
Case Report | DOI: https://doi.org/10.31579/2640-1053/119
1 Department Of Radiation Oncology, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India.
2 Senior Resident, Department of Radiation Oncology, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India.
*Corresponding Author: Haritha V.S, Senior Resident, Department of Radiation Oncology, Netaji Subhash Chandra Bose Medical College, Jabalpur, Madhya Pradesh, India.
Citation: Haritha V.S. (2022). Primary Adrenal Lymphoma. Cancer Research and Cellular Therapeutics. 6(3); Doi:10.31579/2640-1053/119
Copyright: © 2022 Haritha V.S, this is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 18 April 2022 | Accepted: 06 May 2022 | Published: 16 May 2022
Keywords: primary adrenal lymphoma; rare
Primary adrenal lymphoma is a rare disease entity with only less than 200 cases reported till date. We have seen a single case among the 260 cases reported in our hospital in the last 5 years. Review of the English literature showed 65 such cases reported so far most of them being single case reports. The striking similarity in all of them were – median age of 68 years, bilateral involvement in 60% and predominantly diffuse large cell histology with B cell immunophenotype. adrenal insufficiency was seen in two – thirds of them at diagnosis. About one half respond to treatment with median survival of 4 months. A high index of suspicion is needed for early diagnosis and prompt treatment. We herein report a case of a 65-year-old male who was diagnosed with primary adrenal lymphoma.
Adrenal lymphoma consists of primary and secondary adrenal lymphoma. Secondary adrenal lymphoma accounts for approximately 4% to 5% of all non-Hodgkin lymphoma cases, and primary adrenal lymphoma (PAL) is extremely rare, accounting for only approximately 1% of non-Hodgkin lymphoma cases [1]. Primary adrenal tumors are most commonly adenomas
or carcinomas [2]. Primary adrenal lymphomas is usually a non-Hodgkin lymphoma, with diffuse large B-cell lymphoma being the most common subtype, and seen in about 70% of patients [3-6]. PAL tends to affect elderly males aged 60 to 70 years old with a male-to-female ratio of approximately 1.8:1, usually involving bilateral adrenal glands (70%), with an average diameter of 8 cm. Most patients with PAL show adrenal insufficiency, B symptoms (fever, night sweats, weight loss), etc, and most patients can be accompanied by elevated lactate dehydrogenase (LDH) and Epstein–Barr virus (EBV) positivity [1]. The characteristic clinical features also include a high incidence of bilaterality and a low incidence of extra-adrenal disease at diagnosis [7] In the imaging examination, PAL mostly presents as bilateral or unilateral large adrenal masses without the appearance of normal adrenal tissue. However, how PAL develops from the adrenal gland is still unclear [1].
Patients with PAL usually have a poor prognosis [8]. Recently, studies have suggested that BCL-2 and MYC co-expression predict poor prognosis in patients with diffuse large B-cell lymphoma (DLBCL), but there are few reports on BCL-2 and MYC co-expression in patients with PAL [9].
Herein we report a case of primary adrenal lymphoma in a 65 year old elderly man who had presented at our centre.
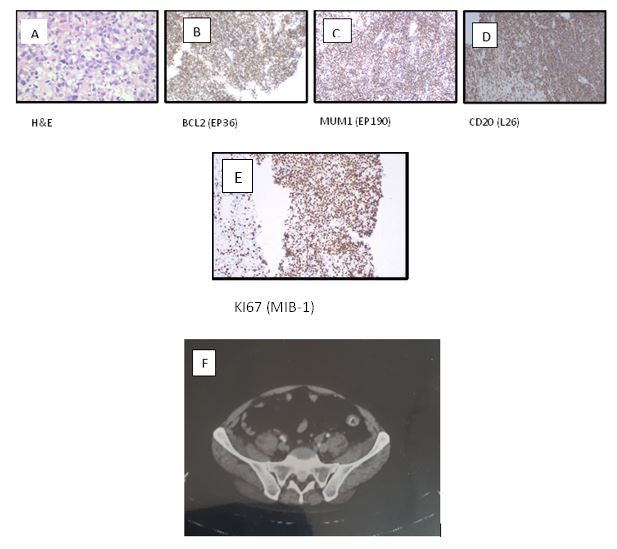
A 65 year old elderly man without significant co-morbid conditions who was diagnosed to have bilateral adrenal masses in an ultrasonography done as a part of workup for abdominal pain with bilateral lower limb pain with reduced appetite for 2 months. He didn’t have complaints of fever, night sweats or weight loss. Ultrasonography showed heteroechoic well defined mass lesion in the bilateral supra renal region with internal vascularity of size 100 x 80 mm on right side and 57x43 mm on left side. A contrast enhanced computed tomography of abdomen and pelvis was later done which showed well defined mass lesion in bilateral supra-renal region of size 12x10x10 cm on right side and 7x6.5x6 cm on left side. No calcification or cystic changes were seen. His blood biochemistry was done which showed a deranged renal function tests. Blood urea was 53.5 mg/dl, serum creatinine was 1.5 mg/dl, serum uric acid was 8.5 mg/dl, serum phosphorous was 6.60 mg/dl, serum sodium was 126 mmol/l, serum potassium was 5.3 mmol/l, serum chloride was 95 mmol/L. A ultrasonography guided biopsy (Panel A) was done from the adrenal masses which reported as high grade non hodgkins lymphoma – diffuse large B cell variety (non – germinal centre variety) after IHC confirmation. IHC showed positivity for CD 20, BCL2, BCL 6 and MUM1(Panel B,C,D) and tumour cells were negative for CD10, CD3,SOX11 and CK. Ki- 67 was 85 -90%.(Panel E) A whole body PET- CT was done to look for primary elsewhere which reported no evidence of primary disease elsewhere . It reported bilateral adrenal lesion with perilesional fat stranding (right - SUV max -11.8, left – 11.6), (Panel F) Multiple enlarged lymph node groups were found in the abdominopelvic, left inguinal (SUV max – 6.2), mediastinal (SUV max – 4.8, and left cervical and supraclavicular region (SUV max -2.6) with mild ascites. A stage IV disease was thus diagnosed and the patient was started on chemotherapy with R-CHOP regimen. At present he has completed 4 cycles of chemotherapy with the same regimen with good symptomatic response.
Primary adrenal lymphomas are rare, but remain a diagnostic possibility in the evaluation of adrenal masses. The diagnosis of a patient with primary adrenal lymphoma can be challenging because symptoms are non-specific, and only 50% of patients have concomitant adrenal insufficiency, which occurs when there is at least 90
This case report concludes that timely diagnosis and treatment with R-CHOP regimen is key in improving the survival outcome in patients with PAL. This condition must be kept in mind when clinicians comes across large bulky bilateral adrenal masses in imaging.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
