
Review Article | DOI: https://doi.org/10.31579/2690-8794/039
1* Department of Public and community Health, Novena University Ogume, Nigeria.
2 School of Community Health, Charles Sturt University, New South Wales, Australia.
*Corresponding Author: Edmond Anowa. Department of Public and community Health, Novena University Ogume, Nigeria.
Citation: Edmond I Anowa, Ezekiel U Nwose, Samuel D Nwajei, Chime H., O. Egwenu S. E. and Eunice O Igumbor (2020) Primary Healthcare and diabetes management in the rural communities; J Clinical Medical Reviews and Reports. 2(7); DOI: 10.31579/2690-8794/039
Copyright: © 2020, Edmond Anowa, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 August 2020 | Accepted: 24 August 2020 | Published: 09 September 2020
Keywords: behavioural change wheel; central hub role; diabetes care; primary healthcare; delta state nigeria
Primary health care (PHC) was conceptualized to play a ‘central hub’ role in health systems. Diabetes care services are presently unavailable in PHC facilities, except the screening programs that are carried out by non-governmental organizations. This implies there is issue of behavioural change wheel (BCW) of the stakeholders including the quartet of ministry of health, hospital management board, healthcare professionals (HCP) and diabetes patients. This narrative review investigates perception of stakeholders towards scaling-up of a diabetes context of PHC agenda in Delta State Nigeria. The study utilized data from ongoing studies including opportunistic and purposive sampling designs. Data from published literatures on Nigeria were also reviewed. The various stakeholders’ perceptions is that motivation is poor across board. The ministry of health as well as the hospitals management board, but not patients, have the capacity. Suggested ways of improving BCW in the state include increased allocation for the ministry of health, and retraining healthcare professionals. Others improvement measures including tackling socio-cultural beliefs, and taboos are suggested. Scaling-up and sustaining diabetes care program at the PHC level in Delta State is agreed to be the responsibility of all stakeholders. There is need to enhance capacity/knowledge among community members living with diabetes, and opportunity/practice among the HCPs, but most importantly attitude/motivation of all stakeholders.
It is known that primary health care (PHC) was conceptualized to bring equitable quality health services to every nook and cranny of communities. Citizens are aware of PHC, but they mostly access the services at secondary healthcare levels. Employees at the PHC are aware of their responsibilities as community healthcare workers, but some are probably unware of non-invasive risk assessments they could do or subconscious of their services being rarely accessed. The management including supervisors of PHCs know the limited services being offered at the sites, but the willingness to improve is a thing of ongoing discussion [1].
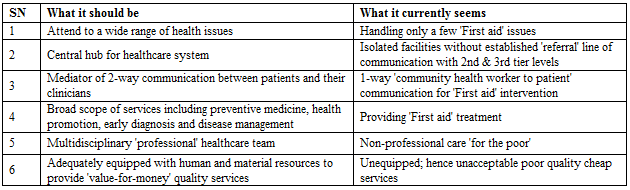
Many rural dwellers are probably unaware of scope of services available to the PHCs. The employees at the sites are unaware that community members do not know the scope of services available or what other capacities they have. The management including supervisors of PHCs do not know what communication gaps exist with the target beneficiaries of their facilities. The prevailing factor has been articulated as a gap between what PHC should be and what it currently seems (Table 1).
With regards to contextualizing primary healthcare of diabetes, the PHC can be described as illustrated (Figure 1). However, a confounding gap in knowledge, attitude and practice is that when community members do not access the PHC, employees have virtually no service to render. The implication is lack of need to demand for resources by staff from management. This leads too little monetary and personnel provision being allocated to the site. The effect is controversy whereby the people complain of inadequate equipment of the PHC.

Therefore, to reactivate PHCs in rural communities of Delta state for improved diabetes services; there need to advocation of behavioral change wheel among both benefactors are beneficiaries of the PHC facilities, especially for community members to access available services. This will necessarily require a ‘community needs assessment’, which is evaluation of stakeholders.
