
Case Report | DOI: https://doi.org/10.31579/2578-8965/188
Post graduate institute of Medicine, University of Colombo, Sri Lanka. India
*Corresponding Author: Walawe Nayaka S, post graduate institute of Medicine, University of Colombo, Sri Lanka.
Citation: Walawe Nayaka S (2023), Primary Amenorrhea Due to Ovotesticular Disorder of Sexual Development, J. Obstetrics Gynecology and Reproductive Sciences, 7(6) DOI:10.31579/2578-8965/188
Copyright: © 2023, Walawe Nayaka S. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 September 2023 | Accepted: 15 September 2023 | Published: 22 September 2023
Keywords: primary amenorrhea; hermaphroditism; ovotesticular; disordered sexual development
Primary amenorrhea with ambiguous genitalia is a diagnostic challenge to physicians. Ovotesticular disorder of sexual development is a one cause for that which need gonadectomy followed by histological assessment to confirm the diagnosis. This is a case of ovotesticular disorder of sexual development which presented with primary amenorrhea with ambiguous genitalia.
Primary amenorrhea (PA) is defined as absence of menstruation at the age of 14 years in a girl without secondary sexual characteristics or absence of menstruation at the age of 16 years in a girl with secondary sexual characteristics1. As highlighted by the definition, investigations should be started at the age of 14 years (if secondary sexual characteristics are absent) or at the age of 16 years (if secondary sexual characteristics are present). Diagnosing and management of PA is always a challenge to both health care provider and the patient which demands multi-disciplinary approach.
Out of the causes for the PA in a girl not having secondary sexual characteristics, abnormal gonadal development is a cause which creates a
diagnostic dilemma. Having gonads which contain both testicular and ovarian tissues which called as ’ovotestis’ leads to ovotesticular disorder of sexual development (ODSD), usually detected during child hood due to the investigations for ambiguous genitalia. ODSD is previously termed as intersex disorders which describe a group of disorder where individuals have discrepancy between their phenotype, genetic materials and gonads2.
Lawson Wilkins Pediatric Endocrine Society (LWPES) and the European Society for Pediatric Endocrinology (ESPE) suggested a new terminology for individuals with intersex disorders in 20063,4.
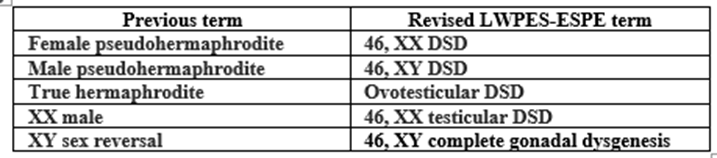
Table 1: Revised LWPES-ESPE terminology for intersex disorders
Thus, ODSD is true hermaphroditism according to the previous nomenclature which the diagnosis totally depends on the histological assessment of the gonads. In other words, it can’t be diagnosed based on karyotyping or internal and external genitalia even though the external
genitalia are ambiguous5. ODSD may present in various ways. Most of them (60%) will have bilateral ovotestis while others have unilateral ovotestis with contralateral ovary or testis2. Very rarely they may present with separate ovary and separate testis on the same side. Histologically ovarian tissues and testicular tissues are compartmentalized by an intervening connective tissue layer.
60% of ODSD individuals are having 46, XX karyotype while 15% are having 46, XY karyotype. Others show various forms of mosaicism. Thus, ODSD is a genetically heterogenous condition2. Genetic chimerism, non-disjunction, XY translocation, mutation and occult mosaicism are the theories used to describe the various phenotypic forms of ODSD. Even though these individuals have ambiguous genitalia, only 25% of them are diagnosed to have ODSD before the age of 5 years2. ODSD accounts only for less than 10% of all sexual development disorders and more common among southern African population.
2.6% of these individuals have gonadal malignancy risk and this is highest among 46, XY karyotype. Dysgerminomas, seminomas, gonadoblastomas, and yolk sac carcinomas have been reported as malignant tumors while mucinous cystadenomas, benign teratomas, and Brenner tumors have been reported as benign tumors2.
24-year-old unmarried lady presented with primary amenorrhea and absent breast development. She was the third child of the family, whom delivered vaginally following uncomplicated pregnancy. She was assigned as a female infant at the time of delivery and reared as a girl. She had normal growth and development during childhood without any chronic medical problems. Even though her mother noticed an abnormality of her genitalia at the age of five years, medical advice was not sought. Her parents had concerns at the age of 13 years as she didn’t have breast development in spite of having normal growth spurt. They sought medical advices at the age of 16 years as she didn’t have both breast development and menarche. Other than that, she had clitoromegaly at that time. At the end of consultation, they were told that she was a genetic male and need to be clarified by karyotyping. Parents didn’t accept this diagnosis and defaulted the follow up. She maintained her female role in the society with the aid of prosthesis as she didn’t have breast development.
Further questioning revealed she had normal height gain during pubertal period. She never had cyclical abdominal pain, skull injury, intracranial infections, symptoms suggestive of space occupying lesion of the brain, abdominopelvic irradiation and abdominopelvic surgeries.
