
Research Article | DOI: https://doi.org/10.31579/2578-8965/223
1Department of Obstetrics and Gynaecology, University of Port-Harcourt Teaching Hospital, Rivers State, Nigeria.
2Department of Obstetrics and Gynaecology, Abia State University, Uturu, Nigeria.
3Department of Nursing, Coventry University, United Kingdom.
4Department of Surgery, Abia State University, Uturu, Nigeria.
5Agapecare Laboratory Services Ltd, 50 Ago Palace Way Okota, Adesola Bus Stop, Lagos State, Nigeria.
6School of Public Health, University of Port Harcourt, Rivers State, Nigeria.
7 Department of Surgery, University of Port Harcourt Teaching Hospital, Rivers State, Nigeria.
8Department of Biochemistry, Lead City University, Ibadan, Oyo State, Nigeria.
*Corresponding Author: Augustine I. Airaodion, Department of Biochemistry, Lead City University, Ibadan, Oyo State, Nigeria.
Citation: E. I. Ezebuiro, E. O. Ezirim, E. M. Akwuruoha, O. R. Omole, A. I. Airaodion, et al, (2024), Prevalence, Awareness, and Attitudes towards Breast Cancer among Women in Southeast Nigeria, J. Obstetrics Gynecology and Reproductive Sciences, 8(5) DOI:10.31579/2578-8965/223
Copyright: © 2024, Augustine I. Airaodion. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 06 June 2024 | Accepted: 14 June 2024 | Published: 24 June 2024
Keywords: breast cancer; southeast Nigeria; awareness; prevalence; risk factors; screening; healthcare access
Background: Breast cancer is a significant health challenge in Southeast Nigeria, contributing to high morbidity and mortality among women. Factors such as limited access to healthcare, lack of awareness, and cultural stigmas exacerbate the burden, leading to late-stage diagnosis and poor survival rates.
Objectives: This study aims to assess the prevalence, awareness, and attitudes towards breast cancer among women in Southeast Nigeria, and to identify the risk factors and preventive measures practiced in this region.
Materials and Methods: A cross-sectional descriptive survey was conducted in Southeast Nigeria. A stratified sampling method was used to select participants from urban and rural areas. Data were collected from 360 women using a structured. Descriptive statistics and cross-tabulations were utilized for data analysis.
Results: Awareness of breast cancer was high (96.67%), primarily obtained through the internet/social media (43.51%) and healthcare professionals (19.18%). However, knowledge about risk factors and symptoms was moderate to low, with only 14.17% considering themselves very knowledgeable. Regular breast self-examinations were practised by 30.28%, while 69.72% had never undergone clinical breast examinations. The prevalence of breast cancer diagnosis was 16.39%. Attitudes towards screening were positive, with 71.11% strongly agreeing that regular screening aids early detection. Despite this, confidence in identifying symptoms was low, with only 3.33% feeling very confident.
Conclusions: The study highlights significant gaps in knowledge and practices related to breast cancer despite high awareness levels. There is an urgent need for targeted educational programs to enhance knowledge about risk factors, symptoms, and the importance of regular screening. Improving healthcare access and addressing cultural barriers are crucial for early detection and better outcomes.
Breast cancer is the most common cancer among women worldwide and represents a significant public health concern [1]. In Southeast Nigeria, as in many other parts of Africa, breast cancer poses a critical challenge due to late-stage presentation and inadequate healthcare infrastructure. Understanding the prevalence and awareness of breast cancer in this region is essential for developing effective strategies to combat this disease.
Globally, breast cancer accounts for approximately 24.2% of all cancer cases among women, making it the most prevalent cancer in this demographic [1]. Despite advances in detection and treatment, breast cancer remains a leading cause of cancer-related mortality among women, with significant disparities in outcomes between high-income and low-income countries. In high-income countries, early detection through regular screening and advanced treatment options have substantially improved survival rates. Conversely, in low-income countries, including many in Africa, the lack of resources and awareness often results in late diagnosis and poor prognoses [2].
In Africa, breast cancer incidence and mortality rates are on the rise. The increasing urbanization, lifestyle changes, and improved life expectancy contribute to this growing burden [3]. However, African women typically present with breast cancer at more advanced stages compared to women in high-income countries. This disparity is attributed to limited access to healthcare services, cultural beliefs, and a lack of awareness about breast cancer symptoms and screening methods [4].
