
Case Report | DOI: https://doi.org/10.31579/2690-4861/690
1 Doct. of Med. Scien., Professor, Academic Secretary, A.V. Vishnevsky National Medical Research Center of Surgery, Bolshaya Serpukhovskaya st., 27, Moscow, 115093, Russia.
2 Cand. of Med. Sci., Associate Professor of Educational Department, Surgeon of Abdominal Surgery Department, A.V. Vishnevsky National Medical Research Center of Surgery, Bolshaya Serpukhovskaya st., 27, Moscow, 115093, Russia.
3 Surgeon of General and Endocrine Surgery Department of A.L. Mikaelyan Institute of Surgery, Ezras Hasratyan St., Bldg. 9, Yerevan, 0052, Armenia.
4 Doct. of Med. Scien., Professor, Head of the surgical clinic EMC, Shchepkina st., 35, Moscow, 129090, Russia.
*Corresponding Author: Stepanova Yulia Aleksandrovna, Doct. of Med. Scien., Professor, Academic Secretary, A.V. Vishnevsky National Medical Research Center of Surgery, Bolshaya Serpukhovskaya st., 27, Moscow, 115093, Russia.
Citation: Stepanova Y. Aleksandrovna, Ionkin D. Anatolevich, Ayvazyan K. Akopovich, Zhao A. Vladimirovich, (2025), Primary Hepatic Lymphoma in Pregnant: Clinical Case and Literature Review, International Journal of Clinical Case Reports and Reviews, 24(3); DOI:10.31579/2690-4861/690
Copyright: © 2025, Stepanova Yulia Aleksandrovna. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 17 January 2025 | Accepted: 27 January 2025 | Published: 18 March 2025
Keywords: primary liver lymphoma; pregnancy; etiology; clinical picture; diagnostics; ultrasound; MSCT; MRI; treatment; features
Primary hepatic lymphoma (PHL) is an extremely rare disease that presents with non-specific symptoms and variable laboratory and imaging findings. It should be part of the differential diagnosis in a patient with nodular liver lesions, especially in the presence of normal tumor markers and/or elevated LDH levels.
A clinical case of a 29-year-old pregnant woman who complained of intermittent pain in the right hypochondrium for six months is presented. Blood biochemistry during control tests at pregnancy were within normal values. The patient didn’t undergo abdominal ultrasound during pregnancy. According to the abdominal ultrasound, the lesions of the SII-III and SVI-VII liver were detected 24 hours before the timely natural birth. During the control abdominal ultrasound the next day after delivery, these focal lesions were confirmed and extrahepatic fluid accumulation was detected in the area of SVI-VII liver lesions localization. Morphological diagnosis was not made before surgery. The patient underwent staged surgical treatment, after which she was referred for consultation to a hematologist. Additional histology and PET-CT were performed. The diagnosis was confirmed: diffuse large B-cell primary non-Hodgkin's liver lymphoma, IVA according to Cotswolds-modified Ann Arbor. The patient receives adjuvant chemotherapy.
Thus, morphology verification is mandatory for the final diagnosis of PHL. It is important to recognize PHL, since this disease is sensitive to chemotherapy, and its timely diagnosis allows for early treatment and improves overall survival.
Literature data on the relationship between PHL and pregnancy are extremely scarce, there is a single case where the fact of such possibility is noted.
In 1666, Marcello Malpighi described “a disease of the lymphatic glands and spleen, which was invariably fatal,” the first documentation of lymphoma. Almost 200 years later, in 1828, Dr. Robert Carswell exhibited a collection of drawings and paintings of his patients, including one that caught the attention of his friend, Dr. Thomas Hodgkin. Hodgkin noted, “…one struck me as representing a greatly enlarged spleen, studded with large tubercles of a rounded shape and light color. I recognized [it] at once….” In 1832, Hodgkin collected seven case reports, including Carswell’s patient, and published “On Some Morbid Manifestations of the Sucking Glands and Spleen,” offering the first formal description of the pathological characteristics of lymphoma. These initial descriptions and illustrations prompted Samuel Wilkes in 1865 to examine pathological specimens and christen the clinical diagnosis Hodgkin's disease (now Hodgkin's lymphoma) (cited in Wijetunga N.A. et al. [1]). Although consensus on the classification of Hodgkin's lymphoma was quickly reached, there remained a large group of very different diseases requiring further classification. The Rappaport classification, proposed by Henry Rappaport in 1956 [2] and 1966 [3], became the first widely accepted classification of lymphomas other than Hodgkin's lymphoma. Non-Hodgkin's lymphomas (lymphosarcoma) (a term proposed in 1972 by Jones S.E. et al. to denote malignant diseases of the lymph nodes, with the exception of malignant lymphogranulomatosis - Hodgkin's disease [4]) are malignant neoplasms of lymphoid and hematopoietic tissues and represent a group of diseases with different clinical and morphological manifestations.
