
Research article | DOI: https://doi.org/10.31579/2642-973X/057
1 Neurosurgery Service, Maciel Hospital, ASSE, Uruguay.
2 Department of Quantitative Methods, Faculty of Medicine, Montevideo. University of the Republic. Uruguay.
3 Chair of Imaging Hospital de Clínicas, Montevideo. University of the Republic. Uruguay.
4 Chair of Neurosurgery, Hospital de Clínicas de Montevideo, University of the Republic. Uruguay.
*Corresponding Author: Alejandra Jaume, Neurosurgery Service, Maciel Hospital, ASSE, Uruguay
Citation: Fernando Martínez, Alejandra Jaume, Pedro Macadam, Verónica De los Santos, Lucia Pereira, et al (2023), Prognostic Factors in Patients with Aneurysmal Subaraconid Hemorrhage in Uruguay: Presentation of a Multi-Center Prospective Study, J. Brain and Neurological Disorders, 6(3): DOI:10.31579/2642-973X/057
Copyright: © 2023, Alejandra Jaume. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 May 2023 | Accepted: 10 May 2023 | Published: 17 May 2023
Keywords: subarachnoid hemorrhage; aneurysm; treatment; prognosis
Subarachnoid hemorrhage (SAH) usually attacks sectors of the population in productive ages (mostly between 30 and 60 years old), which represents a very high social burden for the system and destroys family nuclei. According to a study by the ACROSS Group, overall mortality one month after diagnosis of SAH was 39%. The objective of this work is to identify the factors of poor prognosis for mortality or poor evolution of our population.
All patients older than 18 years with a diagnosis of HSAea, who consulted in a healthcare center in the country between 11/01/2019 and 10/31/2020, were included in the study. The clinical-epidemiological characteristics and comorbidities at the time of diagnosis, the type of treatment received and variables of clinical evolution during the following 6 months were surveyed. The statistical analysis of the data was based on the period evaluated, description of the variables studied and the identification of predictors of poor clinical evolution. Due to the multicenter and national nature of the study, it had to be submitted for evaluation by all the Ethics Committees of the participating health institutions, and by the National Research Ethics Commission (CNEI).
This is a prospective and multicenter study, including all patients over 18 years of age who presented aneurysmal spontaneous SAH in Uruguay between November 1, 2019 and July 31, 2020.
Variables relevant to the pathology under study such as age, sex, arterial hypertension, smoking, diabetes, alcoholism, and personal or family history of aneurysm were analyzed. Regarding the clinical grading ofdiagnostic classification, they were classified as mild SAH at Hunt and Hes-World Federation Neurosurgical Score (HyH-WFNS) 1 and 2, moderate SAH at HyH-WFNS 3, and severe SAH at HyH-WFNS 4 and 5. In addition was analyzed: Vascular study(s) performed, topography of the aneurysm that bled, indicated traten, care center where the treatment was performed, complication related to the indicated treatment, complication related to SAH, modified ranking score (mRS) at 6 months, post-treatment control vascular study, cause of death, date of death, discharge date, and end of follow-up date. Good evolution was defined as patients with mRS equal to or less than 2, and poor evolution was considered to be patients with mRS equal to or greater than 3.
Regarding the statistical analysis of the data pTo estimate the survival of the patients in the analyzed cohort, the Kaplan-Meier method was used and for the statistical comparison between survival functions by strata of another variable, the Log-Rank test was used. To identify possible prognostic factors for mortality and poor clinical evolution at 6 months of follow-up after SAH diagnosis and treatment, a Cox proportional hazards regression model was used. In view of the multivariate analysis, a preliminary selection of the candidate variables was first performed (p-value < 0>
All the information collected in this study is confidential and was handled according to the ethical standards for epidemiological research studies. The research was previously approved byall institutional Ethics Committees, as well as analyzed by the National Research Ethics Commission (CNEI), as it is a multicenter study. It also had the support and endorsement of the Uruguayan Society of Neurosurgery (SUNC).
