
Research Article | DOI: https://doi.org/10.31579/2641-0419/161Copyright
*Corresponding Author: Fabricio Sarmento Vassallo, Electrophysiologist – Medical Coordinator of Electrophysiology in Instituto de Cardiologia do Espírito Santo and Santa Casa de Misericórdia Hospital
Citation: Fabricio Vassallo., Lucas L. Meigre., Eduardo Serpa., Betina Resck., Ariane Leal., et al., (2021) Prevalence and Resolution of Resistant Left Atrial Appendage Thrombus in Non-Valvular Atrial Fibrillation Patients Submitted to Percutaneous Interventions. J. Clinical Cardiology and Cardiovascular Interventions, 4(8); Doi:10.31579/2641-0419/161
Copyright: © 2021 Fabricio Sarmento Vassallo, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 March 2021 | Accepted: 08 April 2021 | Published: 15 April 2021
Keywords: left atrial appendage; left atrial appendage thrombus; atrial fibrillation; anticoagulation; transesophageal echocardiography; direct acting oral anticoagulants
ABSTRACT:
Introduction: Left atrial appendage (LAA) thrombus in atrial tachyarrhythmias is one of the principal causes of stroke. Prevalence and strategies to thrombus resolution has recently been described in the era of the direct oral anticoagulants (DOAC). The aim of the study was to determine the prevalence and strategies to resolve previous LAA thrombus during regular oral antithrombotic therapy in preparation to perform atrial fibrillation (AF) ablation and/or LAA closure.
Methods: Between January 2011 and December 2020 we prospectively followed 23 patients (5.39%) that showed LAA thrombus formation. Persistent AF occurred in 13 (56.52%), median age 72.39 years, 15 (65.22%) females, median CHA2DS2VASC of 4.13, HASBLED of 2.28, 17 (73.91%) with hypertension, (52.17%) with coronary disease, 9 (39.13%) had priors’ thromboembolic events, 7 (30.43%) with heart failure and Diabetes. Diagnosis was by transesophageal echocardiogram (TEE) in 20 (86.96%) and the rest by computed angiotomography. Rivaroxaban was used in 11 (47.83%), Dabigatran in 6 (26.09%), 5 (21.74%) with therapeutic range Warfarin and 1 (4.34%) with Apixaban. Main strategy of treatment was to change mechanism of action of antithrombotic medication in association to an antiplatelet drug, Clopidogrel 75mg a day, and perform a TEE at 90 days after.
Results: Complete resolution of the LAA thrombus was achieved in 18 (78.26%) patients in first medical therapeutic change. Of the remaining a second approach with medical therapy adjustment with off-label dose prescription associated with Clopidogrel showed complete resolution in 3 (13.04%) totalizing a success rate of 91.30% for all patients (p value of 0.001 for treatment success). The failure of the antithrombotic plus antiplatelet therapy occurred in 2 (8.7%) patients, one with LAA sludge and other with a huge thrombus in all LAA and part of left atrium.
Conclusion: Modification of the mechanism of action of direct oral anticoagulants in association with Clopidogrel demonstrates to be successful in a large number of patients with previous resistant left atrial thrombus with and secure since the low adverse event rates.
Atrial fibrillation (AF) predisposes to left atrial (LA) stasis and subsequent formation of left atrial appendage (LAA) thrombus, which can lead to cardioembolic stroke or systemic embolization1.
Direct current cardioversion or catheter ablation are usually performed in AF patients within a strategy rhythm control option, for symptoms relief and to rapidly restore sinus rhythm [1,2,3]. However, both cardioversion and catheter ablation, by inducing atrial stunning and endothelial damage, are associated with a not negligible risk of peri-procedural stroke or systemic embolism [4-7], being this risk maximal in the presence of left atrial appendage (LAA) thrombus8,9. For this reason, pre-procedural transesophageal echocardiography (TEE) is strongly recommended to screen for the presence of LAA thrombus [3,10,11]. Calkins et al. in current guidelines suggest that in patients with an AF duration of more than 48 hours or of unknown duration, three weeks of anticoagulation at a therapeutic level are needed before cardioversion or catheter ablation. However, in most cases, pre-procedural TEE and LA Computed Angiotomography is performed in all AF patients, despite an adequate anticoagulation and a not negligible incidence of LAT has been documented even among patients who have been therapeutically anticoagulated [12].
