
Research Article | DOI: https://doi.org/10.31579/2641-0419/147Copyright
*Corresponding Author: Ezra A Amsterdam, 4860 Y Street, Ellison Building, Suite 2820, Sacramento, CA 95817
Citation: Rakhee Makhija., Sandhya Venugopal., Nene Takahashi., Mrudula Guthikonda., Lavanya Manda., et al., (2021) Progression of Aortic Stenosis and Long-term Follow-Up in Women. J. Clinical Cardiology and Cardiovascular Interventions, 4(8); Doi:10.31579/2641-0419/147
Copyright: © 2021 Ezra A Amsterdam, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 February 2021 | Accepted: 19 April 2021 | Published: 26 April 2021
Keywords: aortic stenosis in women; aortic stenosis progression; valvular heart disease; aortic stenosis prognosis
Data on the rate of progression of aortic stenosis (AS) in women are limited. We retrospectively studied 95 female patients (age 75 ± 13 yrs) with aortic valve area (AVA) <2.0 cm2 (mild AS 1.5-1.9 cm2, moderate AS 1.0-1.4 cm2, severe AS <1.0 cm2). All patients underwent serial transthoracic echocardiography. We determined annual AVA decrease (rate of AS progression) by 3 approaches, each of which was applied to the entire cohort: 1) as a single group; 2) in the 3 subgroups of mild, moderate and severe AS; and 3) in the rapid and slower progressors. Study endpoints were aortic valve replacement (AVR) and all-cause mortality. The mean duration of follow-up was 4.5 ± 2.9 years. Mean rate of reduction in AVA for the total study group was 0.14 ± 0.16 cm2/yr and was directly related to presence of hypertension and baseline AVA, and inversely related to follow-up duration (all p<0.05). The annualized decrease in AVA for each of the subgroups of mild, moderate and severe AS at baseline was 0.21±0.31 cm2, 0.13±0.11 cm2, 0.11±0.09 cm2, respectively (p<0.0001). Rapid progression of AS (decrease in AVA ≥0.20 cm2/yr) occurred in 21% of patients (n=20) and was associated with baseline hypertension (p=0.03) and inversely related to follow-up duration (p=0.0007). Rapid progressors had shorter follow-up than slower progressors (20 vs. 42 mos, p=0.002). Event-free survival with end-points of death (n=65) or surgical/transcatheter AVR (n=24) at 1, 3, and 5 years, respectively, was 93%, 66% and 40% for mild AS; 96%, 72% and 48% for moderate AS; and 93%, 38% and 24% for severe AS. Thus, event-free survival at 5 years in patients with baseline severe AS was approximately half that of patients with AS of mild or moderate severity. In addition, event-free survival at 1 year in slower progressors was 92% and in rapid progressors was 70%.
Running head: Aortic stenosis in women
Aortic stenosis (AS) is the most common valvular heart disease in developed countries, affecting 2-7% of persons >65 years old [1]. Many of the factors associated with development of AS parallel those for atherosclerotic vascular disease [2]. However, there is a paucity of data on the relation of these and other factors to progression of AS specifically in women because, with few exceptions, women have been studied in mixed gender populations [3-14]. Rate of progression of AS is an essential aspect of patient management, especially in terms of valve replacement [2-8]. Our study aimed to determine: rate of progression of AS in women; its relation to mild, moderate and severe baseline AS: and the prevalence of those with rapid AS progression. Study endpoints were mortality and aortic valve replacement (AVR).
We queried the echocardiographic database of the University of California, Davis, Medical Center, to identify consecutive female patients with at least 2 transthoracic echocardiograms (TTE) at ≥3-month intervals and aortic valve area (AVA) <0.20 cm2 at study entry. Patients were followed during the interval from 2002 to 2017. Clinical data were obtained from patients’ electronic medical records including age, coronary artery disease (history of myocardial infarction, coronary revascularization), diabetes, hypertension (blood pressure ≥140/90 mmHg [15]), dyslipidemia, chronic kidney disease and smoking. Laboratory data included basic serum chemistries, hemoglobin A1c and lipid panel.
