at the costo-sternal junction, 2) the presence of a groove for the subclavian vein, 3) the presence of a groove for the subclavian artery, and 4) the presence of tubercle at the medial aspect of the rib. The preoperative MRA study with maneuvers were examined for the presence of extrinsic compression of the subclavian vein. The area of extrinsic compression on the MRA was then correlated with the anatomic findings. The post-operative MRA study with maneuvers were examined for the presence of extrinsic compression of the subclavian vein. The relationship of the first rib to the subclavian vein was assessed at rest and with elevation of the extremity above the shoulder. The intraoperative videos from transthoracic robotic surgical resection of the first rib were examined for surgical observations in terms of the relationship of the medial aspect of the first rib to the subclavian vein. The anatomic features of the first rib in relation to the subclavian vein were recorded.
Data were exported from Excel (Microsoft Corp., Redmond, WA.). Information was obtained through hospital databases, medical records, and our prospective database. The data was prospectively accrued and retrospectively analyzed. Individual consent was waived for inclusion in this study; however, it was required and obtained to enter patient data in the prospective database. This study was reviewed institutional review board and determined to be exempt under 45 CFR 46.101 (b)
Control (C) Group: There were 12 first ribs obtained from human cadavers in the C group. There were 6 right first ribs and 6 left first ribs in the C group. The ribs in the C group had a thickness of 0.5 +/- 0.1cm at the midpoint of the rib and 1.0 +/- 0.08cm at the costo-sternal junction. All of the ribs in the C group exhibited a groove at the subclavian vein with a thickness of 0.2 +/- 0.04cm. In addition, in all ribs in the C group there was a groove at the subclavian artery with rib thickness 0.2 +/- 0.04cm.
Experimental (N) Group: There were 41 first ribs resected from patients who had the definitive postoperative diagnosis of Neurogenic TOS based on complete resolution of the preoperative neurologic symptoms. There were 29 right first ribs and 12 left first ribs in the N group. The ribs in the N group had a thickness of 0.6+/-0.1 cm at the midpoint of the rib and 1.3 +/-0.4cm at the costo-sternal junction. All of the first ribs in the N group demonstrated a bony protuberance at the site of the subclavian vein groove with a thickness of 1.4 +/- 0.1cm.
In all (100%) patients in the N group, the surgeon reported a bony tubercle just lateral to the costo-sternal joint.
Preoperative MRA with maneuvers of the ipsilateral side in all patients (100%) in the N group revealed extrinsic compression of the subclavian vein at its junction with the innominate vein by a bony protuberance on the underside of the vein. (Figure. 1)

Figure 1: Preoperative MRA with maneuvers in a patient with Disputed Neurogenic TOS. The Arrows point to the extrinsic compression of the subclavian vein at its junction with the innominate vein by a bony protuberance on the underside of the vein.
In all patients (100%), elevation of the arm above the shoulder resulted in greater compression of the subclavian vein by the bony protuberance. The postoperative MRA with maneuvers showed relief of extrinsic compression of the subclavian vein in all patients. There was no statistical difference between the C and N groups in terms of thickness of the rib at its midpoint. The thickness of the first rib at the subclavian vein groove and costo-sternal joint was significantly different between the C and N Groups (p less than 0.05).
In 1956 Peet, attempted to classify patients who presented with a variety of symptoms that affected the upper extremity, the ipsilateral neck and shoulder. Curiously, as a result of Peet’s classification which was based on symptoms rather than the underlying pathology, it was extrapolated that TOS represents a group of diverse disorders that result from compression of the neurovascular bundle exiting the thoracic outlet. Compression of this area has been thought to result in a constellation of distinct symptoms, which can include upper extremity pallor, paresthesia, weakness, muscle atrophy, pain, and swelling [8,9]. Historically, the subgroups of TOS have consisted of Neurogenic (NTOS), Venous (VTOS
or Paget Schroetter Syndrome, PSS), and Arterial (ATOS) (85). Neurogenic TOS accounts for over 95% of the cases, followed by venous (3–5%) and arterial (1–2%). (10) Neurogenic TOS (NTOS) has been further divided into True (TNTOS) and Disputed NTOS (DNTOS), with disputed reportedly representing 95–99% of all neurogenic cases [11]. The symptoms of TTOS and DNTOS are largely the same, although objective findings from nerve conduction studies and needle electromyography are notably absent in the DNTOS [12]. TNTOS most commonly affects a younger woman in their teenage years, is associated with cervical ribs or cervical bands, and is usually unilateral. Disputed NTOS is most commonly seen in women ranging from their 20s to 60s and is often bilateral [13]. One possible mechanism for the pathogenesis of a subgroup of patients with DNTOS who present with neurologic symptoms of the upper extremity who have negative nerve conduction studies and a normal neurologic exam is the subject of the present paper.