Nigeria, the most populous country in Africa, faces significant challenges in addressing breast cancer. The country has a high burden of breast cancer, with regional variations in incidence and mortality rates. Southeast Nigeria, in particular, has been reported to have a relatively high incidence of breast cancer, yet studies focusing specifically on this region are limited [5]. The healthcare system in Nigeria is under-resourced, with insufficient facilities for cancer screening, diagnosis, and treatment. This inadequacy is further exacerbated by a shortage of trained healthcare professionals and poor health-seeking behaviour among the population [6].
The prevalence of breast cancer in Nigeria varies across different regions. A study conducted by the Nigerian National Cancer Control Program reported that the prevalence rate of breast cancer was higher in urban areas compared to rural areas, largely due to better diagnostic capabilities in urban centres [7] In Southeast Nigeria, studies have shown a significant lack of awareness about breast cancer symptoms, risk factors, and the importance of early detection [8]. This lack of awareness is a major barrier to early diagnosis and effective treatment.
Cultural beliefs and practices play a crucial role in the health-seeking behavior of women in Southeast Nigeria. Many women rely on traditional medicine and only seek medical attention when the disease has advanced significantly. Additionally, socioeconomic factors such as poverty, low educational levels, and lack of health insurance contribute to delays in seeking treatment [9]. Fear of stigmatization and the misconception that breast cancer is a death sentence also deter women from undergoing screening and seeking early medical intervention [7].
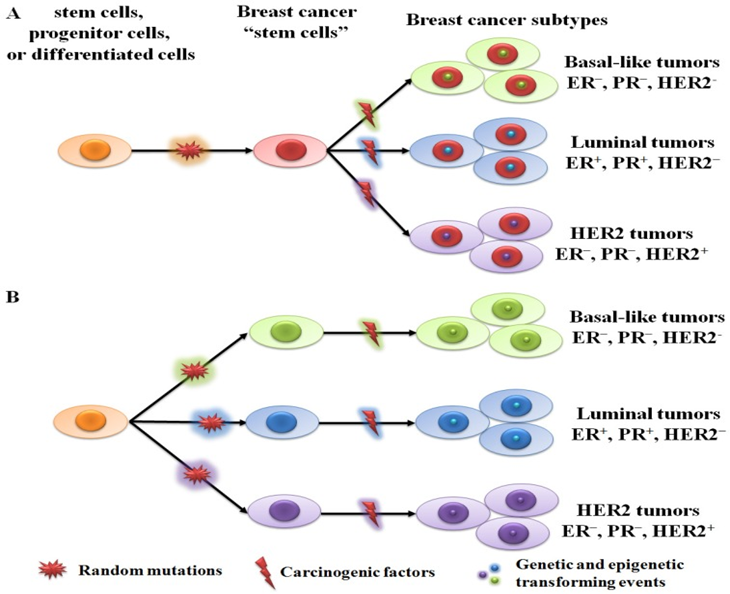
Figure 1: Two hypothetical theories of breast cancer initiation and progression [10].
(A) All subtypes of tumor are derived from the same stem cells or progenitor cells. Different tumor phenotypes are then determined by subtype-specific transforming events. (B) Each tumor subtype is initiated from a single cell type (stem cell, progenitor cell, or differentiated cell). Random mutations can gradually accumulate in any breast cells, leading to their transformation into tumor cells when an adequate number of mutations have accumulated [10].
Increasing awareness about breast cancer through education and community-based programs is essential to improving early detection rates in Southeast Nigeria. Studies have shown that awareness campaigns can significantly
enhance knowledge about breast cancer and encourage women to participate in regular screening practices [11]. Healthcare policies aimed at reducing the barriers to breast cancer screening and treatment, such as subsidizing the cost of mammograms and establishing more cancer care centres, are also crucial.
Study Design
A cross-sectional descriptive survey was conducted to assess the prevalence, awareness, and attitudes towards breast cancer among women in southeast Nigeria
Study Area
Southeast Nigeria, comprising states such as Abia, Anambra, Ebonyi, Enugu, and Imo, faces significant health challenges, including breast cancer. Breast cancer is a leading cause of morbidity and mortality among women in this region. Several factors contribute to this high burden, including limited access to healthcare facilities, lack of awareness about breast cancer symptoms, and cultural stigmas that delay diagnosis and treatment. Healthcare infrastructure in Southeast Nigeria is relatively underdeveloped, with many rural areas lacking adequate medical services. This results in late-stage presentations of breast cancer, which significantly reduces survival rates. Efforts to improve early detection through awareness campaigns and mobile screening units are vital. Additionally, addressing cultural barriers and educating women on the importance of regular breast self-examinations and seeking prompt medical attention can improve outcomes.
