
Case Report | DOI: https://doi.org/10.31579/2690-4861/020
1 MBBS, M.Phil Research Fellow (Histopathology) Lecturer, Department of pathology, DMC, Dow university of Health Sciences, Karachi, Pakistan.
2 MBBS, FCPS, PhD Research Fellow (Histopathology) Professor, Department of pathology DIMC, Dow University of Health Sciences Karachi, Pakistan.
*Corresponding Author: Yusra Shafique, MBBS, M.Phil Research Fellow (Histopathology) Lecturer, Department of pathology, DMC, Dow university of Health Sciences, Karachi, Pakistan.
Citation: Yusra S, Uzma B. (2020) Primary Squamous cell carcinoma of prostate: A diagnostic dilemma. International Journal of Clinical Case Reports and Reviews. 2(4); DOI: 10.31579/2690-4861/020
Copyright: © 2020 Yusra Shafique, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 14 March 2020 | Accepted: 18 June 2020 | Published: 24 June 2020
Keywords: squamous cell carcinoma; prostate; diagnostic dilemma
Prostate squamous cell carcinoma is a rare entity with poor prognosis and it should be considered in patients with normal PSA ranges and symptoms of urinary obstruction.
Prostate carcinoma is the most common malignancy among male population. [1] Majority of cases are diagnosed as adenocarcinoma. Pure squamous cell carcinoma is a rare entity representing less than 1% of prostate carcinoma.[2, 3] It usually occurs in 7th decade of life with symptoms of urinary obstruction and bone pain in case of bone metastasis.[1, 4] About half of the cases arise post hormonal or radiation therapy to prostate adenocarcinoma, however de novo cases with no history of prostate disease have been reported in patients.[5] These findings suggest multiple etiologies for this disease. There are many hypothesis such as squamous differentiation in prostate cancer originates from urothelial lining of prostatic urethra or urothelial ducts. Other suggests that pluripotent stem cells being multi directional can give rise to it.
Morphologically squamous differentiation in prostate cancer can be encountered in pure form or in association with adenocarcinoma, urothelial carcinoma or sarcoma. Due to its multiple possible origins it is difficult to determine whether the squamous component develops through divergent differentiation from adenocarcinoma following treatment, represents squamous differentiation of transitional cell carcinoma or is a pure prostate malignancy.
As this is an aggressive malignancy with poor prognosis than adenocarcinoma and it metastasizes early to bone, liver and lungs so understanding the biology of this tumor might help to develop more efficient therapies.[2]
We discuss our findings for this case to help pathologists encountering the same problem.
An 80 years old male presented in our institution hospital with clinical sign and symptoms of acute urinary retention complaining of voiding difficulties for 3 months. Patient had past history of hemorrhoidectomy with no co-morbids. Physical examination was unremarkable. Digital rectal examination demonstrated an enlarged, fixed prostate, firm in consistency. On cystoscopy urinary bladder appeared normal. No lesion was seen. No history of radiation, hormonal therapy or tumor was given on any other site.
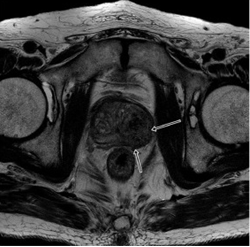
MRI scan shows low signal intensity mass lesion in left peripheral and transition zone. (Figure 1)
Serum PSA and PSAP levels were in normal range (1.2ng/ml). TURP- guided biopsy of prostate was performed due to urinary obstruction, in which 20gm of prostatic tissue was removed and sent for histopathology.
Histopathological findings:
Grossly specimen was in form of multiple grey white prostatic chips measuring in total of 20gm. Microscopic sections from prostatic tissue revealed an infiltrating neoplastic lesion arranged in clusters and nests. Cytologically individual tumor cells were large and cohesive with vesicular nuclei, prominent nucleoli, abundant glassy eosinophilic cytoplasm and well defined cell borders. Individual cell keratinization and keratin pearl formation was seen. Perineural invasion was noted. No other differentiation was seen. (Figure 2)

Prostatic squamous cell carcinoma is a rare pathologic and clinical entity accounting for 0.6-1% of all prostate malignancies. Its histiogenesis is not well understood. In more than 50% of cases it occurs post radiation and post hormonal treatment for adenocarcinoma of prostate. [4, 5]
Several theories have been proposed to explain histiogenesis of primary squamous cell carcinoma. It may arise from squamous metaplasia developing due to metaplastic transformation of adenocarcinoma, collision tumor arising from metaplastic foci post radiation or post hormonal therapy and possible deviation from pluripotent stem cells capable of multidirectional differentiation.[6, 7] It has been postulated squamous component arises from squamous metaplasia of basal or reserve cells of acini and ducts which can be due to different causes including chronic prostatitis, infarction, post radiation and post hormonal prostate or urothelial carcinomas.[1, 7, 8]
Strict criteria proposed by Mott indicates that in order to diagnose a prostate biopsy as pure squamous cell carcinoma that includes clear malignant features (such as disorganized growth pattern, cellular aplasia, invasion) features of squamous differentiation including keratinization, squamous pearls and distinct intercellular bridges, lack of glandular/ acinar component, absence of primary squamous cancer elsewhere particularly within the bladder.[9]
Clinical features pointing towards diagnosis of squamous cell carcinoma includes low serum PSA and acid phosphatase levels so they have limited value in diagnosis.[3]
We report a case of pure squamous cell carcinoma of prostate and unlike most of the cases previously reported our case lacked pre-existing history of hormonal or radiation therapy. Primary squamous cell carcinoma has poor prognosis so in cases where PSA levels are not significantly raised and have obstructive urinary symptoms it should be considered in differential diagnoses.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