Result:
A total of 211 cases were observed in the evaluated period. The average age was 57 years with a predominance of the female sex (75%). Mortality 6 months after diagnosis was 54.5%, and 64.5% of the cases presented a "poor clinical evolution. "Median estimated survival time was 70 days.
Conclusions: The independent predictors of higher mortality were: presence of "severe" SAH from the onset of the symptoms, presence of a dissecting or spindle-shaped aneurysm, presence of a wide neck or absence of a neck in the neck-bottom relationship of the aneurysm, and presenting a Age greater than 60 years at the time of diagnosis. The facts The independent predictors of poor clinical evolution demonstrated were: presence of "severe" SAH from the onset of symptoms, presence of a dissecting or fusiform aneurysm, presence of large ischemia as a complication of the treatment performed, and be older than 60 years at the time of diagnosis
A total of 213 patients were included in the study period. Two patients were excluded because they had a negative vascular study for aneurysm. Thus, the total number of patients analyzed was 211.
The mean age of the patients was 57 years, the female sex predominated in 75% of the cases, and 66% of the patients were hypertensive; and 40% of patients smokers.
Regarding the diagnostic classification or initial diagnosis, 35% of the patients were classified as mild SAH by HyH and 45% by WFNS; 15% and 3% of moderate SAH by HyH and WFNS respectively, and 50% and 52% of severe SAH.
The average hospital stay of the patients analyzed was 26 days, with a minimum of 0 and a maximum of 6 months.
Se The clinical evolution of the patients was assessed using the mRS scale at 6 months, defining "poor clinical evolution" as mRS values greater than or equal to 3, and "good clinical evolution" as mRS values less than or equal to to 2.
The mortality observed in the cohort at 6 months of follow-up was 54.5% (115 patients), and according to the previously defined criteria, 64.5% of the cases presented a "poor clinical evolution".
Median estimated survival time was 70 days. The cumulative survival function curve, estimated using the Kaplan-Meier method, is shown in Figure 1.
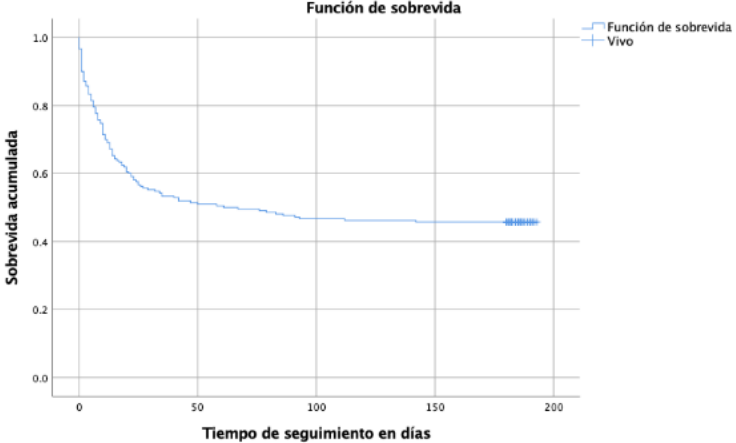
Figure 1: Survival function (Kaplan-Meier) of the 211 included patients.
Within the "declared" causes of death, 42% were due to the disease itself, 10% were linked to a complication due to the chosen treatment, and 2% were due to extra-neurological causes.
All the variables that could favor a fatal outcome of the patients were evaluated, both during their hospital stay and during their evolutionary control at 6 months. The results of the univariate analysis for qualitative and quantitative variables are detailed in tables 1 and 2 respectively.
It is necessary to clarify at this point that the significant effect shown by the variable "treatment performed" reflects the fact that the treatment that would have been indicated could not be given to seriously ill patients. When a sub-analysis was carried out comparing only the patients who were treated, it was possible to verify that said difference became statistically insignificant between surgery and embolization.