Population and Sampling
Target Population
The target population comprised women aged 18 years and above residing in Southeast Nigeria.
Sampling Method
A stratified sampling method was employed to ensure representation from both urban and rural areas within the southeast states. The steps involved were:
i.Selection of States: Three states were randomly selected from the five states in Southeast Nigeria.
ii.Selection of Local Government Areas (LGAs): Six LGAs were selected from each state, with an equal representation of urban and rural areas (three urban and three rural LGAs per state).
iii.Selection of Hospitals: Two general hospitals were randomly chosen from each LGA.
iv.Selection of Participants: From each hospital, ten participants were selected, resulting in a total sample size of 360 women.
Instrument
Data was collected using a structured questionnaire developed by the research team. The questionnaire was divided into different sections covering socio-demographic information, awareness of breast cancer, knowledge of breast cancer, medical history, as well as attitudes and practices towards breast cancer screening.
Procedure
Data Analysis
Data were analyzed using descriptive statistics such as frequencies and percentages to summarize the socio-demographic information, awareness of breast cancer, knowledge of breast cancer, medical history, as well as attitudes and practices towards breast cancer screening. Cross-tabulations were used to explore associations between the dependent and independent variables.
Ethical Considerations
Written informed consent was obtained from all participants before the interviews. Participant anonymity was ensured by assigning codes to the questionnaires and keeping all information confidential. The study protocol was approved by the relevant ethics committees in each of the selected states.
The socio-demographic profile of the 360 participants reveals that the majority are aged between 30 and 39 years (52.50%). Educationally, most participants have attained secondary education (58.89%), while a significant portion has tertiary education (29.17%). In terms of marital status, 84.17% are married. Employment status shows that 56.94% are self-employed, and half of the participants reside in rural areas, with the other half in urban areas (Table 1).
| Socio-Demographic Information | Frequency (n = 360) | Percentage (%) |
| Age (in Years) | ||
| Less than 20 | 19 | 5.28 |
| 20 – 29 | 86 | 23.89 |
| 30 – 39 | 189 | 52.50 |
| 40 and above | 66 | 18.33 |
| Educational Level | ||
| No formal Education | 11 | 3.06 |
| Primary Education | 32 | 8.89 |
| Secondary Education | 212 | 58.89 |
| Tertiary Education | 105 | 29.17 |
| Marital Status | ||
| Single | 36 | 10.00 |
| Married | 303 | 84.17 |
| Divorced/Widowed | 21 | 5.83 |
| Employment Status | ||
| Employed | 62 | 17.22 |
| Self-Employed | 205 | 56.94 |
| Unemployed | 93 | 25.83 |
| Retiree | 00 | 0.00 |
| Residence | ||
| Rural | 180 | 50.00 |
| Urban | 180 | 50.00 |
Table 1: Socio-Demographic Information of Participants
Regarding breast cancer awareness, an overwhelming 96.67% of participants have heard of breast cancer, with the primary sources of information being the internet and social media (43.51%) and healthcare professionals
(19.18%). Additionally, 36.67% know someone diagnosed with breast cancer (Table 2). The degree of awareness varies, with 39.72% having a good awareness level and 21.94% having a very good level (Figure 1).
