
Review Article | DOI: https://doi.org/10.31579/2690-8794/035
*Corresponding Author: Odoko J.O. Department of Public and Community Health, Novena University Ogume, Nigeria.
Citation: Odoko J.O., Nwose E.U., Nwajei S.D., Igumbor E.O., Agege A.A. and Moyegbone J.E., (2020) Primary Healthcare on Utilization of Insecticide Treated Nets among Pregnant Mothers and Careers of Children in South –South Nigeria J, Clinical Medical Reviews and Reports. 2(6); DOI: 10.31579/2690-8794/035
Copyright: © 2020, Joseph O Odoko, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 12 August 2020 | Accepted: 17 August 2020 | Published: 09 September 2020
Keywords: healthcare providers, insecticide treated nets, pregnant mothers, primary healthcare, care-givers, children under five years
One of the strategies of Primary Health Care (PHC) is the use of insecticide treated nets (ITNs) against malaria among pregnant mothers and care givers of children under five years. The agency for PHC in Nigeria is the National Primary Health Care Development Agency (NPHCDA). The objective of this narrative review is to identify the role of PHC providers in promoting the use of ITNs among pregnant mothers and care givers of children under five years. Method was by review of 30 published literatures on PHC; as it relates to use of ITNs. Findings indicate that most pregnant mothers and care-givers of children under five years in Nigeria are aware that the best option to prevent malaria infection is by use of ITNs. Healthcare providers participate in mass distribution of ITNs. There is increase nets ownership in households. Supervisory guidance influences use of ITNs. However, there is evidence of slow uptake of ITNs due to resistance to behavioural change. Also, the knowledge of pregnant women concerning ITNs use was good, but the attitudes and practices were poor. The implication is that health promotion need to be enhanced among both PHC workers and community leaders on use of ITNs. Primary healthcare workers may need to be motivated to do their job in terms of promoting the use of ITNs among pregnant mothers and carers of children under five years.
Primary health care was defined in the Declaration of Alma-Ata at the International Conference on Primary Health Care, Alma-Ata, USSR, in 1978. Delegates to the conference expressed "the need for urgent action by all governments, all health and development workers, and the world community to protect and promote the health of all the people of the world [1]. Most of the PHC strategies are performed at the level of the Health Centers (HC), which are the heart of primary care at the first level of care in the public network. Since HC are where most of the health promotion and disease prevention activities occur, they receive a large portion of the public budget allocated to population health at the municipal level and play an important role in offering services to a large proportion of the population throughout their lifecycle [2]. In 1985, Nigerian government introduces PHC as a national health policy and emphasizes the importance of preventive medicine. In 1992, the creation of the NPHCDA took place for the control of the implementation of PHC [1].
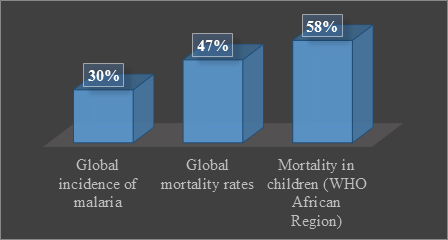
As shown in Fig 1, between 2001 and 2013, a substantial expansion of malaria interventions contributed to a 47% decline in malaria mortality rates globally, averting an estimated 4.3million deaths. In the WHO
African Region, the malaria mortality rate in childrenunder 5 years of age was reduced by 58%. During the same period, the global incidence of malaria was reduced by 30%. Target 6.C of Millennium DevelopmentGoal 6, namely “Have halted by 2015 and begun to reverse the incidence of malaria and other major diseases”, has already been reached, and 55 of the 106 countries that had malaria transmission in 2000 are on track to achieve the goal of reducing malaria incidence by 75% by 2015, as set by the Health Assembly in 2005 in resolution WHA58.2 on malaria control. Despite this progress, the disease remains endemic in all six WHO regions and the burden is heaviest in the African Region, where an estimated 90% of all malaria deaths occur. Two countries – the Democratic Republic of the Congo and Nigeria – account for about 40% of estimated mortality due to malaria worldwide. Around the world, millions of people remain without access to malaria prevention and treatment, and most cases and deaths go unregistered and unreported. Given the projected growth in the size of the world’s population by 2030, more people will be living in countries where malaria is a risk, putting further strains on health systems and national malaria program budgets [3].
