
Research Article | DOI: https://doi.org/10.31579/2690-1919/267
1 ème Pavillon A, Hôpitalnational de Niamey/Niger
2 èmé Service pédiatrie, HôpitalNational de Niamey/Niger
3 èmé Cardiologie, Hôpital Amirou Boubacar Diallo Niamey/Niger
4 eme Chirurgie Cardiovasculaire, Hôpitalgénéral de référencede Niamey/Niger
5 eme Service médecine interne,Hôpital général de référence deNiamey/Niger
*Corresponding Author: Hama Idrissa. ème Pavillon A, Hôpital national de Niamey/Niger
Citation: H Idrissa, I Adehossi, AM Maliki, Amadou H L, Amadou D, et al. (2022). Profile of Congenital Cardiopathies in Paediatric Departments A and B of the National Hospital Niamey National Hospital, J. Clinical Research and Reports, 11(4) DOI:10.31579/2690-1919/267
Copyright: © 2022 Hama Idrissa. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 12 August 2022 | Accepted: 25 August 2022 | Published: 25 September 2022
Keywords: congenital heart disease; national hospital of niamey; Niger
Aim: The aim of this study was to determine the extent of congenital heart disease in the population of children, for a better management and prevention strategy.
Materials and Methods: This was a descriptive and cross-sectional study over a period of 4 years 10 months from January 2016 to October 2020 (retrospective over 4 years and prospective over 10 months) at the National Hospital of Niamey; Were included in our study all patients aged 0 to 21 with congenital heart disease confirmed by cardiac ultrasound who were hospitalized or monitored externally. Our data were analyzed by Epi Info software in version 7.2.2.6. 24. Descriptive and analytical statistics were used: the mean with standard deviation (SD) (for normal distributive variations), odds ratio (OR) and the median (Me) for the description of asymmetric distributive values. The comparison of the proportions was also carried out; to do this we used the statistical test of chi2. The test is significant if p <0.05
Results: The gender ratio was 1.005 in favour of men. The median age of our patients was 16.8 months with extremes ranging from 0 months to 247 months, the most represented age group is 29 days to 24 months with 81.1%. The majority of our patients (62.4%) came from urban areas, parental consanguinity was present in 42.2% of cases.
55.3% of our patients had reported a notion of recurrent respiratory infection. Respiratory distress was found in 29.5% of cases, followed by fatigue during feedings (16.7%). Tachycardia was found in 72.2% of our patients, 49.6% were undernourished. Heart murmur was found in 80.3% of our patients, 4.4% had Down's syndrome.
Cardiomegaly was found in 64.4% of our patients, 15.7% had pulmonary hypervascularization.
CIV was found in 27.03% followed by T4F, CAV, and CIA with 20.39 respectively; 17.20 and 16.95%. Surgery was indicated in 68.3%.
Anemia was found in 55% of our patients, 49.6% had hyperleukocytosis. Antibiotic treatment was started in 72.7% of cases, 31.2% had benefited from diuretics, 23.8% from iron supplementation, 10.3% was on beta blockers. 18.7% had received surgical treatment, PAH and endocarditis were found in 1 and 0.73% of cases, respectively. 34.1% were awaiting surgery. The recorded death rate was 27.3%.
Conclusion: Congenital heart disease is becoming more and more frequent and constitutes a very important health problem in our pediatric departments. They are dominated by CIVs and T4s.
The diagnosis and their management are still difficult due to the lack of diagnostic and therapeutic means.
Congenital heart disease (CHD) is a very common cardiac abnormality that occurs during the formation of the heart during intrauterine life. These conditions have been defined as malformations of the heart and/or vessels present at birth related to a developmental abnormality. Also included are malformations related to the abnormal persistence after birth of structures present only during fetal life. They range from simple anomalies compatible with the growth of the child without major problems to severe malformations making it impossible for the new born to survive. [1].
The prevalence of congenital heart disease worldwide is estimated at 8 cases per 1000 live births, making it the most common malformation in children. In Europe, there are an estimated 5,000 new cases per year per 800,000 births. [2]
In Niger, CC is also very common. However, it should be noted that several factors hinder the diagnosis and management of these CCs, including the absence of obstetrical check-ups for various reasons (financial, material or cultural), and there is no national health programme concerned with the prevention of this defect which remains a public health problem in Niger [11].
Nowadays, in NIGER, cardiac malformations are better and better known thanks to the availability of Doppler ultrasound, which constitutes the basis of diagnosis.
