
Research Article | DOI: https://doi.org/10.31579/2578-8965/231
1King Abdulaziz Medical City. Saudi Arabia.
2Umm Al-Qura University
3King Faisal Specialist Hospital & Research Centre
*Corresponding Author: Rahaf Abdulhai King Abdulaziz Medical City. Saudi Arabia.
Citation: Rahaf A. Ghazzawi, Fadwa H. Taher, Raed A. Sayed, Raghad A. Ghazzawi, Hawazen M. Alsulaimani, Waad I. Barnawi, et al, (2024), Prevalence of Polycystic Ovarian Syndrome and its Relation to Urinary Tract Symptoms among Female Medical Students of Umm Al-Qura University, J. Obstetrics Gynecology and Reproductive Sciences, 8(8) DOI:10.31579/2578-8965/231
Copyright: © 2024, Rahaf Abdulhai Ghazzawi. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 19 July 2024 | Accepted: 29 July 2024 | Published: 18 November 2024
Keywords: pcos; androgens; obesity; menstrual irregularity; urinary symptoms
Background / Aim:
Polycystic ovarian syndrome (PCOS) affects women of reproductive age. Lower urinary tract symptoms (LUTS) are characterized by urgency, frequency, and dysuria. Limited information is available regarding the possible association between PCOS and LUTS. This study aimed to determine the prevalence of PCOS among female medical students and the association between PCOS and LUTS.
Materials and Method: This cross-sectional study was carried out in the Umm Al-Qura University, Makkah, Saudi Arabia. The study was conducted from August to December 2022. An online, self-administered, and validated Arabic-based survey was conducted using Google Forms.
Results: The prevalence of PCOS among the female medical students was 21.6% (n=42). The participants reported urinary tract symptoms; the most reported symptom was pelvic pain (61.9%), followed by urinary frequency (35.7%). A total of 72% of females with an intermenstrual (IM) period of < 21 days had PCOS versus 12.2% of those with variable IM periods, displaying statistically significant differences (P=.001). In addition, 71% of females with dark coarse hair on the belly had PCOS, compared to those with hair on other body parts (P=.001). PCOS was diagnosed in 57.1% of obese/overweight females and 9.7% of females with normal body mass index (P=.001). Similarly, 57.1% of currently obese females were diagnosed with PCOS, whereas 12.5% of those with normal body weight had PCOS (P=.001). Approximately 90.9% of females with milky nipple discharge had PCOS (P=.001).
Conclusions: The prevalence of PCOS among female medical students is surpassing the global average; hence, awareness campaigns and educational programs must be conducted in schools and colleges to spread awareness among young girls.
LUTS is a multifactorial diagnosis with no direct link to PCOS. The sample size of this study was small. Therefore, a cross-sectional study with a larger sample size is needed to investigate the association between PCOS and LUTS.
Polycystic ovarian syndrome (PCOS) is a metabolic and endocrine disorder [1]. Moreover, PCOS is a disease that affects 4–21% of females of reproductive age worldwide [2]. It is characterized by numerous symptoms such as hirsutism, amenorrhea, oligomenorrhea, obesity, acne vulgaris, infertility, alopecia, insulin resistance, and hyperandrogenism [3, 4]. Furthermore, PCOS can lead to complications, such as infertility, dysfunctional uterine bleeding, and several metabolic disorders, including insulin resistance, diabetes mellitus, hypertension, dyslipidemia, and cardiovascular disease [5].
Lower urinary tract symptoms (LUTS) are characterized by three main symptoms: storage symptoms such as urgency, frequency, nocturia, and urge incontinence; voiding symptoms such as poor and/or intermittent stream; and post-voiding symptoms such as the feeling of incomplete emptying [5]. In cases where LUTS exceed the critical threshold, the quality of life is impaired, the level of physical activity is decreased, and psychological condition is negatively affected [6]. Large-scale epidemiological studies have reported that, on average, 84% of females experience at least one LUTS during their lifetime [6].