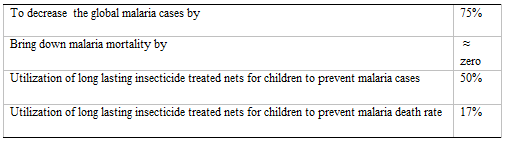
The main aim of WHO’s Roll Back Malaria (RBM) Partnership in 2015 is to decrease the global malaria cases by 75% and bring down malaria mortality to near zero through universal coverage by effective prevention and treatment interventions (Table 1). The reliable tool for malaria intervention recommended by WHO for children under five years is on the utilization of Long-Lasting Insecticide Treated Nets (LLITNs) to prevent up to 50% of malaria cases and 17% of malaria death rate. Universal coverage with ITNs is defined as use by > 80% of individuals in populations at risk [4].
The 2006 declaration in Abuja emphasize on the importance of investing in PHC [5]. Each year on the 25th April Africa and the rest of the world commemorate Africa Malaria Day as was agreed upon at the African Summit on RBM held in Abuja, Nigeria on 25th April 2000. The summit also called upon the United Nations to declare the period 2001-2010 a decade for malaria. One of the expectations of the 6th Africa Malaria Day in 2006 was attributed to the slogan "Universal Access to Effective Malaria Treatment is a Human Right’’[6].
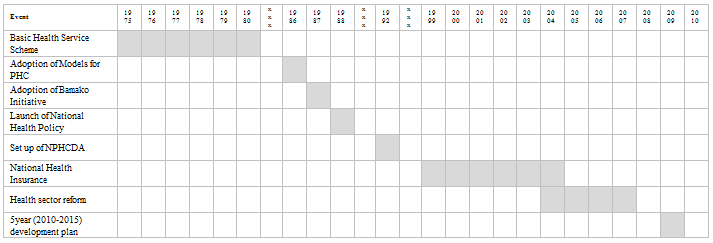
Over 6.2 million malaria deaths have been averted between 2000 and 2015, primarily of children under five years of age in sub-Saharan Africa. The global malaria incidence rate has fallen by an estimated 37 per cent and the mortality rate by 58% (Figure 1). More than 900 million ITNs were delivered to malaria-endemic countries in sub-Saharan Africa between 2004 and 2014 [7]. Despite massive anti-malaria campaigns across the subcontinent, ITNs among pregnant women remain low in large parts of sub-Saharan Africa. The slow uptake of malaria prevention products appears to reflect lack of knowledge and resistance to behavioural change, as well as poor access to resources, and limited support of programmes by local communities and authorities [8]. For an improvement on the health of individuals in the communities four set of reforms on PHC were made on universally (coverage reforms, service delivery reforms, leadership reforms , public policy reforms) for various implementation as a result of demand from member states, health professionals and policy makers [9]. Figure 2 shows a pictorial of timelines in the reforms on Primary Healthcare. For instance, 2009 saw the development of a 5-year National Strategic Health Development Plan (2010–2015); which occurred after implementation of the health sector reform program that kicked-off in 2004 [10].
Given these milestones, this study is set to evaluate expectations and capabilities of stakeholders in PHC on effective utilization of ITNs among pregnant mothers and children under five years in South–South Nigeria. For the purpose of this review series, which this narrative is part of, the stakeholders are divided into two categories. First is the primary healthcare providers (PHP) – including ministry of health officials in charge of primary health care, Local government line managers and PHC workers in the Local Government Areas, Non- Governmental Organizations, (NGOs) State and Local Government and Primary Health Care Boards and Authorities. The second comprises community health beneficiaries including pregnant women, care givers of under five children.
Nigeria was a signatory to the idea of implementing PHC globally vis-à-vis the strategy of community mobilization, service integration and selection of primary health care programmes. Health workers at the primary health care level renders services that are specifically related to the component of primary health care, which includes education concerning prevailing health problems and the methods of preventing and control as well as health promotion amongst others. The policy on PHC accommodates various disciplines of health workers including doctors, utilizing PHC facilities for the needs of the community and families members. This implies a capacity as well as expectation of providing two or more PHC services on the same platform by the same multidisciplinary team and often simultaneously. Unfortunately, the implementation of PHC in Nigeria has been meted with a number of problems relating to health manpower. These problems range from inadequacy of personnel, inequitable distribution of available personnel, inter-cadre conflicts, poor job satisfaction, and paucity of accurate data on the available staff; albeit worsened by lack of planning. In some instances where recruitment of skilled manpower is achieved there have been reported failures in the interpretation of their job descriptions [11].