| Variables | Frequency (n = 360) | Percentage (%) |
| Have you heard of breast cancer? | ||
| Yes | 348 | 96.67 |
| No | 12 | 3.33 |
| *If yes, where did you first hear about breast cancer? (Select all that apply) (n = 485) | ||
| Television/Radio | 83 | 17.11 |
| Newspaper/Magazines | 42 | 8.66 |
| Internet/Social Media | 211 | 43.51 |
| Healthcare professionals | 93 | 19.18 |
| Family/Friends | 42 | 8.66 |
| Community outreach programs | 11 | 2.27 |
| Others | 03 | 0.62 |
| Do you know anyone who has been diagnosed with breast cancer? | ||
| Yes | 132 | 36.67 |
| No | 228 | 63.33 |
* signifies multiple responses
Table 2: Awareness of Breast Cancer
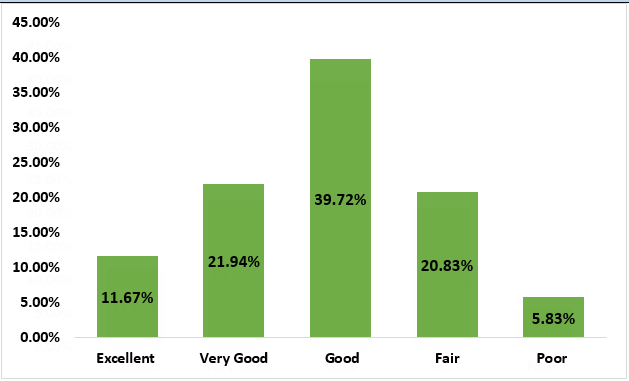
Figure 1: Degree of Awareness of Breast Cancer
Participants' knowledge about breast cancer shows that the most recognized risk factor is a family history of breast cancer (29.11%), followed by lifestyle
factors (23.77%). Common symptoms identified include pain in any area of the breast (25.06%) and lumps in the breast or underarm (22.99%). However,
self-assessed knowledge levels are modest, with 23.06% considering themselves somewhat knowledgeable and 24.44% not knowledgeable at all. Most participants (80.28%) recognize breast cancer as a serious health issue (Table 3).
| Variables | Frequency (n = 360) | Percentage (%) |
| *What do you think are the risk factors for breast cancer? (Select all that apply) (n = 711) | ||
| Family history of breast cancer | 207 | 29.11 |
| Age | 49 | 6.89 |
| Gender | 74 | 10.41 |
| Hormonal factors (e.g., early menstruation, late menopause) | 82 | 11.53 |
| Lifestyle factors (e.g., diet, alcohol consumption, smoking) | 169 | 23.77 |
| Radiation exposure | 76 | 10.69 |
| Lack of physical activity | 07 | 0.98 |
| Obesity | 42 | 5.91 |
