
Research Article | DOI: https://doi.org/10.31579/2690-4861/378
1 Clinic of Infectious Diseases, Multiprofile Hospital for Active Treatment, Stara Zagora, Bulgaria,
2 Dept. of Higiene, Epidemiology, Microbioogy, Parasitology and Infectious Diseases, Medical Faculty, Trakia University, Stara Zagora, Bulgaria,
3 Dept. of Social Medicine and Health Management, Medical Faculty Trakia University, Stara Zagora, Bulgaria
*Corresponding Author: Liliya Pekova, Section of Infectious Diseases, Department. of Higiene, Epidemiology, Microbioogy, Parasitology and Infectious Diseases, Medical Faculty, Trakia University, Stara Zagora, Bulgaria.
Citation: Pekova L, Angelova S, Yordanova A, Parusheva P, (2024), Prognostic factors for severe course and adverse outcome of Clostridium difficile infection after Covid 19, International Journal of Clinical Case Reports and Reviews. 16(3); DOI: 10.31579/2690-4861/378
Copyright: © 2024 Liliya Pekova, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 15 January 2024 | Accepted: 29 January 2024 | Published: 16 February 2024
Keywords: clostridium difficile infection; covid 19
Before the Covid 19 pandemic, the incidence of community-acquired Clostridium difficile infection (CDI) was 35-50%. SARS-CoV-2 created favorable conditions for its increase.
Aim: To identify the factors responsible for the severe course and adverse outcome in CDI post-Covid 19.
Materials and methods: 121 patients aged from 23 to 90 years-53 women and 68 men - with CDI and a recent Covid-19 were included in a prospective study. Clinical, epidemiological, laboratorial and molecular-genetic investigations were used.
Results: All patients were on long-term treatment with broad-spectrum antibiotics for SARS-CoV-2 infection. The most common symptoms of CDI were diarrhea, fever and loss of weight. The majority of patients were discharged in an improved condition. There were 12 lethal outcomes (9,91%).
Conclusion: Age over 65 years, presence of accompanying chronic diseases, as well
Clostridium difficile (CD) is a Gram positive (+) motile anaerobic bacterium that causes Clostridium difficille-associated diarrhea. Clostridium difficille infection (CDI) is a serious medical condition of a large intestine with a reccurence rate of 15-20% and a mortality rate of 5% [1]. CDI is a common hospital-acquired infection with increasing incidence, severity, recurrence and associated morbidity and mortality [2]. Potential risk factors include long-term antibiotic treatment, age over 65, immunocompromised patients, prolonged exposure to health-care facilities [3]. Clinical presentation can range from asymptomatic carriage to mild diarrhea, toxic megacolon and life-threatening fulminant colitis. Symptoms related to CDI are associated with the production and release of toxin A and toxin B [4]. The diagnosis of C difficile colitis should be suspected in any patient with diarrhea who has received antibiotics within the previous 3 months, has been recently hospitalized, and/or has an occurrence of diarrhea 48 hours or more after hospitalization [5] A significant increase in the incidence of CDI is noted during Covid-19 pandemic [6]. Most often, the manifestations of CDI are triggered by antibiotic therapy. Fluoroquinolones, clindamycin, cephalosporins are usually responsible for this, but basically any antibiotic can predispose to CDI. CDI occurs two weeks after the start of antibiotic therapy up to 10 weeks after its discontinuation. [7]. The leading symptom of CDI is watery diarrhea. Impurities of mucus and blood are possible, but melena is rare. In addition, there is spastic pain in the hypogastrium, low-grade fever, rarely exceeding 38.5 C with fever in 15% of cases, nausea and loss of appetite [8,9]. The rates of bacterial infection in Covid-19 pandemic are considerable and probably underestimated. A renewed attention of CDI is necessary. The large use of broad-spectrum antibiotics during Covid-19 pandemic raises serious concern about a consequent increase of CDI.
The aim of this study is to analyze clinical course, outcome and predisposing factors for high morbidity and mortality in patients with CDI and recent Covid-19. To underline the need of rational use of antimicrobial agents.
A total of 1284 Covid-19 patients were hospitalized at the Clinic of Infectious diseases, University hospital, Stara Zagora, Bulgaria. During April 2020 –August 2022 at the Clinic of Infectious diseases 121(9,42%) of them -53 female (43,8%) and 68 male (56,19%), aged 23-90 years, (69,64±12,12) were re-hospitalized with diagnose of CDI.