Isolated liver lymphoma is an extremely rare, difficult to diagnose lymphoproliferative disease. Primary hepatic lymphoma (PHL) was first described in 1965 by A. Ata et al. [5]. In 1986, D. Caccamo et al. characterized the disease as an isolated organ lesion in the absence of other manifestations of the tumor process (i.e., other localizations), including enlarged lymph nodes, splenomegaly, abnormal hematological parameters and/or signs of bone marrow damage, for at least six months after the detection of liver damage [6].
PHL accounts for about 0.016% of all non-Hodgkin's lymphomas, 0.4% of all primary extranodal lymphomas and 0.1% of all malignant liver tumors [7, 8]. At the same time, liver damage in generalized stages of non-Hodgkin's lymphomas is observed in 16-22% of patients [9].
More than 90% of PHL originate from B-cells, T-cell lymphomas (peripheral, anaplastic, hepatosplenic) are extremely rare. Among B-cell PHL, diffuse large B-cell lymphoma accounts for up to 96%, cases of MALT lymphoma, Burkitt's lymphoma with primary liver damage have been described [7, 8, 10-12]. Clinical signs of PHL are nonspecific (the so-called B-symptoms - fever, weight loss, night sweats, abdominal pain and jaundice), which determines the high frequency of errors at the stage of establishing the diagnosis and a long history in most patients. The rapid course of the tumor with the development of hepatic encephalopathy and coma is characteristic. Death often occurs before the start of specific treatment and the diagnosis is established at autopsy [13].
The etiology of PHL is unclear. It is known that normally there is a strong local specific NK-cell immunity in the portal tracts of the liver, which may explain the fact that lymphatic tumors in the liver develop very rarely. High frequency of infection with viral hepatitis C (HCV) is noteworthy: in 60-70% of patients with PHL, according to various authors, HCV markers are detected, which is considered one of the causes of tumor development. Possible triggers include other infections, viral hepatitis C (HCV), HIV and Epstein-Barr virus, as well as chronic liver diseases (primary biliary cirrhosis), autoimmune diseases, immunosuppressive therapy after organ transplantation. The mechanism of lymphatic tumor development presumably consists in the occurrence of insufficiency of the T/NK-cell link of immunity. As a result of the breakdown of local T/NK cell control in the liver, proliferation of B lymphocytes is induced, which with a high probability leads to the development of a lymphatic tumor [7, 8, 10-12]. Thus, the data presented in the literature indicate that chronic antigen stimulation apparently plays a role in the initial development of PHL. The occurrence of PHL after liver transplantation in a recipient [14] is most likely associated with the continued proliferation of B-lymphocytes, which are normally inhibited by T-lymphocytes, against the background of immunosuppressive therapy [15]. According to E.J. Steller et al., PHL was associated with recipients of solid organ transplants, occurring in 4% of cases [11].
Due to the rarity of PHL, it is advisable to accumulate data on various manifestations of the disease. We present a clinical case of PHL detected against the background of pregnancy of the women who underwent treatment after a timely natural birth.
Patient K., 29 years old, was admitted to A.V. Vishnevsky National Medical Research Center of Surgery with complaints of periodic pain in the right hypochondrium in January 2021.
Anamnesis vitae. The patient has subclinical hypothyroidism (takes sodium levothyroxine), underwent appendectomy (2004).
Anamnesis morbi. Since August 2020, the women has been bothered by periodic pain in the right hypochondrium. According to the abdominal ultrasound (12.12.2020), the lesions of the liver SII-III and SVI-VII were revealed. On 12.13.2020, timely natural birth was performed without any peculiarities. A control abdominal ultrasound on 12.14.2020 confirmed focal liver lesions, and a fluid accumulation was detected in the area of the liver SVI-VII lesion localization. On 12.15.2020, the women underwent an MRI of the abdominal organs: the lesion of the liver SVI-VII with a subcapsular fluid accumulation (adenoma rupture?) adjacent to the anterior abdominal wall was detected (Fig. 1), as well as the lesion of the liver SII-III (Figure. 1a). The lesions had a hyperintense signal in the center and a hypointense signal at its periphery on T2-weighted imaging.
