
Case Report | DOI: https://doi.org/10.31579/2642-973X/019
Medicine, Ad-Din Women’s Medical College Hospital, Dhaka Bangladesh.
*Corresponding Author: Richmond R Gomes, Medicine, Ad-Din Women’s Medical College Hospital, Dhaka Bangladesh.
Citation: Richmond R Gomes. (2022). Primary Anti-Phospholipid Antibody Syndrome presenting as Multiple Cerebral Venous Sinus Thrombosis: An Arduous Manifestation. Brain and Neurological Disorders. 5(2); DOI:10.31579/2642-973X/019
Copyright: © 2022, Richmond R Gomes, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 26 February 2022 | Accepted: 10 June 2022 | Published: 21 June 2022
Keywords: lupus anticoagulants; antiphospholipid antibody syndrome; diplopia; mr venography; anticoagulant
Lupus anticoagulants (LA) are circulating autoantibodies, primarily directed against phospholipids, that prolong the partial thromboplastin time. Antiphospholipid antibody syndrome (APS) is an autoimmune disorder, mainly found in young females, presenting with vascular thrombosis and/obstetric complications. Thrombosis at anatomically significant sites may lead to considerable morbidity and/or mortality. We here present a 22 years old lady with no prior rheumatological history, presented with sudden onset headache, vomiting, diplopia who later diagnosed with multiple cerebral venous sinus thrombosis (CVST) due to with primaryAPS.MR venography was instrumental in diagnosis. Except for mild headache, the other symptoms responded to anticoagulant. Such massive cerebral venous thrombosis is extremely rare in primary APS.
Antiphospholipid syndrome is characterized by clinical features which include arteriovenous thrombosis, recurrent pregnancy loss, thrombocytopenia, and the presence of antiphospholipid antibodies including anticardiolipin antibody (call) and lupus anticoagulant (LA) [1,2]. Antiphospholipid syndrome was first observed in a patient with systemic lupus erythematosus, 2 but has also been observed in patients with other connective tissue disorders, as well as with infections or drug-induced disorders1-secondary APS . Antiphospholipid syndrome in the absence of such underlying conditions has been observed, and is defined as primary APS [3,4].
The most common clinical manifestation of APS is venous thrombosis, especially deep vein thrombosis of the lower extremities and pulmonary embolism, followed by thrombosis of the thoracic, abdominal or pelvic veins [5,6]. In approximately one fourth of patient’s arterial thrombosis may be the initial manifestation. Although cerebral venous thrombosis (CVT) is rare as initial presentation of APS 7, this diagnosis should be considered in a patient with an unusual headache and no known risk factors for thrombosis.
A 22-year-old pleasant Bangladeshi lady, not known to have hypertension, diabetes mellitus or bronchial asthma presented to us with the complaints of double vision, photophobia and worsening left occipital headache radiated to the temporal area for the previous 7 days. The pain was worse on awakening, and waxed and waned. Coughing, sneezing or straining at defecation increased the headache. She also had several episodes of generalized tonic clonic seizures over preceding ten days. She reported several months’ history of recurrent morning dull headache with vomiting. She denied any limb weakness, altered sensorium, fever, visual, and speech or memory disturbances. She also reported short-term use of medications for suspected vascular headache with amitriptyline and propranolol without any improvement but there was no history of oral contraceptive use. She also denied history of trauma to the head, any surgical intervention or any previous thrombosis. There was no joint pain, oral ulcer or skin rash. She had two child and no history of menstrual irregularities, previous abortion or bad obstetric history. Her family history was also non-conclusive of any thrombotic disorder. A physical examination revealed bilateral grade II/IV papilledema eye fundus, with no other neurological focal signs except right sided sixth cranial nerve palsy (Figure 1). The patient was awake and alert, in no acute distress, with normal vital signs. There was no evidence of lower limb deep venous thrombosis. Other physical exams were unremarkable.