In turn, when we analyzed the complications related to the treatment, we observed that it was not significant overall, but when we analyzed each of them separately, the presence of major ischemia as a complication was the only one that showed a statistically significant effect (p= 0.002). Similarly, it was observed with SAH-related complications; When performing a sub-analysis of each of them, vasospasm was the only one that showed a predictive effect on mortality (p= 0.005).
| Variable | Deceased n: 115 (%) | Alive n: 96 (%) | p-value* |
| female gender | 86 (75) | 72 (75) | 0.550 |
| Coming from the interior | 49 (42) | 45 (46) | 0.315 |
| strict pandemic | 28 (24) | 23 (23) | 0.554 |
| Afro-descendant race | 3 (2) | eleven) | 0.381 |
| Arterial hypertension | 82 (71) | 58 (60) | 0.064 |
| smoking | 42 (36) | 46 (46) | 0.063 |
| Drug Addiction | 5 (4) | 3 (3) | 0.464 |
| Personal and Family History of Aneurysm | twenty-one) | 6 (6) | 0.089 |
| Obesity (BMI greater than 30kg/m2) | 13 (11) | 11 (12) | 0.570 |
| Alcoholism | 4 (3) | eleven) | 0.246 |
| Diabetes | 13 (11) | 3 (3) | 0.021 |
| Headaches and vomiting as the main symptom | 48 (42) | 48 (50) | 0.244 |
| Coma from baseline (GSC equal to or less than 8) | 24 (20) | 4 (4) | <0> |
| Severe SAH from onset (WFNS andHH greater than3) | 83 (72) | 27 (28) | <0> |
| diagnostic error | 18 (15) | 33 (34) | <0> |
Aneurysm Type: Saccular Aneurysm Dissecting Aneurysm Fusiform Aneurysm |
105 (91) 5 (4) 5 (4) |
95 (98) 0 (4) eleven) |
0.039
|
Neck-bottom relationship of the aneurysm: boy neck big neck Neckless |
71 (62) 40 (35) 4 (3) |
74 (77) 22 (23) 0 (0) |
0.022
|
treatment performed Surgery embolization nothing by gravity |
35 (30) 25 (22) 55 (48) |
56 (58) 40 (42) 0 (0) |
<0> |
| Treatment-related complication | 24 (21) | 28 (29) | 0.109 |
| HSA-related complication | 86 (75) | 72 (75) | 0.550 |
*Chi-square test.
Table 1: Factors associated with higher mortality in the 211 patients included: Univariate analysis (qualitative variables).
| Variable | Deceased md (RIQ) | Alive md (RIQ) | p-value* |
| Age (years) | 61 (20) | 53 (15) | <0> |
| Diagnostic Interval (days) | 1 (2) | 1 (3) | 0.004 |
| Indicated Treatment Interval (days) | 0 (1) | 0 (1) | 0.009 |
| Interval Treatment Performed (days) | eleven) | eleven) | 0.141 |
| Delayed start of treatment (days) | 0 (1) | 0 (1) | 0.664 |
| Hospitalization time (days) | 13 (22) | 28.5 (27) | <0> |
Table 2: Factors associated with higher mortality in the 211 patients included: Univariate analysis (quantitative variables).
Md: Medium. IQR: interquartile range; Diagnostic Interval: time between the onset of symptoms and the diagnosis of SAH. Indicated Treatment Interval: time between the diagnosis of SAH and the indicated treatment. Interval Treatment Performed: time between the diagnosis of SAH and the treatment performed. Treatment start delay: time between the indicated treatment and the treatment performed.
*Mann Whitney test P value
As a result of the multivariate analysis (identification of the independent predictors of mortality), the detail of the final model obtained with the 4 identified variables and their respective Hazard Ratio (HR) and 95% confidence intervals (95%CI), is shown in table 3.
| Variable | p-value* | HR (95%CI) |
Severe SAH from onset (WFNS and HH greater than 3) Aneurysm Type | <0> 0.023 | 3,488 (2,307-5,274) 2,198 (1,113-4,343) |
| Neck-bottom relationship of the aneurysm | 0.050 | 1,479 (0.997-2,196) |
| Age over 60 years. | <0> | 2,0665 (1,418-3,007) |
RR: relative risk; 95% CI: 95% confidence interval
Table 3: Independent predictors of mortality in the 211 patients studied: Multivariate analysis. Cox regression.