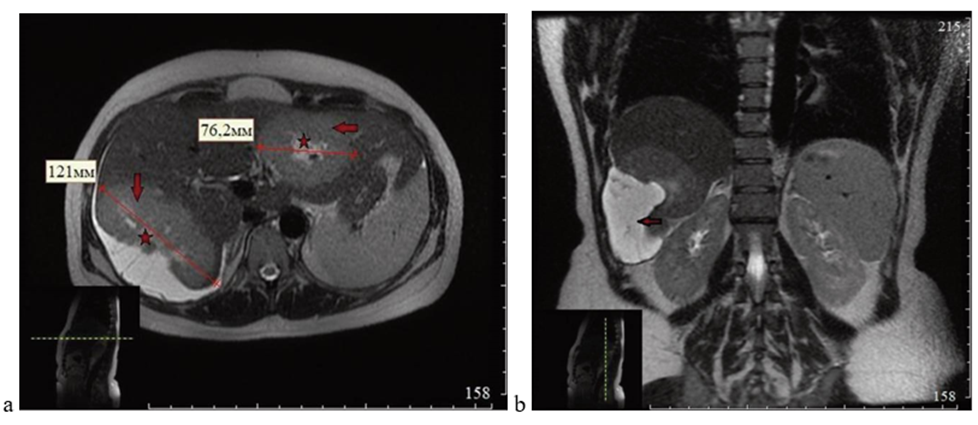
Figure 1: MRI, T2-weighted image: a - axial projection, solid lesions of the liver SII-III and SVI-VII with hyperintense signal in the center (asterisks) and hypointense signal at the periphery (arrows) of the lesions; b - frontal projection, solid lesion of the liver SVI-VII with hyperintense subcapsular fluid accumulation (arrow)
Subsequently, the woman was consulted via telemedicine technologies (Prof. Zhao A.V.), it was decided to perform embolization of the liver SVI-VII feeding arteries and planned surgical treatment at A.V. Vishnevsky National Medical Research Center of Surgery (anatomical resection of the liver SVI-VII and SII-III). On December 17, 2020, X-ray endovascular embolization of the liver SVI-VII feeding arteries was performed (Figure. 2), after which the patient was discharged in a satisfactory condition.
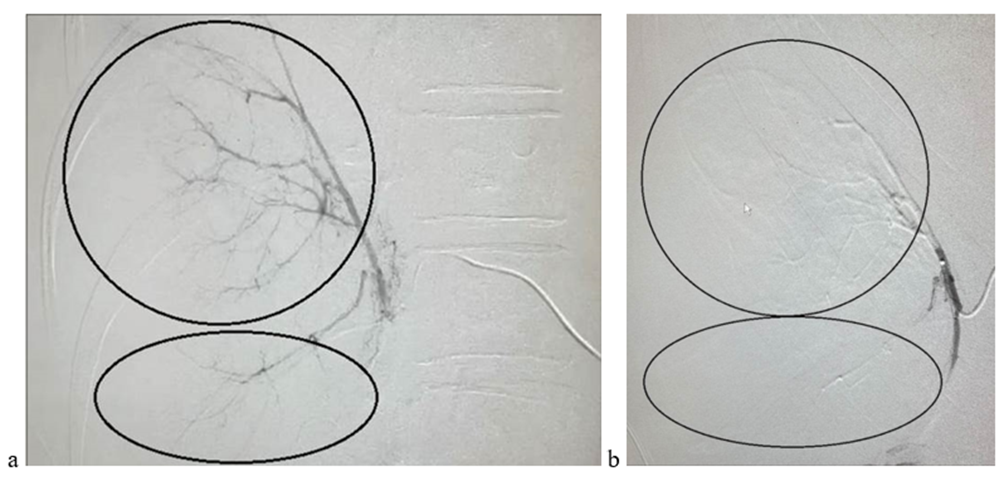
Figure 2. Angiograms before embolization of the feeding arteries of the liver SVII (a)
(area in circle) and SVI (area in ellipse) and after embolization (b)
However, on 01.08.2021, the woman developed sharp pain in the right hypochondrium radiating to the lower abdomen. An ambulance team took her to the emergency room of the city hospital at her place of residence, where an abdominal ultrasound revealed free fluid, after which laparocentesis was performed - 100 ml of light serous fluid was obtained. The next day, the woman was discharged in satisfactory condition.
On 01.15.2021, the woman was hospitalized at A.V. Vishnevsky National Medical Research Center of Surgery for planned surgical treatment.
Physical examination didn’t reveal hepatomegaly and lymphadenopathy of the superficial lymph nodes. Routine laboratory tests are unremarkable, with the exception of mild anemia (116 g/l). The test for the presence of infection (HBV, HCV, HIV) is negative.