| Others | 05 | 0.70 |
| *What are the common symptoms of breast cancer that you are aware of? (Select all that apply) (n = 1209) | ||
| Lump in the breast or underarm | 278 | 22.99 |
| Change in breast shape or size | 211 | 17.45 |
| Nipple discharge | 136 | 11.25 |
| Pain in any area of the breast | 303 | 25.06 |
| Skin changes on the breast | 258 | 21.34 |
| None | 00 | 0.00 |
| Other | 23 | 1.90 |
| How knowledgeable do you consider yourself about breast cancer? | ||
| Very knowledgeable | 51 | 14.17 |
| Somewhat knowledgeable | 83 | 23.06 |
| Neutral | 79 | 21.94 |
| Not very knowledgeable | 59 | 16.39 |
| Not knowledgeable at all | 88 | 24.44 |
| Do you believe breast cancer is a serious health issue? | ||
| Yes | 289 | 80.28 |
| No | 71 | 19.72 |
Table 3: Knowledge of Breast Cancer
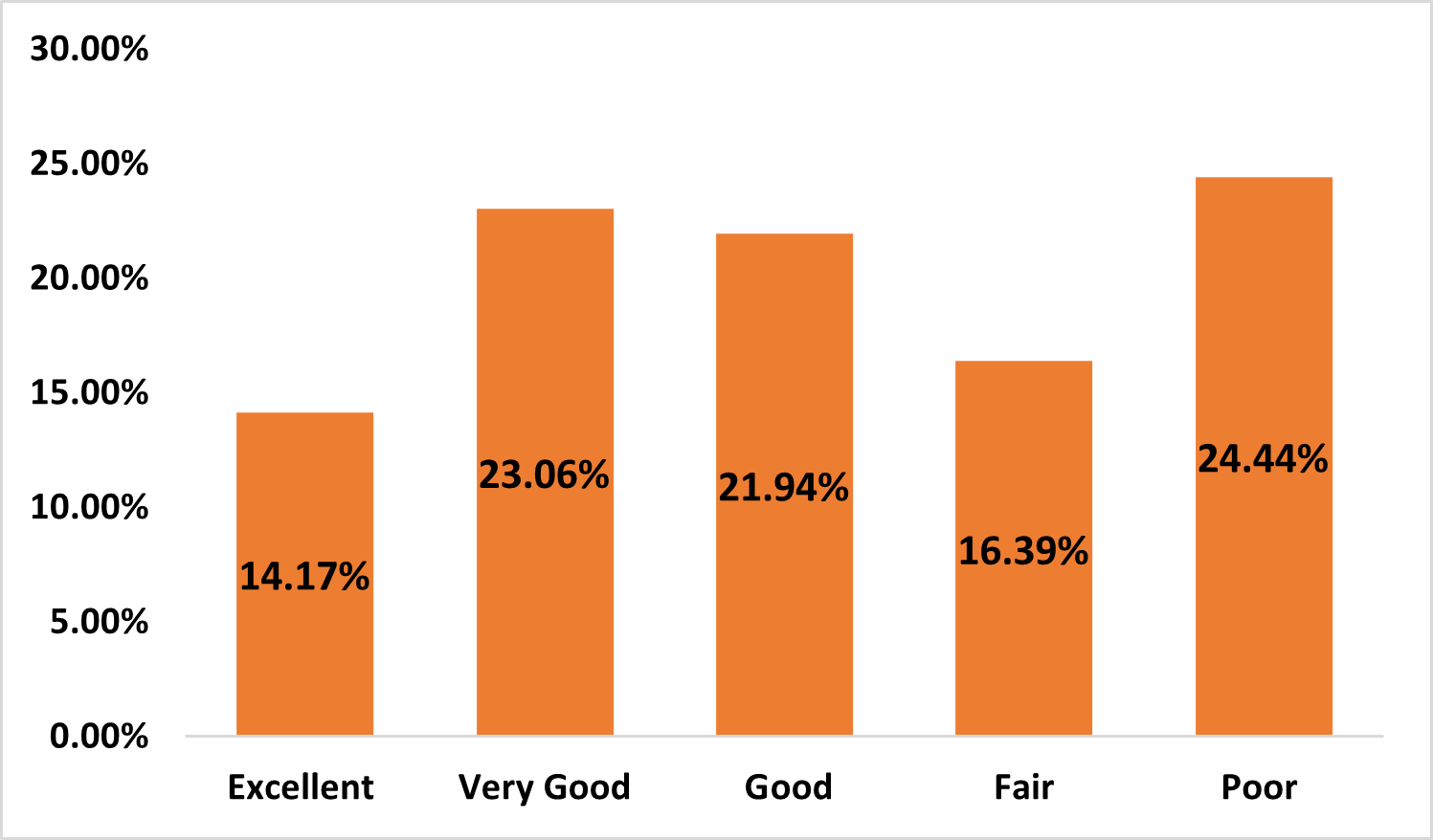
Figure 2: Degree of Knowledge of Breast Cancer
The medical history data indicates that 16.39% of participants have been diagnosed with breast cancer, primarily diagnosed between the ages of 50 and 59 (40.68%). Regular breast self-examinations are conducted by 30.28%, and 16.94% have a family history of breast cancer. Additionally, 69.72% have never had a clinical breast examination, and 91.11% have not had any other type of cancer (Table 4).
| Variables | Frequency (n = 360) | Percentage (%) |
| Have you ever been diagnosed with breast cancer? | ||
| Yes | 59 | 16.39 |
| No | 301 | 83.61 |
| If yes, at what age were you diagnosed? | ||
| Below 30 | 00 | 0.00 |
| 30-39 | 09 | 15.25 |
| 40-49 | 15 | 25.42 |
| 50-59 | 24 | 40.68 |
| 60 and above | 11 | 18.64 |
| Do you perform regular breast self-examinations? | ||
| Yes | 109 | 30.28 |
| No | 251 | 69.72 |
| How often do you undergo clinical breast examinations? | ||