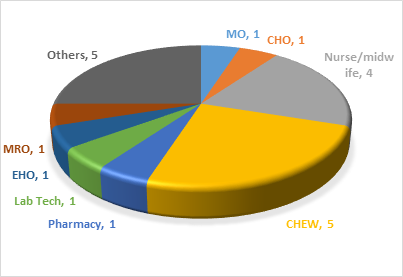
The capacity of health workers expected to deliver primary health care services in terms of control of malaria among pregnant women in PHC setting are Medical Officers (MO), Community Health Officers (CHO), Nurse Midwives, Community Health Extension Workers (CHEW), Environmental Health Officers (EHO), Pharmacy Technicians, Medical Laboratory Technicians (MLT) and Medical Records Officers (MRO). Others include Social Workers, Health Assistants, Security personnel, and General maintenance staff [12]; and there is indication of minimum standard requirement of the different human resources for PHC setting (Figure 3).
Given the recommended PHC services include health education, prevention and promotion on prevailing health issues; management of malaria and distribution of ITNs to pregnant mothers and children under is an expectation. However, there is inequitable distribution of community health work force at the PHC levels. It is hard for any PHC facility to boast of having the expected or suggested minimum staff requirement, except when NGOs visit with their volunteers. Most of the doctors and nurses prefer to work in general or tertiary hospitals. Otherwise, they go into private practice instead of running a PHC. This has caused inequity in access to quality health services [10]. For instance, study in Rivers State indicate that major sources of bed nets is partly from health facilities during antenatal care attendance by pregnant mothers and those distributed free of charge during house-to-house immunization campaigns for children [13]; not necessarily from PHC facilities.
The National Malaria Strategic Plan 2014-2020 is based on providing at least 80% of targeted population with appropriate preventive measures by 2020 through the community, primary, secondary, and tertiary levels. The strategy defines the roles of each health care cadre/level relative to malaria control and case management across all health care services including public, private, and traditional health providers [14]. ITNs mass distribution through Antenatal care and Expanded Program on immunization, has increased net ownership, universal access and net used with children under five. A second facility-based distributed ITN, through EPI beyond the one given at ANC has helped to increase the number at homes with universal access and improving ITNs used by children under five [15]. Health education has been evaluated to show that it increases awareness and improve attitude among breastfeeding mothers, caregivers of children under five years and health workers on utilization of insecticide treated nets in the community [16].
In Kenya, the main channel for ITN distribution is through the government health facilities, particularly to pregnant women who attend antenatal clinics and infants who are seen in the immunization clinics [17]. Also, Togo applied integrated healthcare service to distribute ITNs to children under five years during immunization programmes. This combination of ITNs with vaccinations in health centers by health care providers has increase ownership of ITNs [18]. WHO recommendation on integrating use of ITNs with other program has been successful for universal coverage in terms of distributing LLINs at TT vaccination sites [19]. Therefore, the capacity to improve distribution or uptake of ITNs at PHC facilities exists. Perhaps, the question is whether the community members have behavioural change wheel; and this leads to the next section.
Knowledge and positive perception as well as ability and willingness to practice have been identified as enhancers in effective utilization of ITNs [20]. In this regard, the specific questions on behavioural change wheel to ‘take up and effectively use the ITNs’ are whether the women and caregivers (1) want to do it, (2) know what to do, (3) know how to do it, (4) have change to do it, and (5) have necessary guidance/supervision
Studies have shown that pregnant mothers easily accept sleeping under insecticide treated nets more than non-pregnant mothers. Also, mothers that sleeps with their little children on bed utilized use of ITNs more often than those that sleep on mat [21]. Pregnant mothers and care givers of children under five years have easy access of ITNs through primary health care facilities and private clinics in the communities [22]. Study in Tanzania and Nigeria revealed that majority of mothers with children under five years are aware that the best option to prevent malaria infection is by use of insecticide treated nets. But in the same study, challenges in use of ITNs were associated to negative perception on effect of chemicals in the ITNs, discomfort due to heat with ITNs and at risk of having cancer in pregnancy due to ITNs. This agreed with other related findings for children and pregnant mothers not using the nets despite free possession of ITNs [23]. These reports show there is a desire to own ITNs as well as knowledge and opportunity to effectively use it.
Disparity in knowledge on prevention of malaria with use of ITNs in Nigeria rural setting has been identify to be due to pregnant women and care givers of children under five years who frequent health care facilities and are health educated on the important of ITNs on like other respondents that are not exposed to both massive scaling distribution in the country and having a non-pregnancy status. This signified the need to intensify efforts on malaria awareness campaigns if eradication of malaria from the country is to be actualized [24]. Factors that influences the delivery of ITNs at a wider scope is identified to be involvement of stakeholders during planning, implementation and cooperation across ministries, departments and sectors (e.g. health and retail); which include supervisory guidance, motivation and support in term of subsidized costs of ITNs, sufficient supplies of ITNs and sustained distribution of ITNs to users [25]. Study has shown that malaria control program could be designed to accommodate large community base distributors which include State and Local Government malaria control program managers in various primary health care systems whose role is to supervise, monitor and evaluate community base distributors with continue in training on distribution of ITNs. This approach will help to sustain the availability of ITNs to a large extend to the rural areas [26]. These highlight the limitations in ability and willingness i.e. capacity and motivation components of behavioural change wheel to effectively use the ITNs.