The patient underwent surgery: anatomical resection of the liver SVI-VII and SII-III-IVa (01.19.2021). Intraoperatively: during revision of the abdominal cavity, no pathological changes were found in the stomach, pancreas, duodenum, small and large intestines, spleen, kidneys, para-aortic lymph nodes, ovaries, fallopian tubes and uterus, the parietal peritoneum is without signs of dissemination.
In the right subdiaphragmatic space and in the right lateral canal in the projection of the right lateral section of the liver, there is the lesdion, measuring 15×3 cm, with transparent fluid (Figure. 3a), which is associated with a subcapsular lesion in the liver SVI-VII of a whitish color, with a dense elastic consistency upon palpation. In the liver SII-III, a subcapsular lesion of a whitish color is determined, with a dense elastic consistency upon palpation, partially extending to the liver SIVa (Figure. 3b). No pathological changes were detected in other parts of the liver. The gallbladder and hepatoduodenal ligament are unchanged.
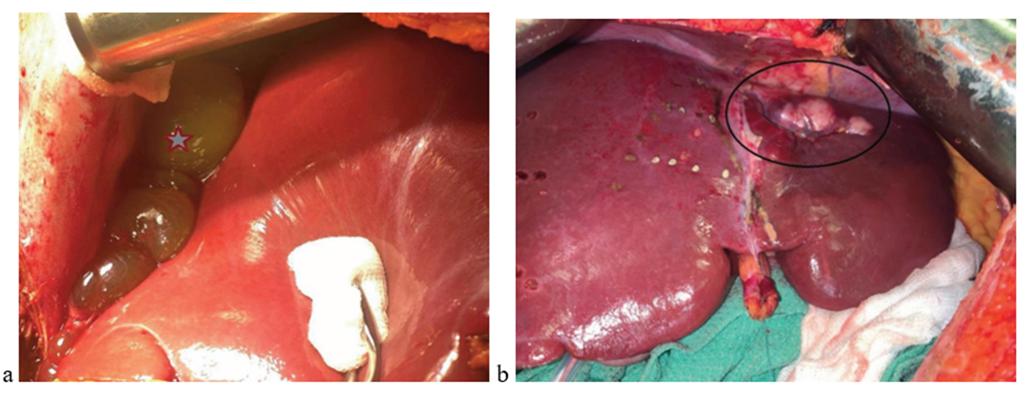
Figure 3. Intraoperative photos: a - a cystic lesion localized along the contour of the liver SVI-VII (indicated by an arrow); b - a solid lesion in the liver SII-III-IVa (indicated by an oval)
Intraoperative ultrasound was performed: in the liver SVI-VII, the lesion with a heterogeneous echostructure (a more echo-dense central part, a less echo-dense periphery with echo-dense structures like septas) with uneven contours without involvement of vessels and bile ducts, measuring 8×4×7 cm (Figure. 