This narrative review utilized pieces of descriptive studies including opportunistic and purposive data [3-5]. The opportunistic study was carried out in the University, when stakeholders are various health professionals who attended take-off workshop of the Bringing Research in Diabetes to Global Environments and Systems (BRIDGES 2) program. The data collection were based on a standard questionnaire that assessed perceptions of ‘capacity, motivation and opportunity’ on Likert scale of ‘poor, fair or good’. Verbal responses of the respondents in the workshop group discussions were documented [4]. Purposive survey involved ‘N = 85’ who attended ‘training the trainers’ workshops at five health facilities from 18/12/2018 – 15/01/2019. Comments of HCP about patients’ behaviour were noted. The collected data were analysed thematically and using Microsoft Excel.
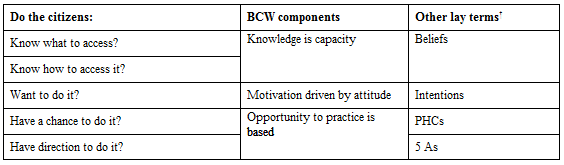
This evaluation of behavioural change wheel that has been ongoing was premised on the fact that beliefs and intentions are integral to running quality health services, especially in reactivation of PHC services [6]. This is with a view to adequately run diabetes clinics – i.e. where the opportunity to practice already exists in the PHC facility (Table 2).
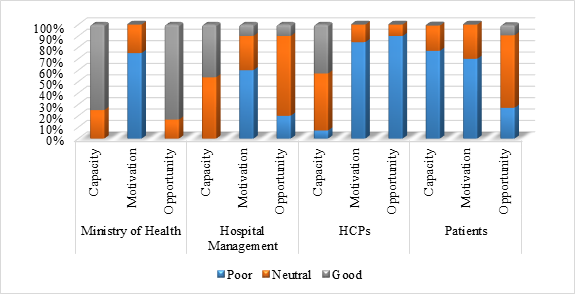
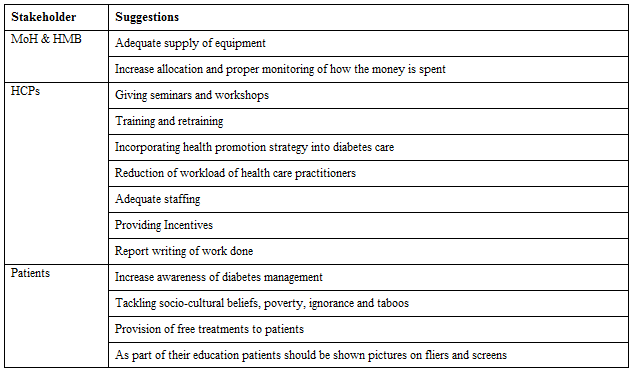
Based on the survey, it was reported that stakeholders’ perceptions on capacity is good (41%), but poor (74%) on motivation and fair (39.5%) on opportunity [3]. A more detailed review show for that capacity is only poor among the patients while the ministry of health and hospital management board have the capacities to deliver. However, lack of motivation cuts across all stakeholders (Figure 2). On the healthcare professional i.e. staff employed to do the job, 85% believe there is poor motivation while a relative higher 90% believe their opportunities to deliver quality services is also poor. Based on qualitative data, ways to improve BCW include adequate funding by the ministry of health, and continuing professional development education for the healthcare professionals amongst others (Table 3).
It was also reported that more than half of civil servants living with diabetes declined to participate in peer-education network albeit out of fear that their public knowledge of their health condition is a threat to job security. Also, more men participated, which was contrary to socio-cultural beliefs (Figure 3). Therefore, tackling socio-cultural beliefs and taboos associated with management of diabetes were suggestions for advocacy [3].