A study conducted in 2021 in Iraq demonstrated that a significant number of females with PCOS suffer from LUTS, such as the urge to urinate, polyurea, and cloudy urine [7]. Moreover, another study conducted in 2023 discovered that PCOS and LUTS are closely associated, emphasizing the importance of a detailed urinary system evaluation in females with PCOS. (6) However, limited information is available on the possible association between PCOS and urinary tract symptoms. This study aimed to determine the prevalence of PCOS among female medical students and the prevalence of urinary tract symptoms in patients with PCOS.
Study design, setting, time, and study participants: This is a cross-sectional study performed at Umm Al-Qura University (UQU) in Makkah, Saudi Arabia. The study was conducted between August and December 2022.
Inclusion criteria included all female medical students at UQU who agreed to participate from the second year (batch 43) until the internship year (batch 38).
Exclusion criteria included pregnancy, females using contraceptive pills or injections, females who had undergone bilateral oophorectomy or hysterectomy, and individuals with diabetes requiring hypoglycemic drugs.
Sample size: The required sample size for this study was 194 participants, with a 95% confidence level and a margin of error of 5%. The calculations were performed using the Rasoft sample size calculator based on the number of female medical students at UQU, which was 194.
Data collection: A self-administered online questionnaire via Google Forms consisted of 11 questions divided into three main sections. The first section aimed to obtain participants’ consent to participate in the study while clarifying the exclusion criteria, followed by a section on each individual's medical history regarding menstruation and PCOS symptoms, and finally, a section to confirm the presence of a relationship between the individual's medical history and urinary tract infection symptoms. The questionnaire is provided in the Appendix.
Ethical approval and confidentiality: Ethical approval for this study was obtained from the Institutional Research Board (IRB) approval no. (HAPO-02-K-012-2023-08-1699).
Data management and statical analysis: The data were collected, reviewed, and fed into the Statistical Package for Social Sciences version 21 (SPSS: An IBM Company). All statistical methods used were two-tailed with an alpha level of 0.05 considering significance if the P-value was ≤ 0.05. Descriptive analysis was performed by providing the frequency distribution and percentage of the study variables, including female demographic data and income. In addition, the PCOS-related symptoms experienced by females, their history of being diagnosed with PCOS, and the effect of PCOS on their daily lives were tabulated. Moreover, the prevalence of PCOS and associated urinary symptoms were depicted graphically. Crosstabulation was used to assess the factors associated with PCOS among female medical students, based on the chi-square test and exact probability test for small-frequency distributions. Furthermore, multiple regression analysis was performed to assess the predictors of PCOS among the study participants by assessing the adjusted odds ratio (OR) with a confidence interval (CI) of 95%.
In total 194 female medical students were included in this study. Among them, 73 (37.6%) reported an average annual income of < 100000 SR, 79 (40.7%) reported approximately 100000 SR, and 42 (21.6%) reported> 100000 SR. Regarding menstrual cycle days, 25 (12.9%) reported < 21 days and 27 (13.9%) reported 21–35 days, but most of the females (71.6%; 139) reported them to be variable (Table 1).
| Demographics | No | % |
| Average income per year | ||
| < 100000 days | 73 | 37.6% |
| Approximately bout 100000 SR | 79 | 40.7% |
| > 100000 SR | 42 | 21.6% |
| Intermenstrual cycle days | ||
| <21 days | 25 | 12.9% |
| 21-35 days | 27 | 13.9% |
| > 35 days | 3 | 1.5% |
| Variable | 139 | 71.6% |
Table 1: Biodemographic data of female medical students at Umm Al-Qura University
Table 2 displays the symptoms of PCOS in female medical students at UQU. The most common sites of dark coarse hair were the legs (39.2%), arms (37.6%), face (23.2%), upper lips (19.6%), and belly (16%). The least reported sites were the back (6.7%) and chest (5.7%). A total of 49 (25.3%)
patients were obese or overweight from the age of 16 years, 40 (20.6%) were underweight from the age of 16 years. Regarding current body mass index (BMI), 136 (70.1%) had normal weight, 36 (18.6%) were overweight, 7 (3.6%) were obese, and 15 (7.7%) were underweight. Eleven (5.7%) patients noticed a milky discharge from their nipples, and 39 (20.1%) reported that these symptoms affected their daily lives.
The prevalence of PCOS among female medical students at UQU is demonstrated in Figure 1. A total of 42 (21.6%) participants were diagnosed with PCOS or experienced some of the previously described symptoms of PCOS while 152 (78.4%) did not.