On examination her height was 163cm, weight was 53kg with BMI of 20kg/m2. She had no acne, hirsutism, webbed neck, wide carrying angle and thyroid enlargement. Her scalp hair growth pattern, axillary hair and pubic hair pattern were normal (Tanner stage 5). Her breast development was absent (Tanner stage 1) and there were no any nipple discharges. Her urethral meatus noted just below the enlarged clitoris and labioscrotal folds were completely fused in the mid line without any bulging. Her anal opening was appeared normal and there were no any palpable masses on inguinal regions. Her cardiovascular and respiratory system examination was normal. There were no any palpable abdominopelvic masses.
Summary of the investigations as follows:
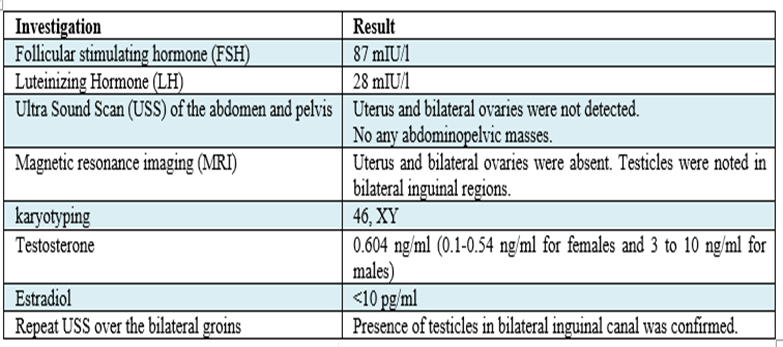
Table 2: Summary of investigations
Multi-disciplinary team (MDT) meeting was arranged and agreed to proceed with laparoscopic gonadectomy followed by hormone replacement to stimulate breast development and support the maintenance of female role. After adequate counselling, she agreed for the decision and underwent laparoscopic gonadectomy. Histology revealed the presence of both testicular and ovarian tissues in the both gonads which confirmed the ovotesticular disorder of sexual development. She was started on estrogen only hormone replacement therapy and she achieved successful breast development. She agreed for neo vagina creation before the marriage.
Delayed presentation to seek medical advice is the main weak point from the patient’s side. If she presents early, the diagnosis could have been made earlier and psycho-social suffering could have been minimized. Missing the diagnosis of ambiguous genitalia at birth of this patient is the main weak point from the health care provider’s side.
As she presented with PA without breast development, her investigations should be started with FSH. Her high FSH value suggests that either her gonads not producing sex hormones or functions of the sex hormones not happening at receptor level and onwards. Performing karyotyping is justifiable as she is having ambiguous genitalia. In this case karyotyping helped to narrow down the working out pathway.
A 46, XY women with PA and clitoromegaly should be investigated to locate the gonads as they need surgical excision to prevent malignant transformation. Best imaging modality is MRI. If the MRI facilities are not freely available, USS would be a good alternative with expert operating hands.
But having normal axillary and pubic hair growth in the absence of normal external genitalia development is a question. Normal axillary and pubic hair growth suggest that she is responding to circulating androgens. Her clitoromegaly during pubertal period suggest that the external genitalia responding to circulating androgens. So, the reason behind ambiguous genitalia may be an undiagnosed 5-alpha reductase deficiency. 5-alpha reductase (5AR) is an essential enzyme which need to convert testosterone into dihydro testosterone (DHT), which is the essential form of testosterone need to form external male genitalia during the fetal life. Even though her testosterone level is normal for a female, it is below the normal male testosterone level. That indicates this patient’s testicular tissues producing sub optimal level of testosterone. That may be the reason for the elevated FSH levels. But these testicular tissues have been able to produce adequate amount of Mullerian inhibitory substance (MIS) proven by absence of any Mullerian structures in MRI scan.
After considering all these investigation findings, the best management would be the bilateral gonadectomy followed by HRT to maintain female role and stimulate breast development. This prevents the risk of malignant transformation of the gonads and prevent the added psychological stress due to gender transformation.
Counselling plays a major role in this case. Patient should be given the optimal support to maintain female role. She should be told that she can’t give a birth to her own child. Adoption would be the only available option for her to enter into a mother’s role in future. She should be reassured that she can have a near normal sexual life as a female by neo vagina creation and the usage of vaginal lubricants. But this should be done when she is ready for a sexual life.
She should have regular psycho-sexual counselor’s help to maintain normal sexual drive, normal female sexual orientation which is accepted by her surrounding culture and reduce psycho social stress due to this DSD.
ODSD is a rare problem which usually presents with ambiguous genitalia at birth. Late presentation at the time of puberty creates lot of problems which need comprehensive history, examinations, proper investigations and management with multi-disciplinary team to minimize the adverse psycho sexual effects to the patient.
Not applicable.
None.
None.
None.
As this is a case report which do not contain any patient identification details, ethical approval is not required.
Informed written consent was obtained from the patient
The author confirms sole responsibility for study conception and design, data collection, analysis and interpretation of results, and manuscript preparation.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