Although there is substantial evidence regarding efficacy of direct current oral anticoagulants (DOACs) for thromboembolic prophylaxis in patients with AF, efficacy of treatment in patients with pre-existing left atrial appendage thrombus is limited to a few case reports [13,14] and one registry of modest size in which rivaroxaban and dabigatran was utilized [15,16].
We aimed to determine the efficacy of the change in the mechanism of action of direct oral anticoagulants (DOACs) in association to antiplatelet therapy with clopidogrel in the resolution of resistant LAA thrombus utilizing transesophageal echocardiographic (TEE) and clinical outcomes.
Materials and Methods:
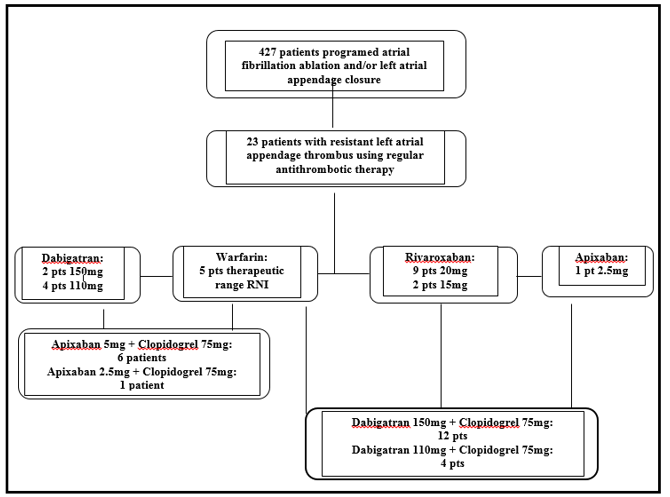
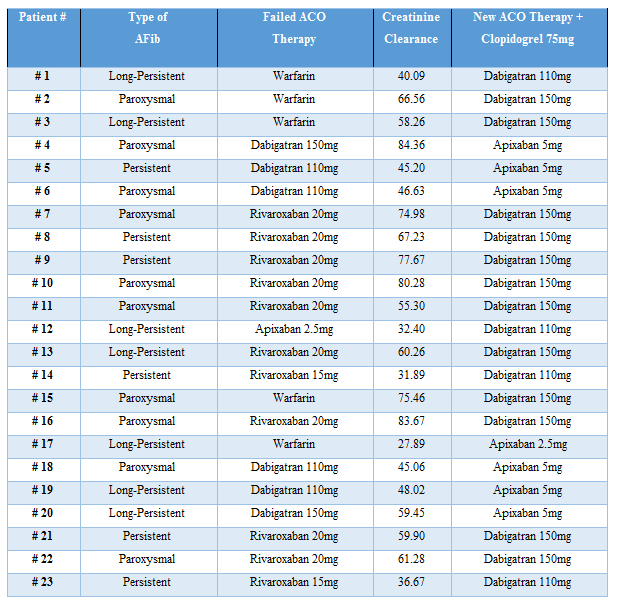
In the present study, 427 consecutive patients between January 2011 and December 2020 that were prepared for catheter ablation and/or LAA closure. The inclusion criteria was 23 patients (5.39%) that showed LAA thrombus formation resistant to regular use of adequate doses of anticoagulant therapy (Figure 1).