4a) is determined. Blood flow is localized in the capsule of the lesion (Figure. 4b) with arterial low-resistance blood flow. In the liver SII-III, there is the lesion with partial extension to the liver SIVa of a heterogeneous echostructure (hypo/isoechoic with echo-dense structures like septas) with uneven contours without involvement of vessels and bile ducts, measuring 6×3×6 cm (Figure. 4c). The above-described blood flow is localized in the capsule and septa of the lesion (Figure. 4d). Two localized hypoechoic foci are also identified along the contour of the main one (Figure. 4d).
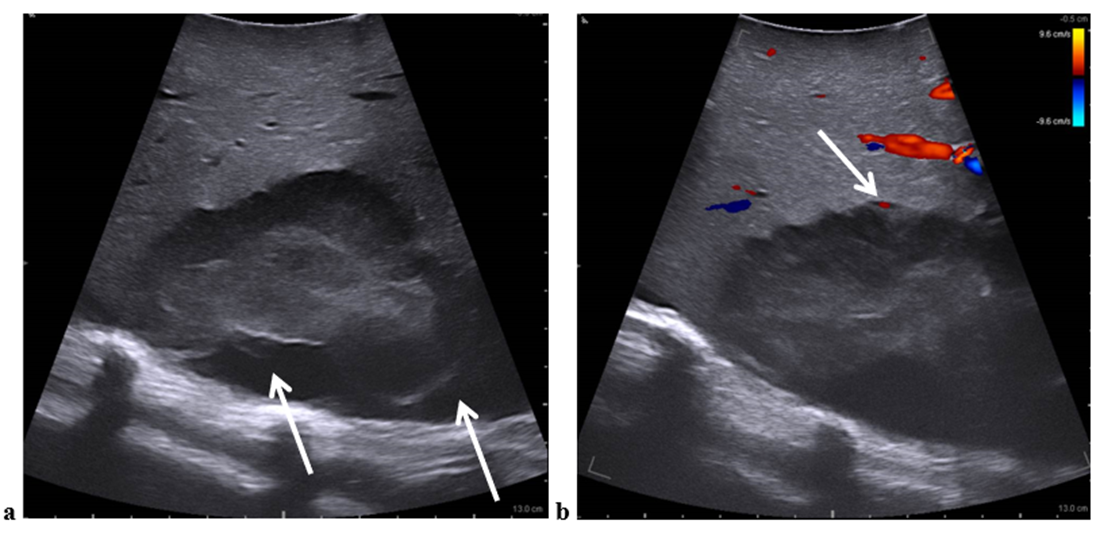
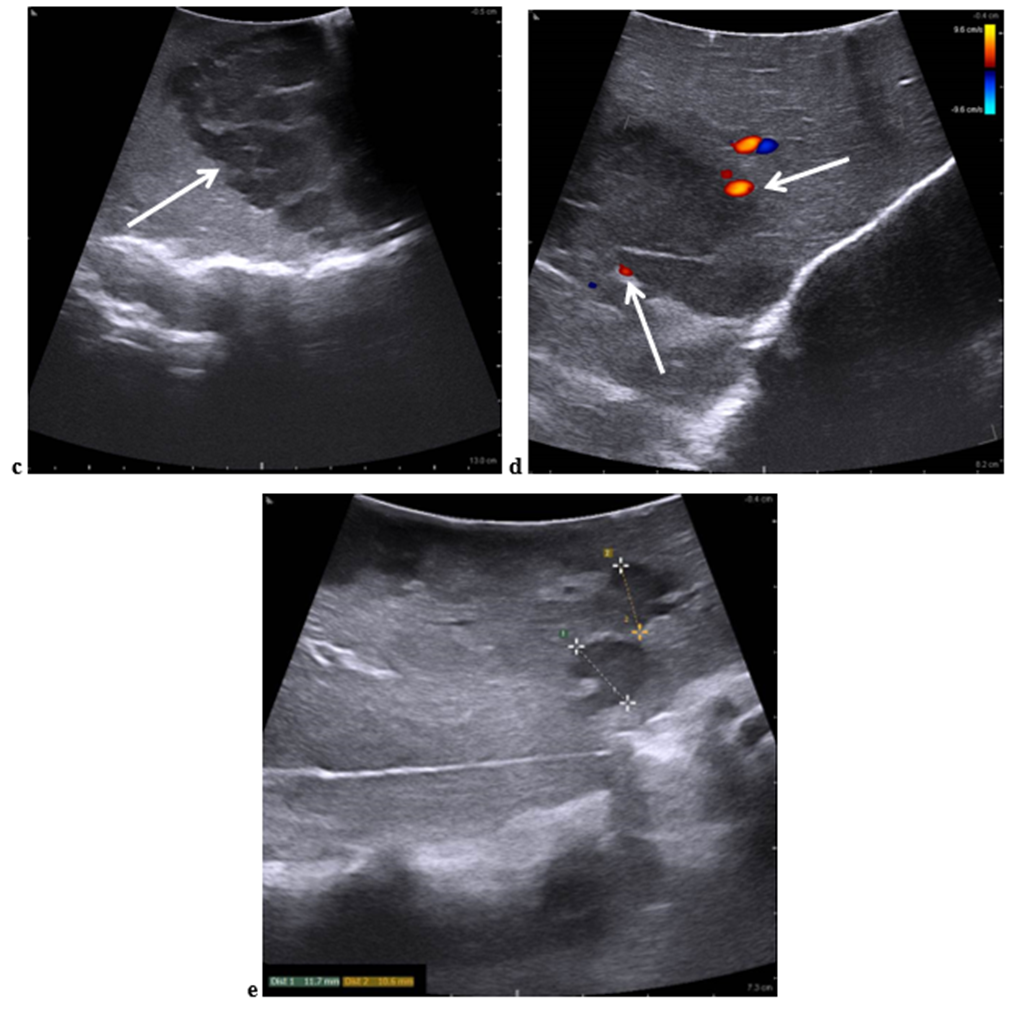
Figure 4: Intraoperative ultrasound images: a - SVI-VII liver lesion with heterogeneous echostructure in B-mode with uneven contours and anechoic extrahepatic liquid lesion spread along the contour of the above-described liver lesion (indicated by the arrows); b - blood flow is localized in the capsule of SVI-VII liver lesion in Color Doppler Imaging (arrow); c - SII-III liver lesion with partial spread to SIVa liver of heterogeneous echostructure in B-mode with uneven contours (arrow); d - blood flow is localized in the capsule and septa of SII-III liver lesion in Color Doppler Imaging (indicated by the arrows); d - two localized hypoechoic foci along the contour of the main (indicated by marks)
The fluid lesion localized along the liver SVI-VII contour was punctured, and 300 ml of serous fluid was obtained. A solid lesion was clearly defined on the liver surface (Figure. 5).
