
case report | DOI: https://doi.org/10.31579/2690-1897/187
1Department of Surgery, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), PMB 5022, Awka. Anambra State, Nigeria.
2Department of Anatomic Pathology and Forensic Medicine, Nnamdi Azikiwe University, Awka. Anambra State, Nigeria.
*Corresponding Author: Nonso Mbah, Department of Surgery, Chukwuemeka Odumegwu Ojukwu University Teaching Hospital (COOUTH), PMB 5022, Awka. Anambra State, Nigeria.
Citation: Nonso Mbah, Felix E. Menkiti, (2024), Primary Tuberculous Mastitis in HIV Negative Patient: Case Report and Literature Review, J, Surgical Case Reports and Images, 7(3); DOI:10.31579/2690-1897/187
Copyright: © 2024, Nonso Mbah. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 10 April 2024 | Accepted: 18 April 2024 | Published: 25 April 2024
Keywords: Breast lump; Tuberculous mastitis; Cold abscess; Surgical management
Tuberculous mastitis is a rare condition even in regions where tuberculosis is endemic. The clinical presentation closely resembles that of breast cancer with which it is often confused. Commoner risk factors are lactation, immunosuppressive state and women in their reproductive age group, between 20 - 40 years age range. Tissue histology provides definitive diagnosis even when other forms of confirmation are either negative or unavailable. Surgical procedure is required for the drainage of accompanying cold abscess. Response to anti-tuberculous therapy is very favourable.
Tuberculous mastitis (TM) is an uncommon disease in the general population, unlike the simple bacterial mastitis.1 It is rarer among patients who neither have pre-existing tuberculosis elsewhere in their body nor immunosuppressive conditions such as the HIV/AIDS.2 The incidence ranges from 0.1% to 4%, being commoner in developing countries where tuberculosis is highly endemic. The low incidence of tuberculous disease of the breast in general is believed to be due to increased breast tissue resistance to the survival and multiplication of the causative Mycobacterium tuberculosis bacilli, the use of anti-tuberculous treatment, and the under-diagnosis of TM.3
This case is reported to raise awareness of TM as an important differential diagnosis in a young, HIV-negative, lactating, primiparous woman who presented with a painless, non-resolving breast lump, in the absence of any obvious pre-existing tuberculous disease elsewhere.
Mrs C.A.M, 25years old primiparous lady, presented at the general surgery outpatient clinic in October 2023 with 3-months history of painless lump in the right breast. She was nursing her 6-month old baby from both breasts at the time of her first hospital presentation. The patient denied any preceding history of trauma to the affected breast. She did not have any past history of breast condition or any family history of breast disease. There were no systemic symptoms or weight loss. She had evacuation of retained products of conception 5 days after her child birth, otherwise her past surgical and medical history were unremarkable.
Clinically, the general physical health and vital signs were satisfactory. Her BMI was 24.4kg/m2 (weight 64kg, height 162cm). The breasts appeared symmetrical. The left breast and axilla were unremarkable. There was a large non-tender mass at the upper outer quadrant of the right breast, firm to hard in consistency, measuring approximately 6 cm in its widest axis. The overlying skin was intact and normal. There was no demonstrable fixity of the mass to the skin or underlying chest wall. The nipple was not retracted. The right axillary lymph nodes were palpably enlarged, discrete, mobile and non-tender. Ultrasonography of the right breast showed the presence of a focal ill-defined heterogenous dominantly hypoechoic collection with hyperechoic core seen within it (fig. 1). Multiple enlarged lymph nodes without fatty hilum were also noted in the right axilla (fig. 2). The sonologist’s conclusions were puerperal mastitis or breast abscess, with right axillary lymphadenopathy.
Her viral markers for HIV, Hepatitis B and C were negative. The PCV was 32% and the WBC was 3.7x109/L.
She had drainage of the cold abscess and wide local excision of the lesion 1-month after discontinuation of breast feeding. Intra-operatively, the mass consisted of breast tissue which was studded all over the surface with numerous tiny tubercles of various sizes (fig. 3). This mass contained a pale yellow cheesy fluid of thick consistency, which was drained and sent for Ziehl Neelsen staining, mycobacterial and microbial cultures. The residual breast cavity was copiously irrigated with normal saline solution before closure. No drain was placed.
The mycobacterial culture and Ziehl Neelsen stain were negative for acid fast bacilli.
The histology report revealed an extensive caseating granulomatous chronic mastitis. The uninvolved adjacent breast tissue showed lactation changes. No malignancy was identified. The histology report confirmed Tuberculous mastitis (fig. 5).