Figure 2 displays the urinary tract symptoms among medical female students with PCOS at UQU. The most common urinary symptoms were pelvic pain (61.9%), frequent urination (35.7%), urgency (16.7%), nocturia (16.7%), incontinence (9.5%) and dysuria (2.4%).
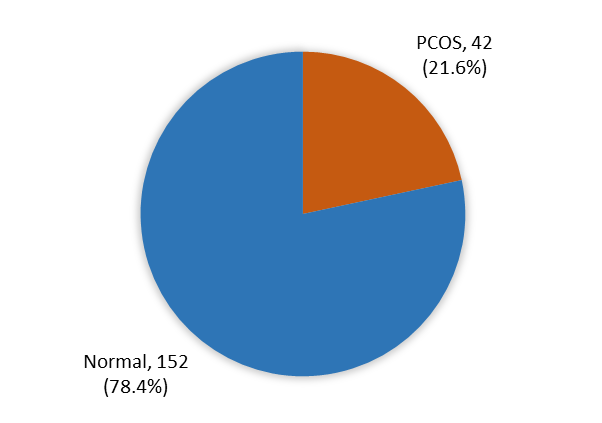
Figure 1: Prevalence of PCOS among female medical students of Umm Al-Qura University
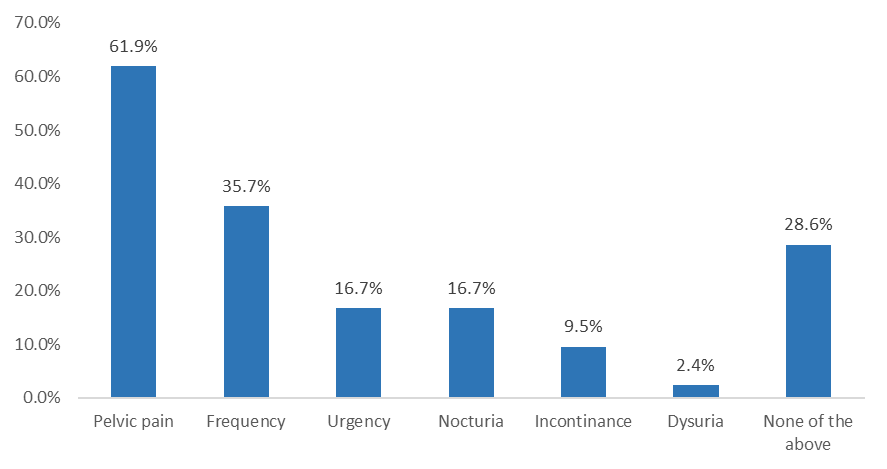
Figure 2: Urinary tract symptoms among female medical students with PCOS at Umm Al-Qura University
Factors associated with PCOS among female medical students at UQU are depicted in Table 3. A total of 72% of females with an intermenstrual (IM) period of <21 days had PCOS versus 12.2% of others with variable IM periods, displaying statistically significant differences (P=.001). In addition, 71% of females with dark coarse hair on the belly had PCOS, compared to 69.2% with hair on the back, 68.4% with hair on the upper lip, and 3.5% without dark coarse hair (P=.001). PCOS was diagnosed in 57.1% of obese/overweight females and 9.7% of females with normal body mass index (P=.001)”). Similarly, 57.1% of currently obese females were diagnosed with PCOS, whereas 12.5% of those with normal body weight had PCOS (P=.001). Approximately 90.9% of females with milky nipple discharge had PCOS, in contrast to 17.5% of those without milky nipple discharge (P=.001).