We conducted a prospective cohort study in order to assess clinical course, outcomes and risk factors for CDI in patients passed through Covid-19 infection. As inclusion criteria for patient participation in our study, we adopted the following: presence of diarrheal syndrome, evidence of Clostridium difficile toxins (A; B; A+B), evidence of recent Covid 19, use of antibiotics. Exclusion criteria were patients with a cause of the diarrheal syndrome other than Clostridium difficile, as well as the small number of those in whom CDI was nosocomially acquired without a previous SARS-CoV-19. Laboratory and microbiological analyses were made during hospital stay. Markers for disease severity and factors associated with increased risk of death such as degree of dehydration, occurrence of renal failure, edemas, presence of concomitant diseases and their severity, levels of laboratory parameters such as leukocyte count, CRP, fibrinogen, electrolytes, creatinine, total protein and albumin, were evaluated. All cases were followed up to 30 days from their hospital discharge to assess the recurrence rate and the mortality [10]. The diagnose was confirmed by combined GDH and toxin A/B immunoassay in stool samples – NADALR-CD toxin A/B +GDH. Being the test accepted as a specific-sensitive method for the detection of toxins A and B of Clostridium difficile, PCR was performed in 9 previously negative patients in which it showed a positive result.
Data was collected using Excel office. The obtained data were analyzed using IBM SPSS Statistics for Windows, Version 26.0. Armonk, NY: IBM Corp. Continuous variables were presented as Mean (± SD). Categorical variables were expressed as frequency (%) and compared using the Chi-square test. The degree of dependence of the variables was determined by the contingency coefficient Cramer's V. P-value was considered significant at less than 0.05.
All the patients had treatment with broad-spectrum antibiotics for SARS-CoV-2 infection for a period of 15 to 51 days, (26,7±9,47). The most common administered antibiotics were cephalosporines, fluoroquinolones and microlides. A little more than half (56,15%) of the study group population had a medical history of cardio-vascular diseases, diabetes mellitus type 2 and malignancies. *******On admission all the patients presented gastrointestinal symptoms – diarrhea, nausea and vomiting, diffuse abdominal pain, and cramping, loss of appetite. Fig. 1. The most common symptom was diarrhea – watery, greenish, foul-smelling stools up to 20 times a day (9,31±4,02) with onset 10 to 60 days (8±7,38) after Covid-19 infection. Diarrhea was mixed with mucus in 68 cases (56.2%) and blood in 19 cases (15.7%). All the patients were in general bad condition, intoxicated with clinical signs of dehydration II-III grade; about 50% of them had fever 37,3-39,4°C, (8±7,38). Loss of weight because of loss of appetite and dehydration had 60 patients (49,6%). Severe abdominal pain, general malaise and elevated inflammatory markers necessitated timely surgical evaluation in 8 patients (6.61%) - without the need for intervention. Elevated inflammatory markers and others laboratory findings were observed in all patients. Tabl. 1. We used the following laboratory values for assessing CDI severity: C-reactive protein – up to 367,1 μg/L; WBC count up to 29,4.109/L with left shift; low levels of serum Na+ and serum K+; high levels of serum creatinine in the course of oligoanuria. Low levels of serum protein and respectively serum albumin led to peripheral edema in 82 patients (67.8%) and anasarca in 3 patients (2.48%). Based on clinical presentation –hypotension, heart rate, dehydration and lab values we assessed the disease severity as follows: mild form in 40 patients (33,1%), moderate in 42 patients (34,7%) and severe in 39 patients (32,2%). The results, mainly confirmed by immunoenzymatic method in stool samples, showed toxin A (+) in 40 patients (33,1%), toxin B (+) in 22 patients (18,2%), toxins A and B (+) in 59 patients (48,8%), and GDH (+) in 63 patients (52,06%). Nine patients with previously negative samples were toxin positive when analyzed by RT-PCR. Antibiotics were the mainstay to treat CDI. All the patients were treated etiologically for 11-16 days, (13,82±6,21) the majority with Vancomycin 4x125 mg orally with Metronidazole 3x500 mg intravenously. Hospital stays varied from 2 to 28 days, (10±4,7). Reccurent symptoms occurred in 9 patients (7,43%) within 12-22 days, (10±7,82) after discharge. Candida albicans was detected in stool samples of 22 patients (18%). In-hospital mortality was 9,9% (12 patients). Pulmonary thromboembolism was the main cause of death in 2 patients, cardiac arrest – in 8 patients and acute renal failure – in 2 patients. The other patients were discharged with improvement.