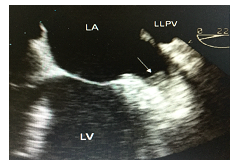
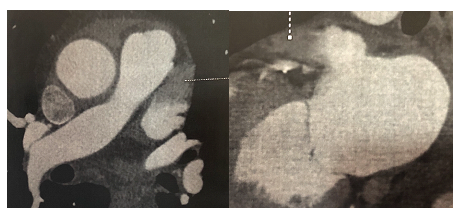
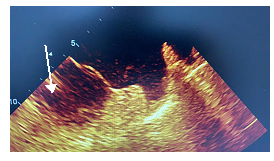
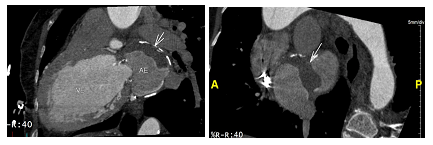
The diagnosis of LAA was made by transesophageal echocardiogram (TEE) in 20 (86.96%) patients and in 3 (13.04%) by computed angiotomography [17] (Figures 2,3 and 4). The examination of these patients was made by experienced physicians and were confirmed by a second physician thereafter.
The diagnosis of LAA was made by transesophageal echocardiogram (TEE) in 20 (86.96%) patients and in 3 (13.04%) by computed angiotomography17 (Figures 2,3 and 4). The examination of these patients was made by experienced physicians and were confirmed by a second physician thereafter.
Rivaroxaban was used in 11 (47.83%), followed by Dabigatran 6 (26.1%), therapeutic range warfarin presented in 5 (21.73%) cases and only 1 (4.34%) patient using Apixaban (Table 2).

Since the aim of the study was the complete resolution of a resistant LAA thrombus our strategy was to change the mechanism of action of the antithrombotic medication and associate empirically an antiplatelet, chosen one was clopidogrel 75mg, and repeat in 90 days thereafter a new TEE, that was performed and revised by the same operators. After the diagnosis of the LAA thrombus Dabigatran 150mg b.i.d. was prescribed in association to Clopidogrel 75mg for 12 (52.17%) patients, Dabigatran 110mg b.i.d. plus Clopidogrel 75mg for 4 (17.39%) patients, Apixaban 5mg b.i.d. in association to Clopidogrel 75mg in 6 (26.09%) and Apixaban 2.5mg b.i.d. plus Clopidogrel 75mg for 1 (4.35%) patient (Table 3).
Statistical analysis:
All tests were performed using BioStat statistical software (AnalystSoft Walnut, CA, USA). Continuous variables were expressed as mean-standard deviation. A result was considered significant if P value of < .05.
Results:
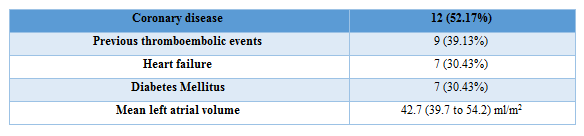
Between the 23 patients, persistent AF was present in 13 (56.52%) patients, median age 66.08 (62 to 83) years, 15 (65.22%) of females, median CHA2DS2VASC of 3.77 (2 to 7), HASBLED of 2.28 (1 to 5), 17 (73.91%) with hypertension, (52.17%) with coronary disease, 9 (39.13%) had previous thromboembolic events, 7 (30.43%) with heart failure and 7 (30.43%) Diabetes Mellitus (Table 1).
After a 90-days new antithrombotic plus antiplatelet regimen we achieved a complete resolution of the LAA thrombus in a total of 18 (78.26%) patients. Of the remaining 5 (21.74%) patients a second attempt with medical therapy adjustment to a higher dose off-label prescription of the same DOAC with maintenance of Clopidogrel showed complete resolution in 3 (60%) of these 5 patients, determining a total success rate of 91.30% (p value of 0.001). All of these 5 patients, 4 (80%) were using Dabigatran 110mg b.i.d. and 1 (20%) using Apixaban b.i.d. 2.5mg, both adjusted dosages because of the renal impairment. The failure of the antithrombotic plus antiplatelet therapy occurred in two patients, one with the use of Apixaban who showed a partial resolution of the LAA thrombus but remained with a sludge (Figure 5) inside the LAA and other using Dabigatran which remained with a huge thrombus in all LAA and part of left atrium (Figures 6 and 7).

In these patients submitted to an off-label prescription we observed minor bleeding in 2 such as gingival or nasal spontaneous bleeding and major bleeding such as gastrointestinal and large subcutaneous hemorrhages that not required hospital admission in 3 patients.