She was commenced on initial 2-month course of antituberculous treatment comprising daily doses of oral Isoniazid 300mg, Rifampicin 600mg, Pyrazinamide 1,500mg, Ethambutol 800mg and Pyrazinamide 50mg, to be followed by the continuation phase with Isoniazid and Rifampicin thereafter.
The patient had an uneventful post-operative course. The surgical wound healed nicely by primary intention within 2-weeks of operation (fig. 4). The axillary lymph nodes had not shown significant regression by 2-months post commencement of the anti-tuberculous therapy.

Figure 1: Sonomammography showing abscess collection within the solid mass lesion in the right breast
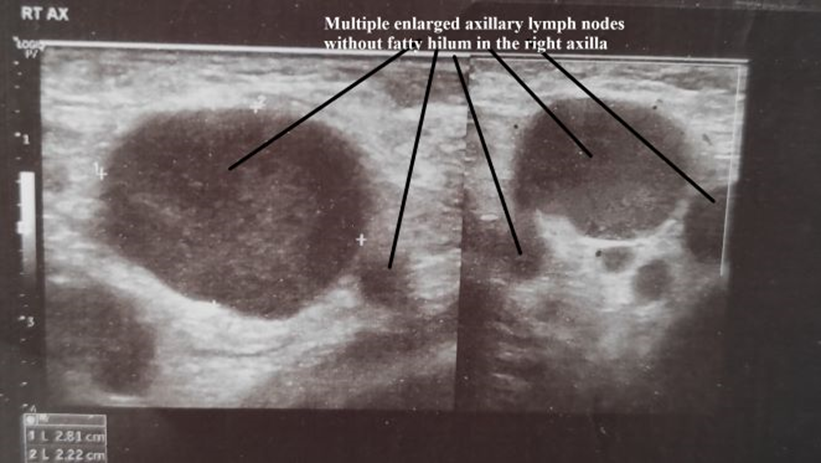
Figure 2: Ultrasonography showing multiple discrete enlarged right axillary lymph nodes.
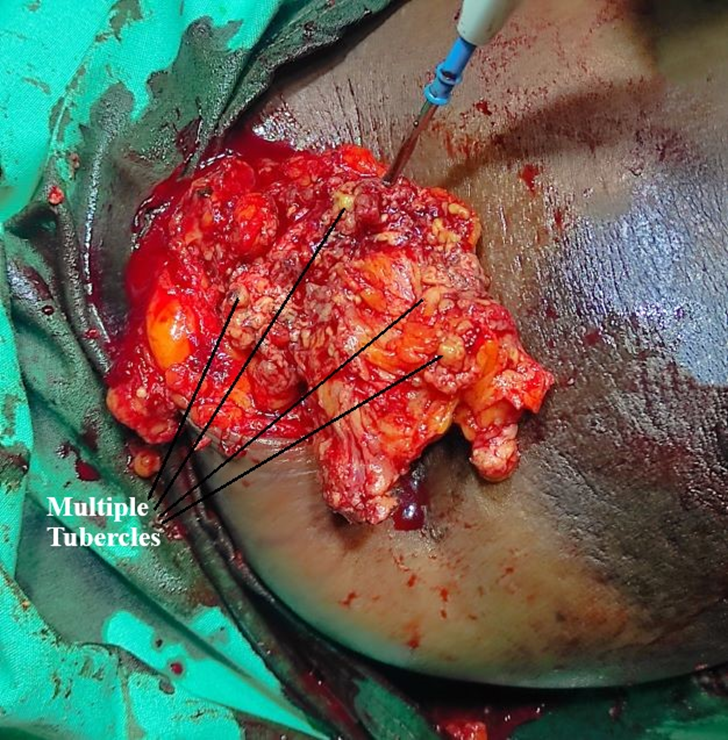
Figure 3: Excision of breast tissue studded with numerous tubercles for histology.

Figure 4: Post-operative wound healing by primary intention on the right breast.