A total of 136 patients (64%) had a poor clinical evolution. In order to identify the characteristics of the patients that could predict or anticipate a "poor clinical evolution" in the short or medium term (follow-up period of this study, limited to 6 months from the diagnosis of SAH), all of them were analyzed. its characteristics at the time of diagnosis (demographics, comorbidities, habits and clinical presentation of SAH). The detail of the results of the univariate analysis is detailed in Tables 4 and 5. From the univariate analysis in this case, we must once again highlight that the type of treatment variable (surgery, embolization or none due to severity) should be interpreted with caution because This translates the difference between not performing any type of treatment and yes performing it, as we saw in the case of mortality analysis. Again here, after analyzing only the patients who were treated, no difference was observed between performing surgery versus embolization (p= 0.342).
Regarding the variable "complication linked to treatment", evaluated as the appearance of some type of complication attributable to treatment during follow-up, it was distributed in a similar way between patients with good and poor evolution (p=0.505). However, when each type of complication was analyzed separately, the presence of large ischemia did appear associated with a poor evolution of the patients, in the univariate analysis (p < 0>
| Variable | good evolution n: 75 (%) | bad evolution n: 136 (%) | p-value* |
| female gender | 55 (73) | 103 (75) | 0.410 |
| Coming from the interior | 38 (50) | 56 (41) | 0.118 |
| strict pandemic | 20 (26) | 31 (23) | 0.470 |
| Afro-descendant race | eleven) | 3 (2) | 0.553 |
| Arterial hypertension | 44 (58) | 96 (70) | 0.050 |
| smoking | 39 (52) | 49 (36) | 0.018 |
| Drug Addiction | 2 (2) | 6 (4) | 0.412 |
| Personal and Family History of Aneurysm | 5 (6) | 3 (2) | 0.108 |
| Obesity (BMI greater than 30kg/m2) | 8 (10) | 16 (11) | 0.501 |
| Alcoholism | 0 (0) | 5 (3) | 0.108 |
| Diabetes | 2 (2) | 14 (10) | 0.036 |
| Headaches and vomiting as the main symptom | 38 (50) | 58 (43) | 0.194 |
| Coma from baseline (GSC equal to or less than 8) | eleven) | 27 (20) | <0> |
| Severe SAH from onset (WFNS and HH greater than 3) | 13 (17) | 97 (71) | <0> |
| diagnostic error | 29 (38) | 22 (16) | <0> |
Aneurysm Type: Saccular Aneurysm Dissecting Aneurysm Fusiform Aneurysm | 74 (98) 0 (0) eleven) | 126 (92) 5 (4) 5 (4) |
0.050
|
Neck-bottom relationship of the aneurysm: boy neck big neck Neckless | 57 (76) 18 (24) 0 (0) | 88 (64) 44 (32) 4 (2) |
0.053
|
Type of treatment Surgery embolization nothing by gravity |
42 (56) 33 (44) 0 (0) |
49 (35) 32 (25) 55 (40) |
<0> |
| Treatment-related complication | 18 (24) | 34 (25) | 0.505 |
| HSA-related complication | 53 (70) | 105 (77) | 0.188 |
*Chi-square test P value.
Table 4: Factors associated with poor evolution in the 211 patients included: Univariate analysis of qualitative variables.