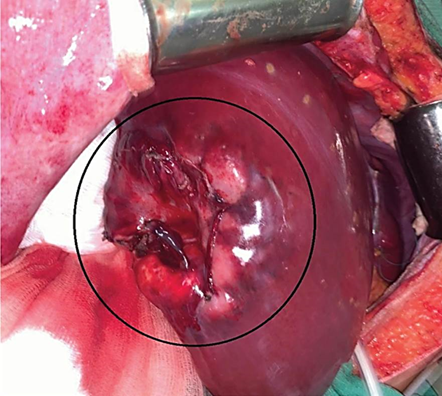
Figure 5: Solid lesion in the liver SVI-VII after puncture of the liquid lesion and its dissection (indicated by a circle)
Liver resection with tumor was performed with preservation of the middle and left hepatic veins. Pringle maneuver was not performed.
Histology (Figure. 6): diffuse large B-cell primary non-Hodgkin's lymphoma of the liver (Figure. 7).
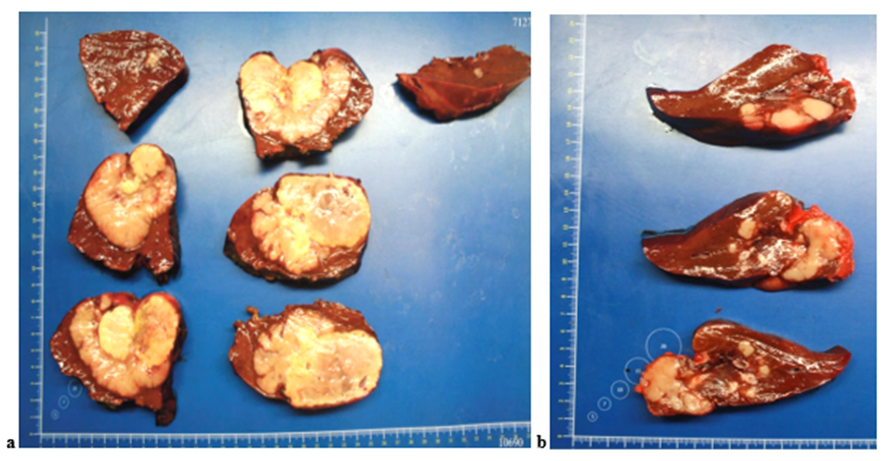
Figure 6: Removed liver segments with tumor nodules: a – the liver SVI-VII; b - the liver SII-III
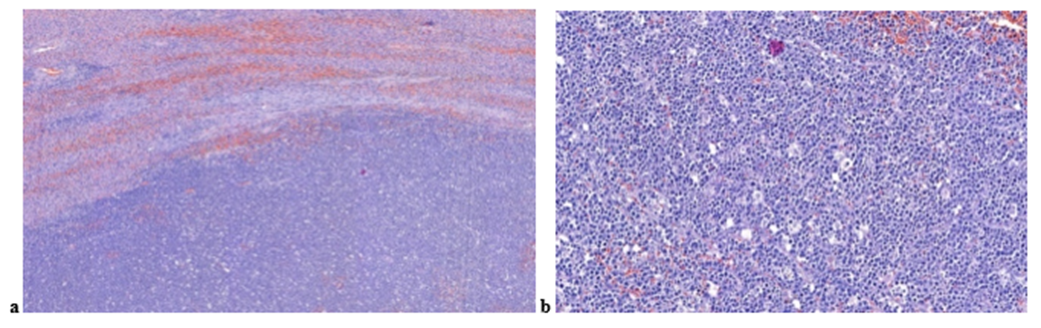
Figure 7: Microscopic preparations, hematoxylin and eosin staining: a - structure of liver lymphoma, x50; b - proliferation of lymphoid cells with signs of atypia, polymorphism, x200
The postoperative period was uneventful. The woman was discharged on the 8th day after surgery in a satisfactory condition.
Subsequently, the woman contacted the National Medical Research Center of Hematology, where she was consulted by a hematologist, an additional histologу and PET-CT were performed. The diagnosis was confirmed: diffuse large B-cell primary non-Hodgkin's liver lymphoma, IVA according to Cotswolds-modified Ann Arbor. The patient receives adjuvant chemotherapy.
Due to the rare occurrence of PHL, the literature most often presents individual clinical cases, sometimes combined with a literature review. Generalizations about any significant number of original cases are extremely rare [16, 17].