The objective of this study was to determine the epidemiological and clinical profile of childhood CC in our paediatric department in Niamey.
The study took place in the paediatric wards of the National Hospital of Niamey. It was a retrospective, descriptive cross- sectional study over 4 years from 01 January 2016 to 31 December 2019 and a prospective cross-sectional study over 10 months from 01 January 2020 to 30 October 2020. We performed an exhaustive sampling; that is, we considered all patients diagnosed with congenital heart disease during the study period and meeting the inclusion criteria. The exclusion criteria were non malformative abnormalities. Pre-established survey form was used as a data collection tool. Our data were analysed Epi info 7 and Excel 2013 software. The statistical analysis used the chi2 test; the significance level of p was 0.05. The writing of our document and the making of our figures were carried out by the office software Excel and Microsoft office WORD 2013.
In 4 years and 10 months, 50238 consultations had been made, including 407 cases of congenital heart disease, i.e., a hospital frequency of 0.81%.
There was a slight male predominance with 50.1% of cases (gender ratio 1.005). Figure 1 shows the gender distribution. The median age of the patients was 16.8 months with extremes ranging from 0 months to 247 months. The most represented age group was 29 days to 24 months with 81.1%. The majority of patients (62.4%) came from urban areas.
Figure 1: Distribution of patients by gender
Consanguinity was present in 42.2% of cases. The pregnancies from which the children were born were full term in 94.1% of cases. The birth weight was between 2500 and 3999 in 37.3% of our patients. Repeated respiratory infections were reported in 55.3% of our patients.
The main reason forconsultation was respiratory distress (70.5%). Table 1 shows the distribution accordingto the different reasons for consultation.
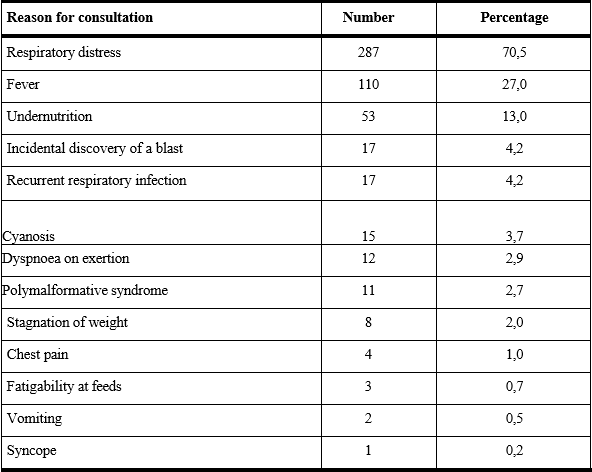
Table 1: Distribution of patients by reason for Consultation
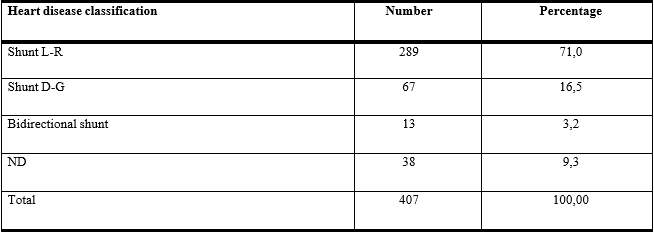
Table2: Distribution by type of shunt
On clinical examination, respiratory distress was the most common functional sign in 29.5% of cases, followed by fatigue during feedings (16.7%). Tachycardia was found in 72.2% of our patients and 49.6% had acute malnutrition. Heart murmur was the most common physical sign (80.3% of our patients). Trisomic facies was found in 4.4% of patients.
Radiological cardiomegaly was found in 64.4% of our patients and 15.7% had pulmonaryhypervascularisation. The left-right shunt accounted for 71%. Table 2 shows the distribution according to the type of shunt. VIC was the most represented ultrasound diagnosis in 27.03% followed by T4F, CAV, CIA with 20.39, 17.20 and 16.95% respectively. %. There was a statistically significant relationship between male sex and tetralogy of Fallot (P value: 0.01), female sex and atrioventricular canal (P value: 0.02).
On the haemogram, anaemia was found in 55% of patients and 49.6% had hyperleukocytosis. Antibiotic treatment was instituted in 72.7% of cases; 31.2% had received diuretics, 23.8% iron supplementation and 10.3% beta-blockers. Tables 3 and 4 illustrate the different treatments received. Four patients or 18.7% had received surgical treatment. PAH and endocarditis were found in 1% and 0.73% respectively. Most of the patients (34.1%) were awaiting surgery, the death rate recorded was 27.3%.