From the personal history of the patients, arterial hypertension, diabetes, and smoking habits were also found in the univariate analysis to be associated with a poor clinical evolution of the patients (Table 4).
| Variable | good evolution Median (IQ range) | bad evolution Median (IQ range) | p-value* |
| Age (years) | 52 (16) | 57 (20) | 0.005 |
| Diagnostic Interval (days) | 1 (4) | 0 (1) | <0> |
| Indicated Treatment Interval (days) | 0 (1) | 0 (0) | 0.057 |
| Interval Treatment Performed (days) | eleven) | eleven) | 0.322 |
| Delayed start of treatment (days) | 0 (1) | 0 (1) | 0.836 |
| Hospitalization time (days) | 25 (15) | 23 (47) | <0> |
Md: Medium. Diagnostic Interval: time between the onset of symptoms and the diagnosis of SAH. Indicated Treatment Interval: time between the diagnosis of SAH and the indicated treatment. Interval Treatment Performed: time between the diagnosis of SAH and the treatment performed. Treatment start delay: time between the indicated treatment and the treatment performed.
*Mann-Whitney test.
Table 5: Factors associated with poor clinical evolution in the 211 patients included: Univariate analysis of quantitative variables.
For the multivariate analysis, all the variables that in the univariate analysis presented statistical significance at a significance level less than or equal to 0.25 were then retained. The variables identified as independent predictors of poor clinical evolution of the patients are shown in Table 6, with their respective Hazard Ratio (HR) estimates and 95% confidence intervals (95%CI).
| Variable | p-value* | HR (95% CI) |
Severe SAH from onset (WFNS and HH >3) Type of Aneurysm (dis or fus vs. saccular) | <0> 0.002 | 3,844 (2,631-5,617) 2,767 (1,436-5,333) |
| Major ischemia as a complication of treatment | 0.026 | 1,854 (1,077-3,193) |
| Age over 60 years. | <0> | 1,861 (1,316-2,632) |
*Wald's test
Table 6: Predictors of poor clinical evolution in the 211 patients included: Multivariate analysis. Cox regression.
Age, as in most neurological diseases, has a predictive role in clinical evolution, as evidenced in this study, with the breaking point being 60 years, which is much lower than for other diseases.
The symptoms at the onset of the symptoms, as well as the type of aneurysm, were confirmed in this work as expected from international reports, as independent predictors of poor clinical evolution.
It is interesting to evaluate, among the complications due to the treatment carried out, that large ischemia at the treatment site was significant as a predictor of poor clinical evolution, which provides information little published in the literature.
Regarding the clinical state at the onset of the symptoms, in the present work a high percentage of severe SAH was evidenced both by the H&H classification (65%) and the WFNS (55%). These percentages are higher than those reported in the international literature, where 20-30% of SAHs are classified as severe from the onset of the symptoms6,7. This is extremely important in order to study in the future whether our country has a predisposing factor for more serious SAH, since the initial clinical state is one of the main prognostic factors, evidencing an unfavorable prognosis in published works.the rest40% in severe SAH, falling to less than 20% with mild SAH (grades I-II)8.
In our work, a 6-month cumulative mortality of 54% was observed, which, according to the causes of death, was distributed as follows: 42% due to the disease itself, 10% linked to a complication of the chosen treatment, and 2% due to extra-neurological causes.By the way, we found that the mortality observed in our work is significantly higher than that reported in other works (30-40%)9,3. One possible explanation would be the fact that in our case material we have a high number of patients with severe SAH from the onset of the symptoms (50%) compared to other series in the literature where percentages of between 20 and 30% of severe SAH are reported10.
The independent predictors of mortality identified in our work were: presence of “severe” SAH from the onset of symptoms (HR= 3.4; 95%CI: 2.3-5.2), presence of dissecting or fusiform aneurysm (HR= 2.1; 95%CI: 1, 1-4.3), presence of a wide neck or absence of a neck in the neck-fundus relationship of the aneurysm (HR= 1.4; 95% CI: 0.9-2.1), and being older than 60 years at the time of diagnosis (HR= 2.0; 95% CI: 1.4-3.0).