PHL most often develops in men (ratio from 2:1 to 3:1). PHL is detected at any age, but it is usually diagnosed in the fifth or sixth decade of life (the average age of patients is 50 years) [15, 18, 19].
The clinical picture varies from asymptomatic to the onset of fulminant liver failure with rapid progression to coma and death. The clinical picture is dominated by symptoms of rapidly progressing liver disease with pronounced signs of intoxication: fever, night sweats, weight loss, jaundice, rapid increase in liver size with signs of liver failure. Increasing severity of liver dysfunction with the addition of portal hypertension may be accompanied by spleen enlargement. Peripheral lymph node involvement is usually absent even in long-standing disease. Hepatomegaly is the most common finding on physical examination, present in 75–100%; jaundice is found in less than 5% of patients [17, 20–23]. Liver involvement may present as solitary nodules, which occur in approximately 55–60%, followed by multiple tumor nodules (in approximately 35–40%) [24]. Diffuse liver infiltration or periportal infiltration is extremely rare, showing only hepatomegaly in the absence of any specific tumor masses in the liver [25, 26]; this subtype is associated with a poor prognosis, as it is more often associated with severe hepatomegaly and liver failure [27]. A combination of infiltration and nodular patterns has also been described [28].
Laboratory examination reveals elevated bilirubin, liver enzymes, LDH, and sometimes hypercalcemia. A case of Bence Jones protein secretion in a patient with PHL has been described [7, 15, 29]. AFP and CEA concentrations in PHL remain within normal values, unlike those in hepatocellular carcinoma, so PHL should be suspected in patients with focal liver lesions, signs of liver failure, and normal AFP and CEA values [8].
Imaging plays an important role in the diagnosis, staging, and monitoring of liver lymphoma cases, since it is used not only to assess the course of the disease but also to guide appropriate procedures (e.g., ultrasound-guided biopsy [30]). The treatment and prognosis of lymphoma differ significantly from other neoplasms. Therefore, familiarization with the imaging features of liver lymphoma is important for its early diagnosis and appropriate treatment.
In PHL, according to ultrasound, hepatomegaly is noted in all cases and only in 46% of cases hypoechoic focal changes are detected in the liver.
There are three variants of the ultrasound picture of the liver and spleen in PHL: hepatosplenomegaly with focal lesions inside the organs; hepatosplenomegaly without focal lesions, the echogenicity of the spleen and liver is reduced (diffuse lesion); and also in the long-term course of PHL - hepatosplenomegaly without focal lesions, the echostructure of the organs is enhanced, heterogeneous (diffuse lesion + fibrosis) and focal lesions in the spleen and liver while maintaining their normal sizes [31-33]. It should be noted that since ultrasound is considered a non-specific screening method of research, then in the literature, especially in recent years, practically no attention is paid to specific ultrasound signs of PHL. In the above clinical case, intraoperative ultrasound was performed with the sensor installed directly on the liver parenchyma, so a high-quality ultrasound image was obtained. The following ultrasound picture can be stated. In the liver, the lesions of heterogeneous echostructure are determined: from hypoechoic homogeneous nodules with clear contours to the lesions of heterogeneous echostructure (hypo/isoechoic lesion with echodense structures like septas or the lesion with a more echodense central part and a less echodense periphery with echodense structures like septas). In the capsule and septa of the lesions, vascular signals with arterial low-resistance blood flow are detected. The presence of fluid lesions (anechoic) filled with lymph is possible. Also, ultrasound patterns of PHL with the echocontrast agent (CEUS) are described in the literature. In CEUS, the PHLs are heterogeneously hypercontrasting in the arterial phase and hypocontrasting in the portal and delayed phases of the study [34].
As seen on unenhanced MDCT, PHL lesions are typically hypodense with soft tissue attenuation. Necrosis or hemorrhage may also be seen. Calcification is quite rare before treatment. After the intravenous contrasting, two different types of enhancement patterns may occur. First, in most cases there is minimal or no enhancement at all phases, and when enhancement is present it is usually less than that of the surrounding liver parenchyma. Second, less commonly, there is marginal enhancement of the lesion with a central non-enhancing zone, giving the lesion a target appearance [28, 35, 36]. On MRI, lesions are typically hypointense or isointense on T1-weighted images and hyperintense on T2-weighted images, with minimal or no enhancement on dynamic post-gadolinium imaging. Central retention of hepatic-specific contrast agent in the delayed (hepatobiliary) phase has been reported. On diffusion-weighted imaging (DWI), PHL lesions typically exhibit markedly restricted diffusion, which is explained by their highly cellular histology [28, 35, 37, 38].