Transthoracic echocardiograms were performed with standard techniques according to the American Society of Echocardiography guidelines [16-18]. Left ventricular outflow tract diameter and gradient were measured in the parasternal long axis view with pulsed Doppler flow. The peak systolic transaortic valve jet velocity was determined from the continuous Doppler flow velocity signal across the aortic valve in apical views and the peak and mean aortic valve systolic gradients were calculated from the modified Bernoulli equation. AVA was determined from the continuity equation [19]. The degree of aortic valve calcification was estimated semi-quantitively from parasternal short axis views and recorded as mild (isolated, small spots), moderate (multiple larger spots), and severe (extensive thickening and calcification of all 3 aortic valve leaflets) [6]. Left ventricular ejection fraction was calculated by the apical biplane method of disks. The degree of AS was classified according to current American College of Cardiology/American Heart Association guidelines into mild (AVA 1.5-1.9 cm2), moderate (AVA 1.0–1.5 cm2) and severe AS (AVA <1.0 cm2) [20]. AS progression in each patient was measured as annual change in AVA (cm2/yr) during the interval from the TTE at study entry to the most recent follow-up TTE (total change in AVA divided by follow-up interval [years]). For additional analyses, patients were divided into rapid progressors (annual AVA decrease of ≥0.20 cm2/yr) and slower progressors (annual AVA decrease of <0.20 cm2/yr) [21]. Data on AVR and all-cause mortality were obtained from patients’ electronic medical records.
Statistical tests were performed with Stata 13.0 MP (StataCorp LP, College Station, TX, USA). Continuous data are presented as mean ± SD and range or percent and their differences were tested by unpaired t-test. Categorical data were compared with X2 test. Reverse step-wise multiple regression analysis was used to determine independent predictors of AVA reduction. Logistic regression analysis was performed to assess predictors of rapid AS progressors. A difference of p<0.05 was considered significant. Event-free survival was depicted by Kaplan-Meier curves according to AS severity and rapidity of progression with log-rank test to compare differences between groups.
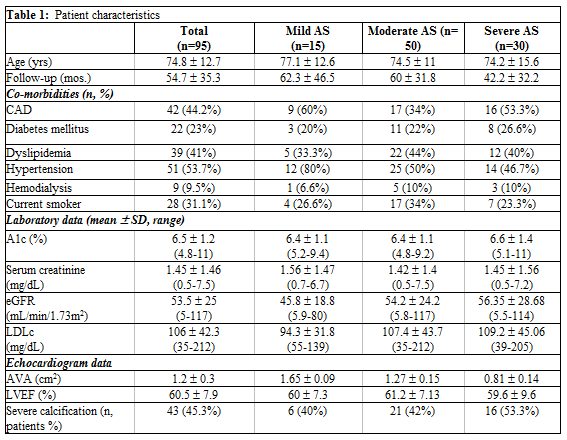
The clinical characteristics of the study group are shown in Table 1. Average age of the patients was 75 years and included a wide range. Follow-up interval was more than 4.5 years. A majority of the women fulfilled criteria for moderate baseline AS and almost one-third had severe AS. More than half of thepatients had ≥2 cardiac risk factors, the most common of which was hypertension; almost half of the patients had coronary artery disease and one-third were current smokers (Table 1).
Number of TTEs per patient was approximately 3 and the average interval between any 2 TTEs was 10 months. The baseline AVA for the entire cohort was 1.2 cm2 and average left ventricular ejection fraction was normal (Table 1). Average rate of decrease in AVA for the total cohort was approximately 0.14 cm2/yr. Annualized decrease in AVA for each of the 3 AS subgroups was greatest in patients with mild baseline AS (0.21 cm2/yr and less in patients with moderate (0.13 cm2/yr) and severe AS (0.11/cm2/yr) (p<0.001). About half of our patients had severe calcification and thickening of all 3 aortic valve leaflets (Table 1).
Progression to severe AS occurred in 26% of patients with initially mild baseline AS and in 66% with initially moderate AS. Factors that univariately correlated to annualized decrease in AVA were hypertension and follow-up duration (both p<0.05) (Table 2).
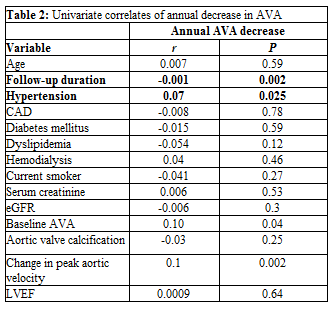
The latter factors were independently associated with AS progression. There was no correlation of age, coronary artery disease, diabetes, dyslipidemia, current smoking, chronic kidney disease or aortic valve calcification with AS progression.