Other authors also report the H&H, WFNS and GSC scales as good predictors of mortality11,12. Julien et al.10 also state, based on their prospective study of 1,532 patients, that the presence of vasospasm, HCF, and intracerebral hematoma also have a significant prognostic role. We must mention on this point that, during the analysis to identify potential factors associated with a higher risk of mortality in our work, there were a series of variables that, although they did not show a statistically significant effect (p<0>
SThe clinical evolution of the patients was evaluated according to the value of the mRS in the control 6 months after the diagnosis of SAH. “Poor clinical evolution” was defined as patients with mRS values greater than or equal to 3. Poor clinical evolution was evidenced in 64.5% of cases. Although this percentage is considered high compared to what has been reported in the international literature, analyzing mild and severe SAH separately at the beginning, we observed poor clinical evolution in 25% and 73%, respectively. These results are comparable to different publications, where it is reported that mild SAH have poor results and a worse prognosis in approximately 20, and SHTo serious in approximately 60%7.When the univariate analysis was performed, the following variables emerged as predictors of poor outcome: advanced age at diagnosis (>60 years), presence of diabetes as comorbidity, presence of hypertension, smoking habit, error at diagnosis, presence of coma from the onset of the symptoms, severe SAH from the onset, presence of a dissecting or fusiform aneurysm, no type of treatment, shorter diagnostic interval (time between onset of symptoms and diagnosis) and shorter hospital stay. These last two variables could be explained by the fact that the most severe patients are the ones that are diagnosed the fastest and die before.The presence of obesity, in turn, had a tendency to appear as a potential factor for poor clinical evolution, but its effect was not shown to be statistically significant.
Finally, when the multivariate analysis was performed, the independent predictors of poor outcome were:presence of “severe” SAH from the onset of symptoms (HR= 3.8; 95%CI: 2.6-5.6), presence of dissecting or fusiform aneurysm (HR= 2.7; 95%CI: 1, 4-5,3),presence of large ischemia as a complication of the treatment performed(HR= 1.8; 95%CI: 1.0-3.1), and being older than 60 years at diagnosis (HR= 1.8; 95%CI: 1.3-2.6). VanDonkelaar et al. in 201914 they published the SAFIRE scale, which is a modelAccurate, generalizable and easy to apply to predict the prognosis in patients with SAH such as: age, Fisher scale, WFNS scale, and aneurysm size. Almatter et al. in 201815 they reported as the main prognostic factors in SAH: age, initial clinical status, rebleeding, parenchymal hemorrhage, and middle cerebral artery aneurysm topography. For mild onset SAHs,Zijlmans et al. in 201813, they publishedas factors of poor prognosis and poor evolution at age: late cerebral ischemia, pneumonia, and meningitis. In severe SAHs,Mocco et al. in 20067 they reported as predictors of poor evolution and poor prognosis: age, severe HH scale in the preoperative period, aneurysm size, and hyperglycemia.
The follow-up of the patients in this study was 6 months, but we must clarify that, in the international literature, a follow-up during the first 10 years is recommended, with a vascular study every 5 years (CT angiography, MRI angiography or angiography), being stricter in patients with risk factors (female sex, smoker, AHT, and multiple aneurysms)16.
the HSAcontinues to be a disease with high associated morbidity and mortality and in the present work it was possible to identifyas independent predictors of higher mortality, the following factors: presence of “severe” SAH from the onset of the symptoms, presence of a dissecting or fusiform aneurysm, presence of a wide neck or absence of a neck in the neck-bottom relationship of the aneurysm, and be older than 60 years at the time of diagnosis.The factsThe independent predictors of poor clinical evolution demonstrated were: presence of "severe" SAH from the onset of symptoms, presence of a dissecting or fusiform aneurysm,presence of large ischemia as a complication of the treatment performed, and be older than 60 years at the time of diagnosis.
the independent predictive factors of higher mortality were: presence of “severe” SAH from the onset of the condition, presence of a dissecting or fusiform-type aneurysm, presence of a wide neck or absence of a neck in the neck-bottom relationship of the aneurysm, and be older than 60 years at the time of diagnosis. The independent predictors of poor clinical outcome demonstrated were: presence of “severe” SAH from the onset of the condition, presence of a dissecting or fusiform-type aneurysm, presence of large ischemia as a complication of the treatment performed, and being older than 60 years at diagnosis
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