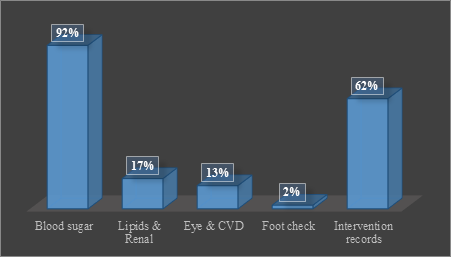
Further from brief literature review, there indication that even in tertiary health facilities, diabetes services are substandard [7]. There is report of very low level of assessment for potential complications and limited interventions in high risk cases (Figure 4). A recent report has also highlighted the need to improve on diabetes care knowledge and practice among PCPs [8].

It is known that healthcare systems determine what health services are available and affordable to those that need them. In particular, the health sector is financed through different sources and the budgetary limitations determine the extent of achieving successful healthcare system. In Nigeria, universal health coverage is a desire of the government, but remains a challenge [9]. The Nigerian health delivery system comprises three tiers including primary healthcare centers (PHC) at rural communities. The primary care level is meant to be the entry point to health care services, and includes the health posts or clinics, as well as health centres with varying scopes of services covering curative, preventive, promotive, and rehabilitative services. It is estimated that more than half of the population are meant to be served by the PHC facilities [10]. For instance, diabetes self-management (DSM) education is now a cornerstone in glycaemic control and preventing cardiovascular disease (CVD) complications [11, 12], but there are still barriers in Nigeria [13, 14]. One of such barriers has recently been reported that “there is capacity to run diabetes screening and service clinic at the primary healthcare levels, but the limitation was incomplete patient information in the medical records” [15].
Concerted efforts have advanced diabetes care to the extent that counselors, nutritionists, physical & health education and psychologists are now part of holistic care system. Suffice to note this underpins the concept of DSM and peer education/support that has been a research interest [16-20]. Further, the capacity, motivation and opportunity to change is synonymous with knowledge, attitude and practice, respectively [21, 22]. It is pertinent to note that belief precedes intention, which leads to planning but depends on habits. Therefore there is need to advocate that reactivation of PHC to takes its appropriate ‘central hub’ role of diabetes management in Delta State is the responsibility of all stakeholders, but especially the government. The opportunities vis-à-vis facilities are available but there is need to enhance advocacy for capacity/knowledge and attitude/motivation of all stakeholders including healthcare professional, health service managers and diabetics in order to advance BCW. For instance, assessment and proper documentation of patients’ weight may be attributable to healthcare personnel’s attitude, but providing the reference chart can enhance motivation. Lack of knowledge of the individuals living with diabetes translates to limited capacity for self-management. Yet, re-training community healthcare workers can enhance informal peer-education process to mitigate lack of knowledge.
This paper critically looked into the subject of PHC with reference to its origin and meaning. As this subject was related to diabetes, the paper illustrated the PHC context of diabetes care. The narrative review utilized ongoing works done in the area of behavioural change wheel of stakeholders to articulate the capacity PHC to play a central hub role in diabetes management. It is plausible to conclude that a negative overall perception of the capacity, motivation and opportunity of the ministry of health, hospital management board, health care professional and diabetes patients to scale-up and sustain diabetes care education program in Delta State. The study recommends increased working synergy among the various stakeholders to scale-up and sustain diabetes education program in Delta State. For the ministry of health and hospital management board there should be increased allocation of resources to rising prevalent non-communicable diseases like diabetes. For the health care professionals, more should be encouraged to specialize as endocrinologist to increase the pool of endocrinologist in the state. Also multidisciplinary approach including team work should be encouraged among health care professionals in sustaining diabetes care at health facilities. For the patients increase awareness of all aspect of the disease should embarked upon regularly while also equipping the patients with skills for self-management of the disease.
This work is a doctoral preliminary review for the extension of an ongoing project. The associated data presented in the results of evaluation have been published in both conference presentations and journal as referenced. Agofure Otovwe, and Josiah Adjene from the department of Public & Community Health in Novena University are instrumental in the work.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