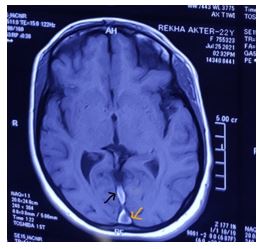
Initial laboratory investigations revealed normal blood counts except thrombocytopenia(104000/µL), TSH as well as kidney and liver function. Electrocardiography revealed sinus tachycardia. Brain Magnetic Resonance Imaging (MRI) revealed cord sign (Figure 2- black arrow), dense vein sign (figure -3, black arrow) and empty delta sign (figure 3 –yellow arrow). Magnetic Resonance Venogram (MRV) suggestive of thrombus in superior sagittal sinus, straight sinus, left transverse sinus and part of left sigmoid sinus (Figure 4).



Tests for other autoimmunity markers (antinuclear antibody, ENA profile-ANCA, c-ANCA) were negative. Laboratory tests performed for the assessment of a hypercoagulable state revealed the following results:, d-dimer 6.74 mg/mL (normal <0>
So, considering our provisional of multiple cerebral venous sinus thrombosis secondary to primary anti phospholipid antibody syndrome was made and treatment with low molecular weight heparin along with oral apixaban was started along with anti-convulsant levetiracetam and resulted in immediate symptomatic improvement. Patient’s hospital stay was uncomplicated, and she was discharged on day 8 on oral anticoagulation with apixaban.
On follow up, after three months, the lupus anticoagulant was still positive. Thus, the antiphospholipid antibody was persistent, supporting our initial provisional diagnosis. The patient remains clinically well on oral anticoagulation with apixaban, without any further episode of thrombosis. The plan of treatment is continuing anticoagulation for 6 months.
Antiphospholipid antibodies are predominantly acquired serum immunoglobulins with affinity for anionic and neutral phospholipid-containing moieties, such as cellular membranes of vascular endothelium. The two most extensively studied a PL are a CL and the LA [3,8]. In the past decade a syndrome—the antiphospholipid syndrome—has been described in which systemic and cerebral venous and arterial occlusions are seen at a relatively young age and with a relatively high risk of recurrent thrombo-occlusive events [9,10,11,12].
Antibodies to phospholipids, first described in association with systemic lupus, are present at low titer in approximately 4% of the general population [13]. Persistent high titers, in particular of IgG anticardiolipin, are clearly associated with thrombosis at multiple sites. In the absence of connective tissue disease, the antiphospholipid syndrome has been associated with a number of neurological presentations including chorea, seizure disorder, psychiatric disturbance, and transverse myelitis [2,11]. The case presented here illustrate the association of antiphospholipid antibodies with cerebral venous sinus thrombosis.
CVST is a rare disorder carrying a relatively high mortality (10% to 15%) [14,15]. With the advent of MRI and MR angiography and digital subtraction angiography, the prevalence and natural history of CVST are being refined [16,17,18]. Risk factors for CVST include systemic noninfectious conditions such as pregnancy and puerperium, hyper viscosity syndromes, Bechet’s disease, coagulopathies including activated protein C resistance and factor V Leiden mutation [19,20,21]. and collagen vascular diseases [22,23,24]. The presence of a PL (a CL or LA) has been suggested as a risk factor for CVST [6,11,25,26]. but the clinical, radiological, and outcome profiles have not been determined or systematically studied, mainly because of the scarcity of the reported cases.
The pathogenesis of thrombosis associated with antiphospholipid syndrome is not clearly understood. Recently, antibodies against the ᵝ2-GPI-phospholipid complex [27,28]. prothrombin-phospholipid complex [4]. protein S-phospholipid complex [28]. and activated protein C-phospholipid complex [28]. have been detected in the serum of patients with antiphospholipid syndrome. ᵝ2--GPI is a cofactor which is necessary for the binding of a CL to cardiolipin. Thea CL reacts with the ᵝ2--GPI-cardiolipin complex which inhibits the prothrombinase activity of platelets and the generation of factor X a on the surface of activated platelets in patients with antiphospholipid syndrome [27,29,30,31]. In addition, a slightly decreased protein S antigen level and moderately decreased protein S activity level was detected in the present case. These findings might be related to the presence of antibody against the protein S phospholipid complex. Protein S has an anticoagulant function by directly binding to factor V a, and this function is independent of activated protein C [32].