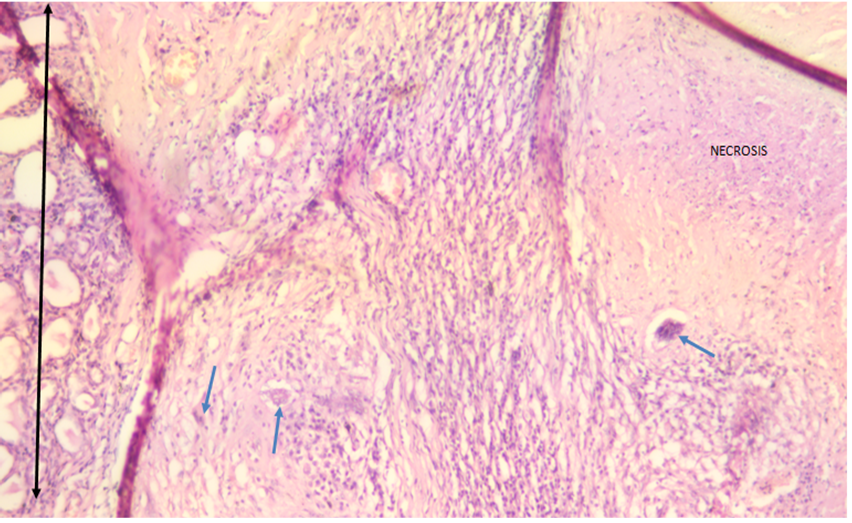
Figure 5: Section of right breast tissue showing a necrotizing inflammatory lesion characterized by numerous granulomas having central structureless necrosis and composed of epithelioid macrophages admixed with inflammatory giant cells (blue arrows) and rimmed by lymphocytes. Two-headed black arrow shows lobule of breast ducts with lactational changes. (H&E X100).
Tuberculous mastitis or breast tuberculosis is a rare form of extra-pulmonary tuberculosis. It accounts for less than 0.1% of breast pathologies and 3 - 4.5% of breast diseases requiring surgery in developing countries.4 Primary tuberculous mastitis (TM) is when the breast is the only tissue affected by the tuberculous disease. It is much less common than secondary TM which occurs when the infection spreads to the breast from a focus in another affected body organ.5 It is generally believed that TM is usually secondary to a pre-existing tuberculous focus located elsewhere in the body such as the lungs or lymph nodes. Consequently, the diagnosis of primary TM may arise because the clinician, radiologist and pathologist were unable to detect the location of the true focus of the disease at another body site. The patient presented in this report did not exhibit features of tuberculosis elsewhere and therefore was considered to have primary TM.
Sir Astley Paston Cooper in 1829 gave the earliest description of breast tuberculosis.6 The relationship of the condition to lactation is quite established. The increased incidence of TM in pregnancy and lactation may be attributable to the increased vascularity and dilation of breast ducts which predispose them to trauma and therefore tuberculous infection. Majority of cases are seen in females who have born children, who are between the ages of 20 and 40 years. Breast tuberculosis has therefore been considered the “younger woman’s disease.”7 Other risk factors are breast trauma, previous history of suppurative mastitis, malnutrition and HIV/AIDS.2 The patient’s general health in cases of primary TM is remarkably good. This certainly is not true of the secondary type where the breast condition merely represents yet another threat to the survival of a patient already in jeopardy from long-standing infection in some other site or sites.8 Our patient did not have any obvious breast trauma or underlying malnutrition, previous suppurative mastitis and HIV/AIDS. This implies that the absence of these other risk factors does not absolutely exclude a patient from having TM.
Mammary tuberculosis may present in diverse ways. Rarely are the typical constitutional symptoms of tuberculosis seen in the patients, namely fever, anorexia, night sweats or weight loss. These were absent in
our patient. Rather, TM commonly manifests as a painless or painful breast mass, breast abscess with or without multiple discharging sinuses or as an ulcerated breast lesion. Its other clinical presentations include nipple retraction, peau d’orange skin changes, breast deformity, induration of the overlying skin of the breast, axillary lymph node enlargement or ulcerated axillary lesion.5,8 The similarity between the clinical features of TM and those of the more rampant breast malignancy particularly, as well as those of other disease conditions of the breast earned the former the monika “the great masquerader” or “the great mimicker”.9,10 In the index patient, the finding of a painless mass lesion in an otherwise healthy-looking breast, and the presence of palpably enlarged ipsilateral axillary lymph nodes made breast malignancy our primary concern. Unfortunately, there are no pathognomonic symptoms or signs to differentiate breast tuberculosis from breast cancer, until the lesions are subjected to histological examination. Pujani et al cautioned that the recognition of TM does not exclude the presence of concomitant breast carcinoma because there have been infrequent reports of double synchronous pathology with both tuberculosis and malignancy occurring in the same breast and axillary nodes.11,12,13
The ultrasound finding of abscess collection within the lesion in our patient widened the scope of our differential diagnosis to include pyogenic abscess from simple bacterial infection,which invariably necessitated an open surgical drainage, tissue biopsy, Ziehl Neelsen staining, mycobacterial and microbial cultures.