A multiple logistic regression model was used to assess predictors of PCOS among female medical students (Table 4). Among all included factors, the IM period demonstrated an elevated risk of PCOS for all periods compared to the risk observed in < 21 days (OR range from 25 for 21–35 days to 6.7 for> 35 days). In addition, females who were overweight or obese from the age of 16 years were 11 times more likely (OR=11.6) to have PCOS than those with normal body weight. Moreover, those with dark coarse hair also demonstrated an 11 times higher likelihood of having PCOS (OR=11.3) than those without dark coarse hair.
| PCOS symptoms | No | % |
| During your menstruating years (not including during pregnancy), did you tend to grow dark, coarse hair on | ||
| Legs | 76 | 39.2% |
| Arms | 73 | 37.6% |
| Face | 45 | 23.2% |
| Upper lip | 38 | 19.6% |
| Belly | 31 | 16.0% |
| Back | 13 | 6.7% |
| Chest | 11 | 5.7% |
| None of the above | 113 | 58.2% |
| Were you ever obese or overweight from the age of 16 till now? | ||
| Yes | 49 | 25.3% |
| No | 145 | 74.7% |
| Were you ever underweight since the age of 16 till now? | ||
| Yes | 40 | 20.6% |
| No | 154 | 79.4% |
| Body mass index | ||
| <18.5 (Underweight) | 15 | 7.7% |
| 18.5–24.9 (Normal) | 136 | 70.1% |
| 25–29.9 (Overweight) | 36 | 18.6% |
| 30–39.9 (Obese) | 7 | 3.6% |
| Since the age of 16 till now, have you ever noticed a milky discharge from your nipples? | ||
| Yes | 11 | 5.7% |
| No | 183 | 94.3% |
| Are these symptoms affecting your daily life? | ||
| Yes | 39 | 20.1% |
| No | 155 | 79.9% |
Table 2: Symptoms of PCOS as reported among female medical students, at Umm Al-Qura University
| Factors | PCOS | p-value | |||
| Yes | No | ||||
| No | % | No | % | ||
| Average income per year | .422 | ||||
| < 100000 SR | 17 | 23.3% | 56 | 76.7% | |
| About 100000 SR | 19 | 24.1% | 60 | 75.9% | |
| >100000 SR | 6 | 14.3% | 36 | 85.7% | |
| Intermenstrual cycle days | .001*^ | ||||
| < 21 days | 18 | 72.0% | 7 | 28.0% | |
| 21–-35 days | 5 | 18.5% | 22 | 81.5% | |
| > 35 days | 2 | 66.7% | 1 | 33.3% | |
| Variable | 17 | 12.2% | 122 | 87.8% | |
| During your menstruating years (not including during pregnancy), did you tend to grow dark, coarse hair on | .001* | ||||
| Face | 27 | 60.0% | 18 | 40.0% | |
| Upper lip | 26 | 68.4% | 12 | 31.6% | |
| Arms | 35 | 47.9% | 38 | 52.1% | |
| Chest | 7 | 63.6% | 4 | 36.4% | |
| Back | 9 | 69.2% | 4 | 30.8% | |
| Belly | 22 | 71.0% | 9 | 29.0% | |
| Legs | 37 | 48.7% | 39 | 51.3% | |
| None of the above | 4 | 3.5% | 109 | 96.5% | |
| Were you ever obese or overweight from the age of 16 till now? | .001* | ||||
| Yes | 28 | 57.1% | 21 | 42.9% | |
| No | 14 | 9.7% | 131 | 90.3% | |
| Were you ever underweight since the age of 16 till now? | .061 | ||||
| Yes | 13 | 32.5% | 27 | 67.5% | |
| No | 29 | 18.8% | 125 | 81.2% | |
| Body mass index | .001*^ | ||||
| <18.5 (Underweight) | 3 | 20.0% | 12 | 80.0% | |
| 18.5 - 24.9 (Normal) | 17 | 12.5% | 119 | 87.5% | |
| 25 - 29.9 (Overweight) | 18 | 50.0% | 18 | 50.0% | |
| 30 - 39.9 (obese) | 4 | 57.1% | 3 | 42.9% | |
| Since the age of 16 till now, have you ever noticed a milky discharge from your nipples? | .001*^ | ||||
| Yes | 10 | 90.9% | 1 | 9.1% | |
| No | 32 | 17.5% | 151 | 82.5% | |
P: Pearson X2 test ^: Exact probability test
* P< 0.05 (significant)
Table 3: Factors associated with PCOS among female medical students of Umm Al-Qura University
| Factors | P-value | AOR | 95% CI of OR | |
| Lower | Upper | |||
| Intermenstrual cycle days | ||||
| 21–35 vs. < 21 days | 0.001* | 25.0 | 3.5 | 178.6 |
| > 35 vs. < 21 days | 0.229 | 6.7 | 0.3 | 150.6 |
| Variable vs.< 21 days | 0.002* | 9.4 | 2.2 | 39.1 |
| Were overweight/obese since the age of 16 till now | 0.003* | 11.6 | 2.3 | 58.7 |
| Were underweight from the age of 16 till now | 0.094 | 2.8 | 0.8 | 9.4 |
| Body mass index | 0.415 | 1.6 | 0.5 | 5.3 |
| Milky discharge from nipples | 0.141 | 7.2 | 0.5 | 100.7 |
| Have dark coarse hair | 0.001* | 11.3 | 3.4 | 38.0 |
AOR: adjusted odds ratio CI: confidence interval* P < 0.05 (significant)
Table 4: Multiple logistic regression model to assess predictors of PCOS among female medical students
In the United States, PCOS is the most common endocrine disorder affecting women of reproductive age [8].