| Laboratorial Indicators | Minimum | Maximum | Mean | SD |
| Leuc.(.109/L) | 1,21 | 32,6 | 12,82 | 6,73 |
| BUN (mmol/L) | 1,8 | 33,6 | 9,98 | 6,25 |
| Creatinine (μmol/L) | 32,3 | 502,14 | 135,67 | 83,41 |
| Total protein (g/L) | 22,1 | 80,2 | 55,62 | 10,55 |
| Albumin (g/L) | 11,2 | 50,8 | 30,43 | 7,49 |
| CRP (mg/L) | 30,2 | 362,3 | 139,44 | 88,13 |
| K (mmol/L) | 2,2 | 6,2 | 4,09 | 0,83 |
| Na (mmol/L) | 107,12 | 154,21 | 135,06 | 6,69 |
Table 1: Some laboratorial indicators in CDI
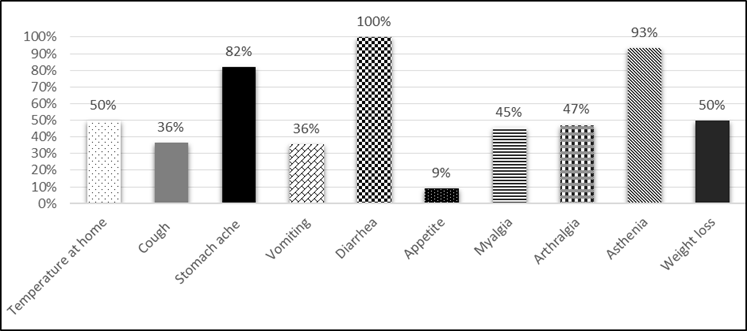
Figure 1: Spectrum of clinical manifestations in CDI.
The Covid-19 pandemic significantly impacted the healthcare systems worldwide. Now more than ever some open questions concerning CDAD need to be discussed. CD is a multi-resistant pathogen recognized as a leading cause of diarrhea associated with antibiotic treatment [11]. Age is considered one of the primary risk factors of CDI in general and especially for severe forms. Keller MJ at al. found that patients over the age of 65 were 10 times more likely to contract CD as younger in-patients in the same facility [12]. The mean age of our patients was 69,64±12,2 which corresponded to the statement that the elderly are more prone to CDI. It has been established that female are 1,5 times more likely than male to have CDI [13]. In our research, men have a slight preponderance - 56.19%. Diarrhea was the main symptom of all the patients of the studied cohort – profuse watery stools, which may be mixed more often with mucus than with blood. Diarrhea with such characteristics is described in the scientific literature as a cardinal symptom of CDI [14]. We registered mucus in 52,2% and blood in 15,7% of the cases. Most patients developed diarrhea during or shortly after starting antibiotics. Some individuals may not show symptoms for up to 8 weeks after completing therapy [15]. Patients who develop mild to moderate CDI commonly present with 3 or up to 10 loose stools in 24 hours. Mild abdominal pain, nausea and low-grade fever may be another symptom [16]. We registered such clinical manifestations in 33% of the cases. Clinical manifestations of severe form include profuse watery mucoid diarrhea as often as 10 to 15 times a day, dehydration, hypotension rapid heart rate, abdominal pain that may be severe. Fever up to 40˚C and WBC up to 50.109/L are markers for severe forms. Criteria proposed for severe CDI (based on expert opinion) include WBC count ≥15. 109/L and serum creatinine >133 mmol/L [17]. High levels of CRP, hypoproteinemia and hypoalbuminemia are another marker of severity [16]. 32,2% of our patients developed severe CDI. Fever up to 39,4˚C and elevated WBC count to 29,4.109/L were indicators for severity in our study. Protein-losing enteropathy with hypoalbuminemia may develop within the first days of clinical presentation of CDI [18]. We registered hypoalbuminemia in 82 patients (67,8%) resulting in peripheral edema. Three patients (2,48%) developed anasarca. All the patients of the studied cohort received massive antibiotic treatment for SARS-CoV-2 infection before admission, during hospitalization and after discharge. The median duration of antibiotic use was 26,7±9,47 days.