McKeown and Wilkinson in1952 originally described five histological types of mammary tuberculosis namely the nodular tuberculous mastitis, the disseminated tuberculous mastitis, the sclerosing tuberculous mastitis, the tuberculous mastitis obliterans and the acute miliarytuberculous mastitis.14 However, current classification has narrowed the histological variants to only three. They are the nodular, diffuse and sclerosing.5The nodular caseous form is a well circumscribed, slowly growing, painless solid lesion and could hardly be differentiated from a fibroadenoma or malignancy. It’s the commonest type of TM which is considered to manifest in individuals with high immunity and low disease virulence. Our patient presented with this form of the disease. The diffuse or disseminated variety is characterized by multiple lesions which could lead to caseation, ulceration and discharging sinus tract formation. It often affects a large area or even the entire breast. This type is the second most common form of TM and represents a more virulent tuberculous infection in a patient whose immune response is low, which is typically seen in cases with the HIV/AIDS. The sclerosing variety is characterized by extensive fibrosis with no caseation or suppuration, in which the entire breast is hard, shriveled and the nipple is retracted. It is the least common of the three types, slow growing and most commonly seen in elderly women.3,4
The confirmatory diagnosis of TM is by histology or fine needle aspiration cytology (FNAC). Incidentally, adequate tissue samples are not possible with FNAC. Therefore surgical management is best advocated not only to drain any coexisting cold abscess as in the case presented, but also to obtain tissue biopsy in order rule out other differential diagnosis of TM such as malignancy, simple bacterial mastitis, idiopathic granulomatous mastitis, sarcoidosis, traumatic fat necrosis, duct ectasia and fungal infections like actinomycosis.9
Mammary tuberculosis is paucibacillary.4.15 Consequently, investigations such as mycobacterial culture of the breast lesion and Ziehl Neelsen staining for AFB are often negative as was observed in our patient, and elsewhere.15,16 Likewise, sophisticated test like nucleic acid amplification test using polymerase chain reaction (PCR), although rapid and specific, has a low yield for the bacilli.16
Although imaging studies such as ultrasound scan, mammography, magnetic resonance imaging (MRI) scan and computerized tomography (CT) scan are not specific for TM, they are however invaluable in the evaluation of the patient.7 They may reveal the presence and location of an abscess collection, as well as the extent of spread of the lesion including axillary lymphadenopathy, as was observed in our index patient. Makanjuola et al., described the peculiar mammographic finding of “skin bulge and sinus tract sign” in patients with TM.17 Incidentally, mammography was not employed for the diagnostic evaluation of our patient because she was younger that the minimum eligibility age of 40 years.
The definitive treatment and prognosis of tuberculous mastitis differ greatly from that of breast malignancy which remains its closest differential diagnosis. Like pulmonary and other extra-pulmonary tuberculosis, the mainstay of treatment for primary TM is medical, with the same statutory anti-tuberculous regimen.18It is given over a period of 6 to 18 months and achieves cure for most (≥95%) cases of mammary tuberculosis. Common regimen consists of 2-months initiation phase with the combination of daily doses of oral Isoniazid 300mg, Rifampicin 600mg, Pyrazinamide 1,500mg, Ethambutol 800mg and Pyridoxine 50mg. Thereafter, continuation phase follows with only Isoniazid and Rifampicin for the remaining duration of therapy depending on the protocol in place. With this regimen, our patient’s surgical wound healed primarily. The expectation is that the disease would have completely resolved by the end of the full course of treatment.
Surgical procedures are adjunctive in the management of primary TM. The indications include the drainage of cold abscess which may be located in either in the breast or axilla or both. Surgery is also required for biopsy of the lesion in order to establish an accurate tissue diagnosis, or for axillary dissection in patients with large ulcerated nodes or for the removal of large painful ulcerative lesions.3 The dual benefits of operation in our patient were to drain the cold abscess as well as provide tissue for histological diagnosis. Simple mastectomy is an extreme surgical option which is rarely needed in the modern era. It is now reserved for patients with extensive disease comprising large painful ulcerated mass involving both the entire breast and the draining axillary lymph nodes.5
In conclusion, the ultrasound finding of an abscess collection in a young lactating woman with palpable breast and axillary lumps in the tropics should prompt the consideration of TM as a foremost differential diagnosis. Histology remains the corner stone of the definitive diagnosis. The clinical outcome from conventional anti-tuberculous treatment is favourable.
Written informed consent was obtained from the patient for the publication of this case report and the accompanying images.
The authors declare no competing interests.
Nonso Mbah was the consultant General Surgeon who managed the patient. He provided the clinical images and wrote the Abstract, Case presentation and Discussion. Felix Menkiti was the consultant histopathologist who provided the micrograph and wrote the Introduction part of the article. Both authors reviewed and approved the final version of this manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