The worldwide prevalence of PCOS is estimated to be 6–7% [9]. The prevalence of PCOS in our study was 21.6%, which is higher than the prevalence. This high prevalence may indicate a lack of information and awareness about PCOS among medical students. This lack of knowledge can lead to inappropriate lifestyle behaviors, which further exacerbate the risk of PCOS.
One meta-analytic study investigated the prevalence and health consequences of PCOS medical students. A complete search of seven recent studies (2019–2022) was conducted, and relevant data were retrieved and summarized. The pooled prevalence of PCOS was 24.7% among 2498 female medical students included in this meta-analysis and systematic review [10]. The results of the aforementioned study were comparable to our findings.
Another study among students at a tertiary care teaching hospital had a significant prevalence of PCOS (32.11%) [11]. The annual cost of diagnosing and treating PCOS in the American healthcare system is estimated to be $4 billion [8].
Thus, obesity may play a significant role in the development of PCOS. Weight gain can exacerbate insulin resistance, which not only increases testosterone production but also disrupts ovulation. Therefore, motivating females upon diagnosis to follow a diet and exercise plan that will assist in weight loss, menstrual cycle regulation, emotional well-being, and the reduction of insulin resistance is imperative [12].
In our study, 49 (25.3%) patients were obese or overweight from the age of 16 years, while 40 (20.6%) were underweight from the age of 16. Regarding current BMI, 136 participants (70.1%) had normal weight, 36 (18.6%) were overweight, 7 (3.6%) were obese, and 15 (7.7%) were underweight. These findings are consistent with the results of previous studies. Other studies have confirmed the association between obesity and PCOS in medical and dental students.
In a study conducted in Nepal, 20.73% of the participants reported being obese or overweight, either currently or at some point in the past [12]. In another study conducted in India, 62.5% of the students with PCOS were overweight or obese [13]. In a study conducted in Pakistan, 36.3% of the students with PCOS who participated were obese [14].
Menstrual irregularities are known to increase among medical students who undergo dietary, lifestyle, and stress-related changes. Overactivation of the hypothalamic-pituitary (HP) axis psychological stress increases plasma cortisol levels, which in turn can cause menstrual disturbances [15]. In our study we identified menstrual irregularities among medical students. For instance, 25 (12.9%) participants reported a menstrual cycle of < 21>
Therefore, medical and dentistry students should be encouraged to pay attention to the early symptoms of irregular menstrual cycles and obesity and receive medical assistance to facilitate early diagnosis and treatment, as well as to prevent comorbidities associated with PCOS. Patients with PCOS may exhibit hirsutism on various body parts. The presence of excess male gender hormones such as testosterone, dihydrotestosterone, dehydroepiandrosterone sulfate, and androstenedione is the reason behind the development of such hair. The degree of hirsutism varies in individuals affected with PCOS, owing to variations in the sensitivity of hair follicles to excess androgens [18].
In our study, we found that 71% of females with dark coarse hair on the belly had PCOS, compared to 69.2% with hair on the back, 68.4% with hair on the upper lip, and 3.5% without dark coarse hair (P=.001). In clinical practice, the Ferriman-Gallwey scoring system is frequently used to visually examine body hair patterns and rate excessive terminal hair [19–20]. In our study, dark coarse hair was distributed as follows: legs (39.2%), arms (37.6%), face (23.2%), upper lips (19.6%), and bellies (16%). The back and chest were the least frequently affected (6.7% and 5.7%, respectively).