It should be noted that the imaging appearance of PHL is difficult to differentiate from primary and metastatic liver cancer and cholangiocarcinoma, especially when patients have cirrhosis. It is difficult to differentiate PHL from primary liver cancer because primary liver cancer often shows changes in liver size, liver lobe proportions and contour, as well as the presence of cirrhosis and significantly elevated alpha-fetoprotein levels. Also, primary liver cancer is characterized by the phenomenon of “rapid enhancement and rapid washout” in the arterial phase of the examination, with clear contrast between the lesion and the surrounding liver parenchyma and a clear peripheral low-density halo sign. However, when PHL involves the portal vein and its surroundings, a similar halo sign around the portal vein may appear, making differentiation difficult. In addition, in some patients, enhancement may occur at the periphery of the lesion, while the central area does not enhance, which resembles cholangiocarcinoma. Foci of cholangiocarcinoma may be present in the bile ducts and show enhanced scans with a peaked linear density similar to water. Delayed phase enhancement is a typical feature of cholangiocarcinoma. Elevated levels of CA 19-9 and the appearance of symptoms such as jaundice further help in the differential diagnosis. Multiple liver abscesses (bacterial, cholangiogenic, parasitic) cannot be completely excluded due to pronounced signs of a systemic inflammatory response - fever, leukocytosis with a band shift, increased C-reactive protein levels, as well as blurring and hypoechogenicity of foci in liver tissue according to ultrasound data [35, 39-42].
Thus, although there are no specific MDCT and MRI imaging features for liver lymphoma and biopsy is almost always necessary, familiarity with the most common imaging features can facilitate early suspicion and appropriate treatment, which may improve the prognosis of the disease. Radiologists and clinicians should work closely together to ensure a comprehensive and multidisciplinary approach to the evaluation and management of patients with liver abnormalities.
Based on clinical and radiology features, it is impossible to reliably differentiate PHL from other liver diseases (squamous cell carcinoma metastases, adenocarcinoma, primary liver cancer, embryonal sarcoma, granulomatous cholangitis, inflammatory pseudotumor, granulomatous hepatitis, etc.). The diagnosis of PHL requires biopsy of the liver lesion in the absence of extrahepatic disease [43]. Immunohistochemical studies are necessary to determine the correct subtype. If the focal lesion is not visualized for percutaneous biopsy, a transjugular approach may be a reasonable option [44]. In this regard, the diagnosis of PHL is often established only after surgical removal of the tumor [15, 45, 46]. Due to the rare development of PHL and the lack of prospective studies, there is no general algorithm for choosing a therapy. Surgery usually fails to achieve stable remission; without subsequent specific chemotherapy, disease progression is observed early after the intervention, while tumor removal does not improve treatment outcomes [47]. The standard chemotherapy for this group of patients is the [R]-CHOP regimen, which contains Rituximab, which increases the tumor response rate and overall survival of patients with diffuse large B-cell lymphoma without significantly increasing toxicity [48]. The median survival of patients with PHL is on average 163 months, and the 5-year survival is 77%. The absence of fever, weight loss, and anemia are independent factors of poor prognosis in patients with PHL [15]. It should be noted that fever theoretically increases survival in patients with PHL by stimulating the production of long-lasting tumor-specific immune responses that recognize and destroy tumor cells [49, 50].
In the above clinical case, PHL was detected during pregnancy. Before pregnancy, examination of the abdominal organs didn’t reveal a focal lesion in the liver. The lesdion was detected upon admission to the hospital the day before the timely natural birth at the 39th week of gestation. Unfortunately, during pregnancy, the woman didn’t undergo abdominal ultrasound. Biochemical blood parameters in control tests during pregnancy were within normal values. There were complaints of periodic pain in the right hypochondrium, however, the patient didn’t undergo the recommended abdominal ultrasound. Thus, it is not possible to judge pregnancy as a factor contributing to or provoking the development of PHL. It is only possible to state the fact of the presence of multiple PHL in the patient during gestation. Literature data on the relationship between PHL and pregnancy are extremely scarce, there is a single case where the fact of such a possibility is noted [51]. The presented data are only descriptive in nature without an analysis of the causes of occurrence. The tumor was detected in the third trimester of pregnancy; examination and treatment were carried out after delivery.
PHL is an extremely rare disease with non-specific symptoms and variable laboratory and imaging findings. It should be part of the differential diagnosis in a patient with nodular liver lesions, especially in the presence of normal tumor markers and/or elevated LDH levels. Histology is mandatory for definitive diagnosis. It is important to recognize PHL because it is a chemotherapy-sensitive disease and its timely diagnosis allows for early treatment and improved overall survival.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