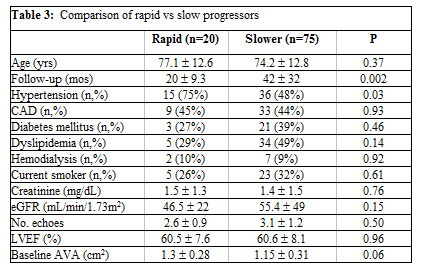
Patients with rapid AS progression (decrease in AVA≥0.20 cm2/yr) comprised approximately one-fifth of our cohort of 95 patients. Average decrease in AVA was >0.30 cm2/yr for rapid progressors and approximately one-fourth this rate (0.08 cm2/yr) in the slower progressors. Compared to slower progressors, the rapid progressors had more frequent hypertension, larger baseline AVA and shorter follow-up (all p<0.05) (Table 3).
Results of logistic regression analysis depicting factors affecting rapid progression is shown in (Table 4).

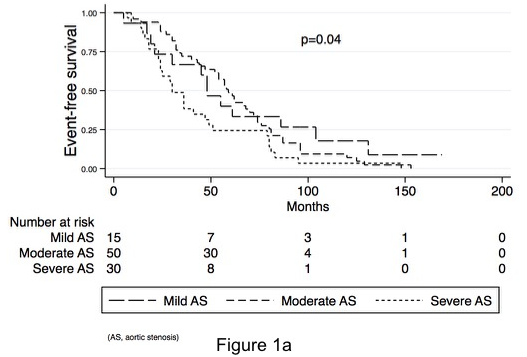
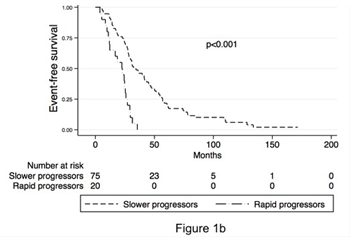
Follow-up interval exceeded 4 years and included >90% of patients (n=89). In the total group of 95 patients, mortality was 68% (n = 65), 25% (n=24) received AVR and 6% (n = 6) were lost to follow-up. The annual average rate of AVR was 5%. Event-free survival with end-points of death (n=65) or surgical/transcatheter AVR (n=24) at 1, 3, and 5 years, respectively, was 93%, 66% and 40% for mild AS; 96%, 72% and 48% for moderate AS; and 93%, 38% and 24% for severe AS. Follow-up duration differed significantly between those with mild and severe AS (p=0.04) (Figure 1a). Among rapid progressors, mortality was 75%, and 25% of patients underwent AVR. In the slower progressors, 68% died and 25% received AVR. Event-free survival at 1 year in slower progressors was 92% and in rapid progressors was 70%. (Figure 1b).
This study extends our understanding of AS progression and clinical outcomes in women. First, it enhances prior limited data on this disease and its related factors in females [22]; second, it includes one of the largest of the few AS cohorts limited to women; and third, the follow-up interval is among the longest in women with AS. Importantly, we found no prior studies that reported incidence of AVR specifically in women.
Our results show that the rate of AS progression in women was similar to previously reported findings in major studies of mixed sex cohorts [2,3,5,6]. However, most of the latter investigations included a majority of men with no delineation of the sexes, precluding assessment of AS progression specifically in women. Additionally, many of these studies involved smaller follow-up intervals for assessment of progression than our study [2-7, 10,12,13,23]. Further, our findings indicate that rapid AS progression was directly associated with hypertension and baseline AVA and inversely related to follow-up duration. Our results reveal that event-free survival at 5 years, including AVR and mortality, were significantly more favorable in women with mild and moderate baseline AS than in those with severe AS.
Our data revealed an average annual decrease in AVA of 0.14 cm2 (0.09 to 0.21) during a follow-up of 4.5 years in 95 females. The annualized decrease in AVA for each of the 3 AS subgroups was greatest in patients with mild AS. Although prior studies reveal a wide range of AS progression in mixed sex cohorts, our findings in women are consistent with the predominant results of studies with rates of 0.11 to 0.14 cm2/yr [2,3,5,6]. However, some reports of AS progression in women noted rates as low as 0.044 and 0.08 cm2/yr [22]. Rapid AS progression, defined as ≥0.20 cm2/yr [21], occurred in 20 (21%) of our patients and was associated with a higher prevalence of hypertension and larger baseline AVA compared to their frequencies in the slower progressors.