Recently, examination of the medial aspect of the resected first ribs in patients with Paget–Schroetter syndrome has demonstrated the presence of a congenitally malformed bony tubercle that forms a tighter and wider joint at the junction of the first rib and the sternum [4-6]. (Figure. 2)

Figure 2: Preoperative MRA with maneuvers in a patient with Paget Schroetter Syndrome. The Arrows point to the extrinsic compression of the subclavian vein at its junction with the innominate vein by a bony protuberance on the underside of the vein.
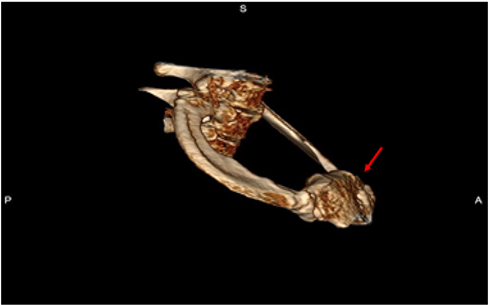
It has been observed that the wider and less mobile cost-sternal joint “locks” the medial aspect of the first rib into place and results in extrinsic compression of the boney tubercle onto the subclavian vein at its junction with the innominate vein. It can be surmised that without the benefit of the sophisticated modern imaging, and relying only on intraoperative observations, it is likely that historically surgeons have erroneously referred to this tubercle as the hypertrophied costoclavicular ligament and the hypertrophied scaleneus anticus tubercle. This abnormal tubercle on the medial aspect of the first rib can be seen on 3-D reconstruction of computerized axial tomograms in patients with PSS. (Figure. 3) In addition, the extrinsic compression of the subclavian vein by the tubercle at the medial aspect of the first rib can be demonstrated on dynamic magnetic resonance angiography (MRA) with maneuvers and dynamic venography. (Figures. 4a, 4b)
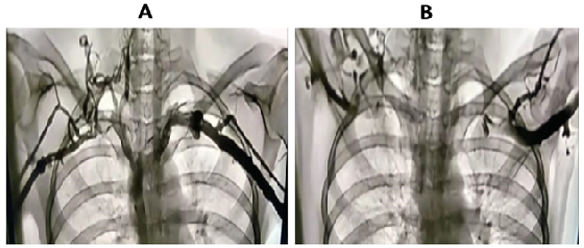
Furthermore, these studies clearly demonstrate that the subclavian vein compression increases with elevation of the arm above the shoulder. Prolonged compression stemming from activities that elevate the arm above the shoulder, result in thrombosis of the vein (PSS). As a definitive proof of the proposed pathogenesis of Paget Schroetter Syndrome, Gharagozloo et al. have demonstrated that disarticulation of the costo-sternal joint and resection of the medial aspect of the first rib results in decompression of the subclavian vein and complete resolution of symptoms [6].
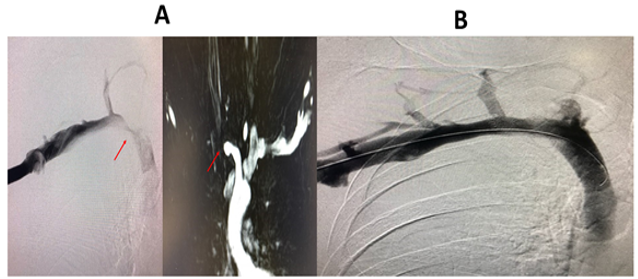
Observations in patients with a previous diagnosis of Neurogenic TOS who had persistent upper extremity neurologic symptoms following first rib resection by the transaxillary and supraclavicular approaches, revealed persistent extrinsic compression of the subclavian innominate junction on dynamic MRA. Disarticulation of the cost-sternal joint and removal of the remaining portion of the first rib, which bore a tubercle similar to that which was seen in patients with Paget Schroetter syndrome, resulted in relief of neurologic symptoms in all patients. In turn, Postoperative MRA and Venogram showed relief of extrinsic compression and decompression of the subclavian innominate junction. (Figures. 5a, 5b) This observation, in addition to the observation that patients with PSS have diffuse neurologic symptoms of the upper extremity prior to clotting of SV, led to the hypothesis that in a subgroup of patients with DNTOS, upper extremity neurologic symptoms may be due to venous compression and the resultant venous ischemia of the nerves in the upper extremity. This hypothesis is supported by the fact that the upper extremity is fed by a single artery and a single vein as an “end organ.” In such a setting, studies have demonstrated that the blood-nerve barrier in the nerve root was more easily broken by venous congestion than by arterial ischemia. Venous congestion may be an essential factor precipitating circulatory disturbance in nerve roots and inducing neurogenic intermittent claudication. This phenomenon is illustrated by the feeling of a leg “falling asleep” or pain and paresthesia which is experienced in the lower extremity after crossing the leg for a prolonged period of time. Of interest, patients with DNTOS liken their symptoms to their arms “falling asleep”.