Anatomical and neuroendocrine factors are required for voiding physiology. Furthermore, LUTS occur when this dynamic is disrupted. The lower urinary system is affected by the inflammatory and metabolic effects of PCOS. Patients with PCOS experience a significantly diminished quality of life when urinary symptoms are present [6].
Many changes occur in bladder dynamics in patients with PCOS. For instance, the effects of changes in androgen levels on the urinary bladder have been emphasized in many studies. In a study that investigated rats undergoing oophorectomy, low levels of androgen and estrogen reduced bladder capacity and compliance; however, function was restored after hormone therapy [21]. Another study evaluating the effect of testosterone on rat bladders demonstrated an increase in bladder capacity and smooth muscle/collagen content [22]. Moreover, a study noted no statistically significant differences in pelvic floor muscle strength between females with PCOS and controls. However, the control group had a higher incidence of urinary incontinence (UI) than the PCOS group [23]. Another study reported similar results and identified a correlation between bladder symptoms, such as nocturia, dyspareunia, urgency, and testosterone levels in females with PCOS. However, no statistically significant relationship was observed between ultrasonographic results such as bladder capacity, post-void residual volume (PVR), and testosterone levels [24].
Similarly, a previous study observed an increased incidence of LUTS with high testosterone levels; however, there were no significant differences in maximum flow rate, PVR, bladder capacity, or bladder wall thickness [6]. Numerous studies have examined the association between LUTS and obesity. This can be explained by the lowering collagen levels, induction of oxidative stress in the urethral mucosa, and decreased urethral elasticity. Additionally, the lower urinary system is linked to increased intra-abdominal pressure [25]. In a large study, Lai et al. identified a correlation between obesity and hyperactive bladder frequency, urinary incontinence, and stress incontinence [26]. Another study indicated that in patients with PCOS, a direct association was observed between high waist circumference, BMI, and urinary symptoms [6].
Bladder dynamics are significantly impacted by metabolic diseases [27]. A large meta-analysis revealed that patients had a 3.35-fold higher prevalence of metabolic syndrome [26]. A study performed on experimental animals indicated bladder dysfunction with increasing leukocytes in interstitial tissue, severe neutrophil infiltration surrounding the endothelium, and damage to the mitochondria of the smooth muscle of the bladder [27]. Another study revealed that 62.5% of rats exhibited detrusor hyperactivity after the development of metabolic syndrome [28].
This study had some limitations. The study population was limited to female medical students at UQU and may not be representative of the general population. The use of self-reported questionnaires may have introduced recall bias and subjectivity. Future research could expand on this study to include a large and diverse population to enhance the generalizability of the findings. Longitudinal studies should also be conducted to assess the long-term impact of PCOS on urinary tract symptoms and to explore the potential mechanisms underlying this association.
From this study, we can conclude that the prevalence of PCOS among female medical students is surpassing that of the global average; therefore, awareness campaigns and educational programs must be conducted in schools and colleges to spread awareness among young girls to help them identify the symptoms of PCOS and seek medical assistance to prevent further consequences and metabolic disorders. PCOS can develop regardless of body weight and socioeconomic status but is strongly influenced by lifestyle and obesity.
LUTS is a multifactorial diagnosis with no direct link to PCOS. The sample size of this study was insufficient to identify the prevalence of LUTS in patients diagnosed with PCOS. Therefore, a cross-sectional study with a larger sample size is needed to examine the relationship between PCOS and LUTS.
UQU: Umm Al-Qura University
PCOS: polycystic ovarian syndrome
LUTS: lower urinary tract symptoms
Ethics approval and consent to participate: Ethical approval for this study was obtained from the Institutional Research Board (IRB) (approval no. (HAPO-02-K-012-2023-08-1699).
Consent for publication: Not applicable
Availability of data and material: Not applicable
Competing interests:
The authors declare that they have no competing interests
Funding: Not applicable
RG wrote the paper; RA performed the analysis; FT contributed with analytical tools; WB approved the abstract; AS collected the data; HA designed the analysis.
The authors are grateful to the medical students who participated in this study.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