In our patients, AS progression independently correlated with hypertension. Prior studies of mixed sex cohorts have been inconsistent regarding this relationship. Aronow and co-workers [32] found that hypertension (systolic ³140 mm Hg) was positively associated with AS progression in all patients with mild baseline AS in a 2-year follow-up. By contrast in our cohort of mild, moderate and severe AS, follow-up was more than twice as long as that of Aronow et al. Other studies reported no correlation between hypertension and AS progression [11,33] but one did note that hypertension was associated with increased mortality in patients with AS, especially in women [11].
As anticipated, the follow-up interval to AVR or mortality was considerably shorter in our patients with rapid progression than in the slower progressors (20 vs 42 mos, p<0.002). Unlike several previous observational studies of mixed gender, we did not find an association between AS progression and age [34,35], smoking [24,32], chronic kidney disease [13,14,24], diabetes mellitus [32] or dyslipidemia [36,37] (Table 3), which may be related to the size of our cohort. We found that AS progressed more rapidly in patients with mild than severe baseline AVA: 0.21 vs. 0.11 cm2/yr. Bahler et al [13] also identified baseline AVA as an independent predictor of rapid AS progression, which they defined as ≥0.10 cm2/yr. However, their study was shorter (1.8 yrs) and smaller (61 women) than ours.
Studies of long-term mortality and AVR specifically in women are few. In gender-mixed populations the annual rate of surgical AVR has varied widely [3,7,11,34,38] from 4% to 25% in follow-up studies of <1 year [11] to >5.0 years [38]of follow-up. In our patients with AS varying from mild to severe, the annual rate of AVR was 5%. In one investigation, a relatively high rate of AVR at 1 year (~25%) is likely accounted for by variables such as baseline severity of AS, rapidity of progression and symptoms [11]. The annual AVR of 10% reported by Pellikka et al [38]in 622 male and female patients was closer to ours (5%) as was that of Rosenhek et al. in 176 mixed sex patients (4%) [7].
Reports of mortality related specifically to AS in women are discordant. Of the 2 extended follow-up studies in women with AS, one for 5.4 yrs, reported that all-cause mortality was 31% lower in women than men [38] while the other, in which patients were observed for 3.2 yrs, detected no mortality, but the rate of AS-related events was almost twice as high in women than men[22]. Annual all-cause mortality in our total cohort was 15% and was highest in those with baseline severe AS (Figure 1a). To our knowledge, mortality in women with AS has not been previously addressed in terms of graded severity of baseline disease. By contrast, in mixed gender studies of AS, annual all-cause mortality has varied widely [3,7,11,34,38] although rates in the most commonly cited studies are 2-4% [3,7]. The differences between mortality in the latter studies are again likely related to multiple factors contributing to this endpoint. In this regard, Rosenhek et al [7] studied patients with mild and moderate AS, while our cohort included those with severe reduction in AVA. Additionally, the cohort of Otto et al. was approximately a decade younger than our patients [3].
Our study has several limitations. It is a single center retrospective investigation with the inherent limitations of this method. However, it adds information on an important subject with previously limited evidence. The study cohort is not large enough to exclude all factors that may influence AS progression, but we have assessed multiple potential variables. Our study did not include a control group of males but prior investigations are predominantly of males. Our results are based on changes in aortic valve area rather than gradients, although multiple measures of AS based on gradients and velocity have been published. The clinical outcomes and frequency of AVR reflect results from the pre-TAVR era but our data on rates of AS progression and rapid progression are relevant to contemporary management. Our cohort is limited in size number but it compares favorably in this regard with prior investigations of AS in women, and our follow-duration is longer than most studies in women. We did not find a relationship between diabetes and renal failure with AS progression, unlike other larger mixed sex studies, as ours is a smaller investigation and underpowered to determine predictors.
This study extends limited data on aortic stenosis in women by reporting average rate of progression of this lesion and associated factors, relation of aortic stenosis to severity of this disease, and identification of rapid and slower aortic stenosis progressors.
Acknowledgement: The project described was supported by the National Center for Advancing Translational Sciences, National Institutes of Health, through grant number UL1 TR001860. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Funding source(s): none
All authors contributed to the production and analysis of the data, had acquisition to the data and contributed to production of the manuscript
Declarations of interest: none
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