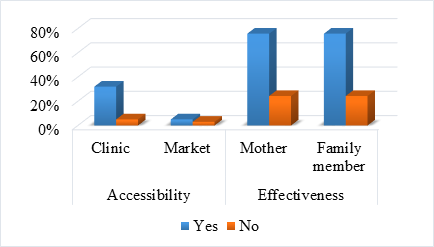
A descriptive community based study of mothers on use of ITNs in a rural area in North Sudan shown that in spite of good knowledge about ITNs mothers still have negative attitude to always sleep under it. Also, mothers with formal education have high rate knowledge about ITNs than those with informal education [27]. In a similar research, it was concluded that ownership of ITN/LLIN by pregnant women per household does not necessarily translate to usage. It recommended extensive health education how and why to use ITNs in order to improve ITN usage among pregnant women in Nigeria [28]. Therefore malaria education will help in behavioral change towards an increase utilization of insecticide treated nets among mothers. Nevertheless, some challenges of wanting to use ITNs when pregnant or having a child under five years has been identified during a previous preliminary study in the communities. Besides issues of accessibility and queried effectiveness (Figure 4); excessive heat and nature of accommodation were among the barriers cited [29]. Pertinently, this is evidence of slow uptake. It has been reported from priori study in the same Nigeria that 26% of a control group were not ready to use ITNs even if given free [16]. Further, a recent report supporting this view shows about 50% Nigerian households own ITNs, but less than 20% slept under it ‘the previous night’ of survey [30].
PHC is the lowest level of care in the health care system. Most of the activities are carried out in the PHC, which include health promotion and disease prevention. Among the activities are provision of ITNs for pregnant mothers and children under five years to prevent malaria. The NPHCDA is responsible for the control of PHC in Nigeria. Intervention of malaria has been a global responsibility to World Health Organization (WHO) where its role has contributed to 47% decline in malaria mortality globally thereby preventing up to 4.3 million deaths. In Africa the mortality rate in children under five years due to malaria effect was reduced by 58% and at the same period the global malaria cases has reduced by 30%. A reasonable numbers of countries that is 55 of the 106 countries that had malaria transmission are close to reducing the incidence malaria by 75% by 2015. The progress in control of malaria transmission is yet to create an impact in Africa regions where 90% of all malaria mortality exist as endemic disease [3]. The RBM Partnership has help to bring down malaria mortality to near zero through universal coverage, using a recommended tool such as utilization of LLINs by vulnerable groups [4]. The implementation of the African submit slogan of 2000 through Universal access to effective malaria treatment is a human right, have prevented over 6.2 million malaria deaths among under five years children in Sub-Saharan Africa [6, 7]. Nigeria has use PHC workers to render distribution of ITNs to pregnant mothers and caregivers of under five years through maternal and child healthcare program. Success of integrating PHC programs with free and subsidized ITNs to the population at risk of malaria has increase ownership and usage of ITNs among pregnant mothers and caregivers under five years resulting to decrease in incidence of malaria cases and mortality.
However, the challenges on achieving universal coverage for zero malaria is identified as poor attitude and low utilization of ITNs due to misconception, discomfort, poor building quality, through various research. The barrier to effective utilization of ITNs can be removed by motivating PHC workers, and improving on integrated healthcare services. Other indispensable program is health promotion in terms of education on benefits and ways of using ITNs, regular supply of free or subsidized ITNs to individual’s homes and improvement on quality on housing to overheat during dry seasons.
PHC has played a key role in improving majority of the population at the rural areas through the availability of primary health facilities being organized mostly by the Local government authorities under the supervision of the Federal and State Governments. One of the interventions methods utilized in health promotion for the pregnant mothers and under five children at the PHC level is the creation of awareness on use of ITNs. The challenges identified to effective utilization of ITNS are basically behavioural change wheel vis-à-vis capacity, motivation and opportunity for both benefactor (primary healthcare providers and end-users. This report draws attention on various stakeholders to acknowledge available opportunities of health promotion in PHC for the benefits of pregnant mothers and under five children on effective use of ITNs to reduce incidence of malaria cases and mortality.
This work is a prelude to public health dissertation into ITNs among pregnant mothers and care givers of children under five years in South- South Nigeria, a case study of Delta, Bayelsa and Rivers State respectively.
no funding sources
there are no conflicts of interest
not required
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