The antibiotic most frequently prescribed were cephalosporines second and third generation, fluoroquinolones, macrolides, and aminoglicosides. Some patients had concomitant therapy with two or three antibiotics. According to Rowson et al. 72% of the hospitalized patients with Covid-19 were treated with broad-spectrum antibiotics but only 8% had confirmed bacterial/fungal coinfection [19]. Our patients developed diarrhea as the main symptom of CDI within 10 to 60 days (8±7.38) days after the diagnosis of Covid-19, which coincides with the interval of 21 days reported in the scientific literature [20]. Severe CDI may be complicated with ascites, acute respiratory distress, toxic megacolon, acute heart failure, acute renal failure, liver abscessus, septic shock, cardiac arrest. Some patients may develop mental disorders [21]. Granata et al. reports for 28,9% severe cases with complications in their studies [14]. In our study those cases were in 11,57%. There was a lethal outcome in 12 patients (9,91%). The other patients were discharged with improvement. In recent years there is an increased global burden of CDI associated with increased morbidity and mortality. According to many studies hyper virulent clone of CD - ribotype 027 is associated with a great number of severe and fulminant cases [22]. Ribotypes were not detected in our study, so we could not associate the severity and the outcomes of CDIs with any ribotype. The diagnosis was based on clinical presentation suspectable for CDI and confirmed by detection of CD toxin in stool samples. Covid-19 can present with gastrointestinal symptoms similar to CDI, making it appropriate to consider both conditions in a patient with diarrhea. SARS-CoV-2 alters gut microbiota and discussed as a possible risk factor for CDI commensurate with overuse of antibiotics [23]. Candida albicans was detected in stool samples of 22 our patients (18,2%) with confirmed CDI. Antibiotics are mainstay to treat CDI. Treatment strategies should be based on disease severity, reccurence risk and comorbidities. Vancomycin is recommended for severe and complicated CDI. Methronidazole is recommended for mild to moderate disease. Both may be used in combination to treat severe CDI [24]. We applied treatment of CDI according to the cited generally accepted recommendations. Fecal microbiota transplant is a treatment for multiple recurrent CDI but its role in primary and severe CDI is not established [25]. Recently CDI increases and become less responsive to treatment [26] Relapses occurred in 9 (7,43%) of our patients within 12 to 22 days, (10±7,82) after dischargment. This percentage is lower than that reported in the literature - 15-20% [27]. The hospital stay was 10±4.73 days, which is consistent with the data published so far [28]. We found a correlation between length of hospital stay and fatal outcome. Cramer's correlation coefficient was used: Cramer's V=0.418, p=0.002. The relationship between the variables was checked by χ2 test and was statistically significant with p=0.003. However, we did not find such a relationship between the hospital stay and the severity of the clinical form of the disease, as well as between Clostridium difficile toxins and the outcome of the disease.
The identified risk factors for development of CDI correspond to the published data for the general population – overuse of broad-spectrum antibiotics, geriatric population, patients with suppressed immune system, comorbidities, delayed diagnose and admission in hospital. There is no correlation between the duration of antibiotic treatment, the patient age and the severity of CDI [29].
As limitations of the study, we can indicate the lack of PCR test for all cases included in the study, as well as identification of Clostridium difficile ribotypes.
Older people are more prone to CDAD. The average age of the studied cohort was 69.64±12.12 years with a slight male predominance. Any new onset of diarrhea after prolonged therapy for Covid-19 is suspicious for CDI. In the elderly, comorbidities of Covid-19, delayed diagnosis and therapy predict severe complicated CDI and increased risk of fatal outcome.
The authors declare that there are no conflicts of interest regarding the publication of this paper.
The study was conducted with funds from the scientific project 2021"Features in the spectrum, clinical course and outcome of respiratory viral infections in patients over the age of 65” at the Ministry of Health of the Republic of Bulgaria.
We thank all the doctors, nurses, laboratory staff and patients who participated in this work. We thank the staff of the Infectious Diseases Clinic of University Multiprofile Hospital for Active Treatment, Stara Zagora for their medical care and treatment.
Distribution of the involvement of the author team in the preparation of the manuscript:
1. Angelova S examined feces of patients with CDI for evidence of GDH, toxin A and toxin B.
2. Yordanova A carried out the statistical processing of the study data.
3. Parusheva P. and 4. Pekova L. collected the data from the patients, arranged them in a way convenient for statistical processing, made a literature review on the topic and prepared it for publication.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