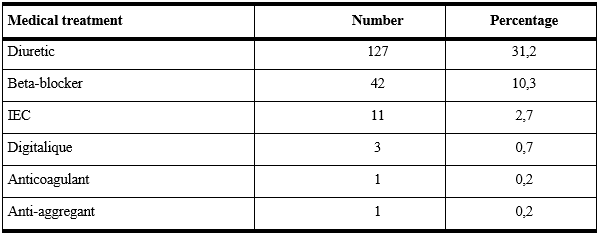
Table 3: Distribution of patients by specific medical treatment
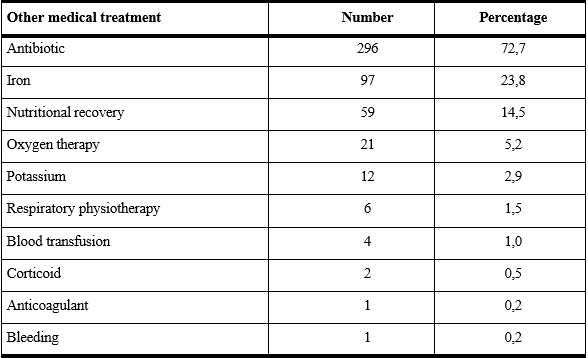
Table 4: Distribution of patientsby other treatments
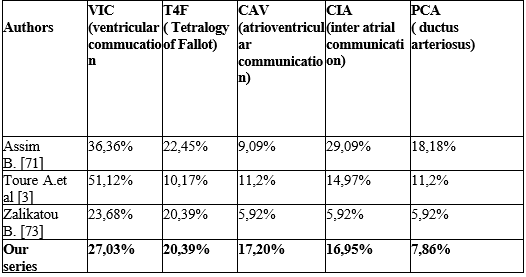
Table 5: Frequency of different types of CC according to the literature
Congenital heart disease is very common in paediatric hospitals. During the study, the prevalence was 0.81%. These results are close to those of Kinda George [3] in Burkina Faso in 2015 and Benbahia [4] in Morocco in 2018, but much lower than that reported by Oulhabib [5] in Morocco who found 7.7% in a neonatology department. These differences could be related to the following factors: difference in patient selection criteria, neonatal paediatric series in some studies [6] and finally ultrasound series [3].
Socio-Demographic Aspects:
Both sexes were involved with a slight male predominance of 50.1% with a sex ratio of 1.005. This result is similar to those of Benbahia [4] and Kinda G. [3]. On the other hand, Daou H. [7], Boubacar Z. [8] and Banou N. [6] found a female predominance. Despite this male predominance observed in the study and in most authors, there is no clear gender predominance.
The age range of 29 days to 24 months represented 81.1% which is close to that of Rantotiana R. [9] who found 84.31%, but higher than that of Kinda G. [3] who reported that most of the heart diseases (55%) were revealed at an early age (0 to 30 months). This high rate of CC in this age group could be explained by the fact that some CCs such as IVC, IAC, and PCA often have a spontaneous evolution towards closure; CCs of late discovery are most often benign and compatible with a quasi-normal life, which means that these patients do not consult and are often not recorded
The majority of our patients (n=254) came from urban areas, i.e. 62.4%. The same observation was made by Benbahia A. [4] and Boubacar Z. [8] with respectively 66% and 63.7%.
Parental consanguinity was found in 42.2% of our study, this rate is higher than those of Z Boubacar [10], Benbahia A. [4] and Banou N. [6] with respectively 26.97%;20.3%; 19%.
The age of the mothers was between26 and 35 years in 44.6% of the cases, which is lower than those of Benbahia A. [4] (52.40%) and Banou N. [6] (63%).
Pregnancy was not followed in 12.8% of our cases, which is lower than those of Daou H [7] in Mali (23.52%) and Oulhabib [5] in Morocco (54.50%).
A history of death in siblings was reported in 31.7% of cases. These deaths were not documented, but some occurred during the neonatal period in a context of respiratory distress according to the mothers. This result is higher than that of Z Boubacar. In Niger who reported a rate of 8.55% of cases. [10]. The literature reports that if a child has CC, the risk of recurrence in siblings is 2 to 3%. This risk can be as high as 10% if two previous children have a heart defect.
The patients were born by vaginal delivery in 86% of cases, a figure similar to that of Daou H[7] in Mali (82.35%).