| Annually | 33 | 9.17 |
| Every 2 years | 25 | 6.94 |
| Every 5 years | 51 | 14.17 |
| Never | 251 | 69.72 |
| Do you have a family history of breast cancer? | ||
| Yes | 61 | 16.94 |
| No | 299 | 83.06 |
| Have you ever had any other type of cancer? | ||
| Yes | 32 | 8.89 |
| No | 328 | 91.11 |
| *Do you have a history of any of the following conditions? (Check all that apply) (n = 363) | ||
| Diabetes | 44 | 12.12 |
| Hypertension | 59 | 16.25 |
| Obesity | 29 | 7.99 |
| None | 231 | 63.64 |
* Signifies multiple responses
Table 4: Medical History of Participants
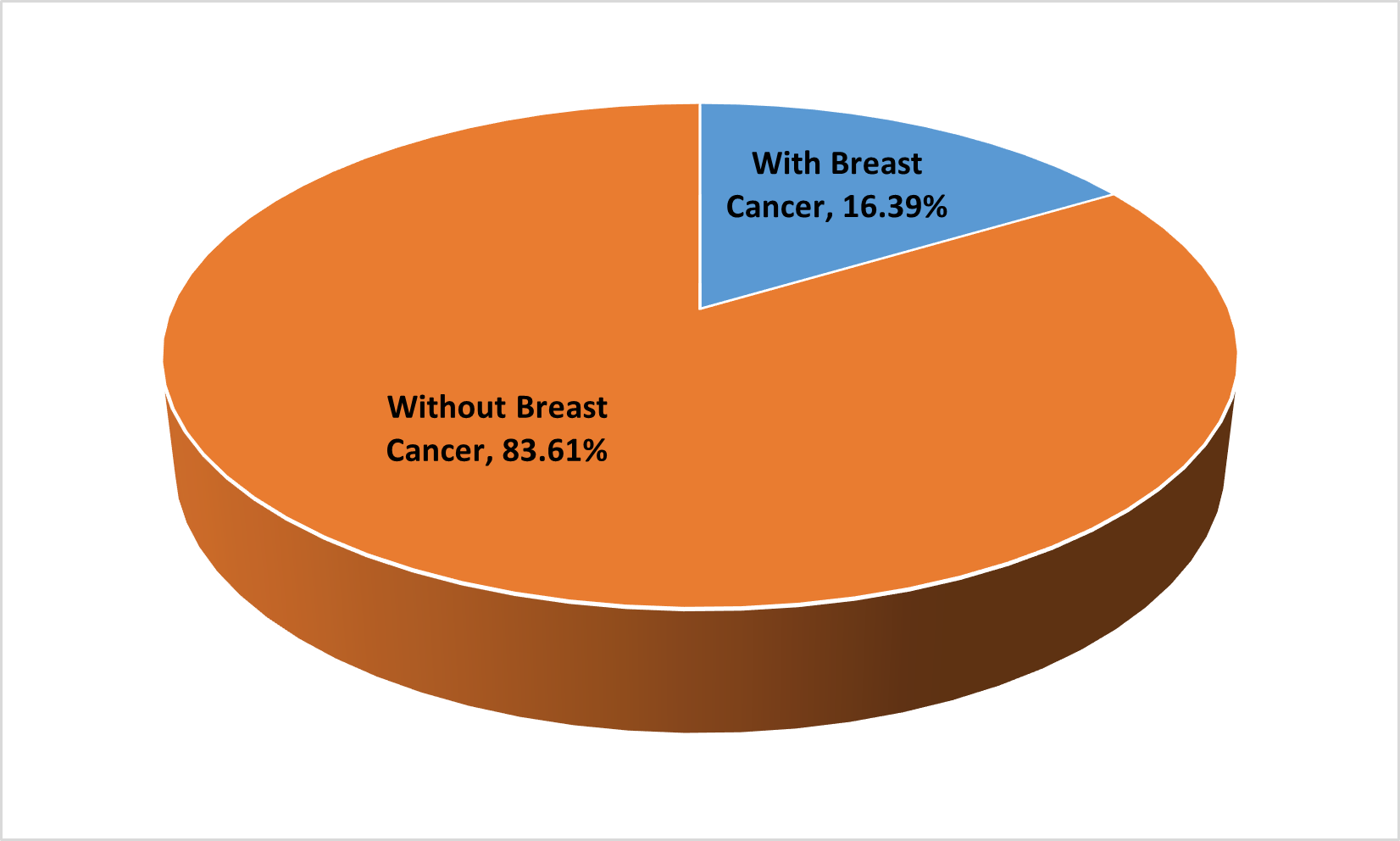
Figure 3: Prevalence and Awareness of Breast Cancer in Southeast Nigeria
Regarding attitudes and practices towards breast cancer screening, confidence in identifying symptoms is low, with 38.06% not confident and 49.72% unsure. However, 71.11% strongly agree that regular screening aids early detection, and 80
The results of this study indicate a high level of breast cancer awareness among women in Southeast Nigeria, with 96.67% of respondents having heard of the disease. This high awareness is consistent with findings from similar studies in other parts of Nigeria and sub-Saharan Africa. For instance, Agbo et al. [12] reported a comparable awareness level of 94.8% among women in Northern Nigeria, suggesting a widespread recognition of breast cancer across different regions of the country. The primary sources of information identified in this study were the Internet and social media (43.51%), followed by healthcare professionals (19.18%), and television/radio (17.11%). These findings reflect the growing influence of digital media in disseminating health information, a trend also observed in studies by Balogun et al. [13] and Akintola and Olubiyi [14].