In a proof-of-concept study, surgical outcomes in patients diagnosed with DNTOS who underwent robotic first rib resection were reviewed. Diagnosis was made by history, physical exam, MRI of C-spine, orthopedic and neurologic examination, nerve conduction studies, and MRA of the thoracic outlet with maneuvers. Patients with specific nerve compression, cervical ribs or cervical bands we excluded. Patients with compression of the subclavian vein by the medial aspect of the first rib underwent robotic resection of the first rib. Subjective symptoms were assessed by Disabilities of the Arm, Shoulder and Hand Questionnaire Score (Quick DASH), at 1 week, 1 month, and 6 months. With relief of extrinsic compression on the subclavian vein, 97% of patients with Disputed Neurogenic TOS experienced complete relief of symptoms [14, 15]. Significant relief of symptoms was reported in the remaining 3% of patients.
In this study we compared the resected ribs from patients with DNTOS who experienced complete postoperative relief of symptoms to normal ribs. In patients with Disputed Neurogenic TOS, the first rib exhibits an abnormal bony tubercle immediately lateral to the costo-sternal joint. The tubercle is found in the same location as the subclavian groove which is seen in normal first ribs. The tubercle results in a wider and tighter costo-sternal joint and traps the subclavian vein at its junction with the innominate vein. In this study, in normal individuals, the rib thickness at the subclavian groove was 0.2cm which represented an indentation of 0.8cm from the rib surface. It can be surmised that at the time of extension of the upper extremity above the shoulder and elevation of the first rib, the presence of this groove prevents compression of the subclavian vein by the rib. On the other hand, in patients with DNTOS the thickness of the first rib at the abnormal tubercle was 1.4 cm, which represents a differential elevation of 1.2 cm above the subclavian groove. Given the fact that the subclavian vein has an average diameter of approximately 1cm [16] in its position over the first rib, it can be concluded that the tubercle compresses the subclavian vein at rest, and significantly occludes the vein with extension of the arm above the shoulder.
These observations support the “ischemic” versus the “compressive” pathogenesis of a subgroup of patients with DNTOS. In these patients DNTOS appears to be the manifestation of a congenital malformation of the first rib. The congenital malformation is in the form of a pronounced tubercle, which results in an abnormal costo-sternal joint and the compression of the subclavian vein at its junction with the innominate vein. (Figure. 6) The compression of the subclavian vein in the thoracic outlet results in a spectrum of neurologic symptoms which are the result of venous ischemia of the upper extremity nerves. The ischemic pathogenesis of DNTOS is consistent with the normal neurologic exam and lack of objective evidence for nerve compression in these patients.

Figure 6: Resected specimen of the medial aspect of the first rib at the costo-sternal junction showing the abnormal bony tubercle which results in compression of the subclavian vein (SV) at its junction with the innominate vein (IV).
Magnetic Resonance Angiography clearly demonstrates the extrinsic compression at the subclavian innominate junction and can guide the decision for surgery. The most compelling evidence for ischemic pathogenesis of DNTOS is the relief of symptoms following disarticulation of the costo-sternal joint and removal of the medial aspect of the first rib.
A bony tubercle at the site of the subclavian vein groove in patients with DNTOS may be the pathologic entity which causes extrinsic compression of the subclavian vein at rest. The neurologic symptoms resolve following disarticulation and resection of the medial aspect of the first rib. In a subgroup of patients, NTOS may be the manifestation of venous ischemia of the nerves of the upper extremity as opposed to nerve compression.
None.
The author(s) declare that they have no competing interests
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