The birth weight was between 2500 and 3999 g in 37.2% of the patients, which is lower than the result of Daou H. [7] (76.47%). Thisdifference could be explained by the fact that the birth weight was not determined in 48% of the patients.
Ninety-two (92) patients, i.e. 22.6%, had a delay in psychomotor development, a result similar to that of Rantotiana R. [9] who found 19.61%.
It should be noted that 55.3% of our patients had a history of repeated respiratory infections, which is higher than that of Rantotiana R. [9] in Antananarivo (23.53%).
Respiratory distress was the main reason for consultation with 70.5%, which was higher than the results found by Benbahia A. [4] in Morocco and Daou H. [7] in Mali who found 55 and 49.1% respectively, but lower than that of Rantotiana R. [9] in Antananarivo (96.08%).
Fatigue during breastfeeding was 16.7% which is lower than that of Benbahia A. [4] who found 67%. Excessive sweating was found in 6.9% of patients, which is similar to that of Rantotiana R. [9] (5.88%).
The heart rate was above 120 beats per minute in 72.3% of cases, which is higher than that of Benbahia A [4] in Morocco (56.3%).
Oxygen saturation was low (below 96%) in 39.8% of patients, which is close to that of Oulahbib [5] in Morocco (44%).
Acute undernutrition was found in 49.6%, which is higher than the result of Rantotiana R. [9] in Antananarivo (11.10%).
Heart murmur was the most common physical sign found in 80.3%, this result is close to those of Daou H.[7] in Mali; Rantotiana R. [9] in Antananarivo; and Z Boubacar.[10] in Niger who found respectively 84.31%; 86.70%, and 88.16%.
The trisomic facies was noted in 4.4% of cases, this rate is lower than those of Daou H. [7] (25.49%) and Banou N. [6] (23%).
On radiography, the cardiothoracic index was greater than or equal to 0.55 in 56.3% of cases, this result is superimposed on that of Daou H. [7] in Mali who found 54.91%. Pulmonary hypervascularisation was found in 15.7%, higher than those of Benbahia A. [4] in 2018 and
Oulahbib [5] in 2017 in Morocco who had respectively 6.55 and 2.5%. Pneumopathy was found in 13.5%, this result is lower than that of Noel B. [6] in Mali in 2020 (40%).
Ventricular septal defect was the most common cardiac anomaly found in 27.03%. This result is slightly higher than those of Zalika B [10] in Niger (23.68%) and Benbahia A. [4] in Morocco (25.80%). If studies are unanimous on the predominance of ventricular septal defects in congenital heart disease, they are less so on the frequency classification of the others [4, 10, 11]. Table 5 shows the frequency classification of heart disease in the literature. The left- right shunt was the most frequent with 71%, this rate is higher than that of Kamdem F. [12] in Cameroon who found 57.9%, but lower than that of Banou N. [6] in Mali (90%).
Anemia was found in 55% of the blood tests, higher than those of Boubacar Z. [8] in Niger and Banou N. [6] in Mali, who found 24% and 12% respectively.
The patients had benefited from a treatment based on diuretics, beta- blockers and antibiotics, these results are superposable those of Banou H.[6] Rantotiana R. [9] Benbahia A.[4]
Surgical treatment was performed in 18.7% of patients, this rate is lower than those of Rotantiana R. [9] in Antananarivo and Benbahia A. [4] in Morocco who found 37.26 and 23% respectively.
The complications found after medical treatment were PAH (1%) and infective endocarditis (0.73%). These results are lower than those of Benbahia A. [4] in Morocco (PAH: 15.67%; endocarditis: 1.42%).
A death rate of 27.3% was recorded during the study, which is higher than that of Benbahia A. [4] in Morocco who reported 13.70% was recorded during the study, which is higher than that of Benbahia A. [4] in Morocco who reported 13.70%. deaths.
The postoperative evolution was favourable in 68.9% of patients, against 20% of deaths; these results are similar to those of Benbahia A. [4] in Morocco who found 33% of deaths and 67% of favourable evolution after surgery.
Congenital heart diseases are increasingly diagnosed in our country. They are dominated by VICs but also by cyanogenic cardiopathies represented mainly by T4F. Diagnostic means are limited and rely essentially on echocardiography.
They pose a problem of surgical management especially in our developing countries, their evolution is therefore unpredictable, and more often than not marked by complications with a high mortality. The development of cardiac surgery in our country will be a giant step forward in the management of this sub-group of the population
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