The significant role of healthcare professionals as a source of information underscores the importance of medical practitioners in health education. This aligns with the findings of Akinola et al. [15], who emphasized the critical role of healthcare providers in improving health literacy and awareness. Conversely, the relatively lower impact of newspapers/magazines (8.66%) and community outreach programs (2.27%) suggests potential areas for targeted improvement, particularly in rural and underserved communities where digital access may be limited.
The study also revealed that 36.67% of respondents knew someone diagnosed with breast cancer. This personal connection to the disease could potentially enhance awareness and understanding, as suggested by the Health Belief Model, which posits that personal experiences and perceived susceptibility influence health behaviors [16]. The relatively high percentage of respondents with a personal connection to breast cancer in this study is higher than the 24% reported by Okobia et al. [11] in a study conducted in Edo State, Nigeria. This increase may reflect a growing incidence of breast cancer or improved diagnosis and reporting over the years.
When examining the degree of awareness, 39.72% of respondents rated their knowledge as good, while 21.94% rated it as very good, and 11.67% as excellent. These results are promising but also highlight room for improvement. Comparatively, a study by Bassey et al. [17] found that only 25% of women in Calabar, Nigeria, rated their awareness as good or better, indicating significant regional variations in the depth of knowledge about breast cancer.
The distribution of awareness levels in this study—with 20.83% rating their awareness as fair and 5.83% as poor—suggests that while initial recognition of breast cancer is high, detailed understanding and knowledge may be lacking for a substantial portion of the population. This is consistent with findings from a systematic review by Donnelly et al. [18], which highlighted that although general awareness of breast cancer is often high, specific knowledge about symptoms, risk factors, and early detection methods is frequently insufficient.
The findings of this study are consistent with the broader literature, which indicates high levels of awareness but varying degrees of detailed knowledge about breast cancer across different populations in Nigeria and sub-Saharan Africa. For instance, Okobia et al. [11] and Bassey et al. [17] both highlight the gap between general awareness and specific knowledge, a trend also observed in studies from other regions, such as East Africa [19] and South Africa [20].
The study identified that only 29.11% of the respondents recognized family history as a significant risk factor for breast cancer. This is relatively low compared to other studies in different regions. For instance, a study conducted in Lagos, Nigeria, found that about 48% of the participants acknowledged family history as a risk factor [7]. This disparity may indicate regional differences in health education or awareness programs.
Lifestyle factors such as diet, alcohol consumption, and smoking were identified by 23.77% of the participants as risk factors. This is slightly higher than the findings from a study in South Africa, where only 18% of women identified lifestyle factors as contributing to breast cancer [21]. The awareness of hormonal factors, including early menstruation and late menopause, was acknowledged by 11.53% of the participants, which is comparable to the 13% reported in a study in Kenya [22].
Interestingly, only 0.98% of the participants recognized lack of physical activity as a risk factor, a stark contrast to findings in developed countries where physical inactivity is well-documented and more commonly recognized by the public as a risk factor [23]. This suggests a need for targeted education on the importance of physical activity in reducing breast cancer risk in Southeast Nigeria.
Regarding symptoms, 25.06% of the respondents were aware that pain in the breast is a common symptom, while 22.99% identified lumps in the breast or underarms as a key symptom. These findings are lower compared to a study in Ghana where 35% of the women could identify lumps as a primary symptom of breast cancer [24]. The awareness of changes in breast shape or size was 17.45%, which is somewhat aligned with the findings in rural India, where approximately 20% of women recognised changes in breast shape as a symptom [25].
The high level of awareness about skin changes on the breast (21.34%) and nipple discharge (11.25%) aligns with previous studies that highlight these symptoms as less commonly known among women in developing countries [26].
The self-perceived knowledge about breast cancer among the respondents showed that only 14.17% considered themselves very knowledgeable, while 24.44
While awareness of breast cancer is high, there is a significant gap in regular screening practices and detailed knowledge. Interventions should focus on increasing practical knowledge and encouraging preventive practices through targeted awareness programs and improved healthcare access. Addressing cultural barriers, enhancing education on breast cancer prevention, and improving healthcare infrastructure are critical for reducing breast cancer morbidity and mortality in Southeast Nigeria.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