Molecular mimicry has been demonstrated in experimental models between B2GPI related peptides and bacterial, viral and tetanus toxoids suggesting that in predisposed individuals contact with microorganisms or their products could activate potentially autoreactive lymphocytes [33,34].
The etiologies of sinus and cerebral venous thrombosis can be divided into infectious and non-infectious types. Various non-infectious etiologies, such as pregnancy, post-partum, oral contraceptives, head injury, tumors, Bechet’s disease, nephritic syndrome, have been reported [35]. However, 10 of 38cases of sinus and cerebral venous thrombosis had no definite etiology [35]. The presence of a CL or LA was not examined in these cases. Recently, tests for a CL and LA were made in a series of 40 patients with cerebral venous thrombosis, finding a CL or LA in four patients [36]. An increased a CL level was founding three of another series of 40 patients with cerebral venous thrombosis [20]. These reports suggest that some patients with a diagnosis of sinus and cerebral venous thrombosis of unknown etiology may have primary antiphospholipid syndrome. Therefore, primary antiphospholipid syndrome should be considered in the evaluation of patients with sinus and cerebral venous thrombosis of unknown etiology.
The majority of cerebrovascular disorders associated with antiphospholipid syndrome by thrombosis or thromboembolism [8,11]. Sinus and cerebral venous thrum bosses relatively rare. The nine reported cases [11,25,37,38]. showed no specific features in terms of the CT findings and neurological symptoms, like sinus sand cerebral venous thrombosis of other etiologies. However, serological studies showed a positive LA test result and/or increased acyl level in all cases. These nine patients, four males and five females, were aged from 21 to 52 years (average 35.6 years). Four of the five females had experienced one or more spontaneous abortions, and sinus and cerebra venous thrombosis occurred during pregnancy or just after delivery in three. Four patients developed there arterial and/or venous thrombosis, and five had thrombocytopenia. Three cases were associated with systemic lupus erythematosus. All nine patients were treated with anticoagulants (heparin and/or warfarin) and/or platelet-activating agent(aspirin), and seven patients with steroids. Craniotomy was performed in two of the three patients under a diagnosis of hemorrhagic infarction. One patient with superior sagittal sinus and transverse sinus thrombosis received a local injection of urokinase. These procedures all yielded good results.
Features of cerebral venous sinus thrombosis include symptoms of raised intracranial pressure and papilla edema in chronic cases and impaired consciousness, seizures and focal symptoms/signs in acute cases. MRI with MR venography of brain is the investigation of choice to diagnose CVST. Treatment options for CVST include treatment of underlying condition heparin/warfarin in acute presentations, acetazolamide/steroids for raised intracerebral pressure, anticonvulsants for seizures, antiplatelet agents multiple cerebral venous sinus thrombosis is very rare. In a recent study from India, out of a series of CVT cases, only 20% were multiple [39]. The mortality in this group of patients was extremely high. We report this case to highlight this rare complication of APS. Such a manifestation of primary APS has been reported once previously from the subcontinent [40].
Our report expands the cerebrovascular manifestations associated with LAs to include CVST and should be considered in the differential diagnosis of cerebral venous thrombosis. The case demonstrates the importance of screening for antiphospholipid antibodies inpatients presenting with cerebral venous sinus thrombosis. In patients where such antibodies are identified clinicians should be aware not only of the risk of recurrent thrombosis but also of the possible later development of associated immunologically mediated conditions.
None declared
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