The clinical characteristics of the patients are as followed; ≥ 71 years, all with persistent and long-persistent atrial fibrillation, CHA2DS2VASC ≥ 4; left atrial volume of ≥ 47ml/m2, the creatinine clearance was ≤ 40ml/min, rest heart rate observed commonly was ≥ 85bpm, 4 (80%) patients had heart failure with left ventricular ejection fraction of ≤45% and 4 (80%) were female gender.
Atrial fibrillation is commonly associated with formation of left atrial appendage (LAA) thrombus which can lead to thromboembolic events. Traditionally, warfarin has been the primary anticoagulant used for patients with AF [18]. In 2009, the RE-LY trial in patients with AF showed that dabigatran reduced stroke risk in patients with atrial fibrillation without increasing the risk of major bleeding as compared to warfarin [19]. In 2011, the ROCKET-AF trial demonstrated that rivaroxaban was non-inferior to warfarin in preventing stroke or another systemic thromboembolism in a similar patient population [20]. Also, in 2011, the ARISTOTLE trial showed that apixaban was associated with a lower incidence of stroke and/or thromboembolism, and a decrease in the incidence of bleeding, as compared to traditional anticoagulation therapy with warfarin in patients with atrial fibrillation [21,22]. Although these studies demonstrated efficacy in thromboembolic prophylaxis in patients with AF [23], there is limited data regarding use of these agents to treat patients with pre-existing LAA thrombus [24-26].
Complete LA thrombus resolution is mandatory prior to performing procedures within the LA, such as catheter ablation for AF and LA appendage occlusion [27]. Reasonable confidence in LA thrombus resolution rates would provide guidance as to the optimal time to reschedule procedures.
DOACs have become common in clinical practice for thromboembolic prophylaxis in nonvalvular, and recently in patients with AF and biological valves [28], AF following several landmarks randomized controlled trials that demonstrated noninferiority to warfarin [29]. Nevertheless, there is uncertainty regarding the application of these results for the management of LA thrombus. To the best of our knowledge, there have been only five publications on NOACs to date where all or the majority of subjects with AF or flutter were oral anticoagulant (OAC) naïve at the time of initial diagnosis of LA thrombus [26,30-33].
Hao et al [30] reported intracardiac thrombus resolution by TEE in 19 of 22 (89.5%) subjects after three months of treatment with dabigatran 150 mg b.i.d. This prospective study, performed at Qilu Hospital of Shandong University, was notable for having a warfarin comparison group with resolution in 17 of 22 (77.3%) subjects. However, prior OAC use was present in three subjects in the dabigatran group and eight subjects in the warfarin arm.
Lip et al [26] conducted the Xarelto–ThRombus Accelerated resolution (X-TRA) multicenter prospective study throughout seven countries.20 Rivaroxaban dosage was 20 mg b.i.d., or 15 mg b.i.d. in the case of renal impairment. The LA thrombus resolution rate was only 41.5% (95% CI, 28.1%–55.9%) in 60 subjects after mean treatment duration of 46 days. Of these subjects, 23.3% had prior OAC use. Results from the rivaroxaban treatment group were compared to 156 patients from a multicenter retrospective registry who were treated with five different VKA agents. Two important limitations included different time periods of patient recruitment and marked differences in baseline characteristics between treatment groups.
Xing et al administered dabigatran 150 mg q.d. to subjects with nonrheumatic AF and LA thrombi confined to the appendage who presented to General Hospital of Shenyang Military Command of PLA [31]. TEE was performed after 3 months of DOAC treatment. In 58 subjects, complete LA appendage thrombus resolution was observed in only 15 (25.9%). Lack of prior long-term OAC use at the time of initial LA thrombus diagnosis was not explicitly reported.
Fleddermann et al reported a retrospective cohort study from St. Luke’s Mid America Heart Institute in 16 patients with AF who were treated with NOACs for LA appendage thrombus [32]. None of the patients received OAC agents prior to the index medical encounter. Complete resolution was demonstrated in 9 of 9 (100%) patients who received apixaban, 4 of 4 (100%) patients who received dabigatran, and 2 of 3 (67%) patients who received rivaroxaban. The median time between initial and follow-up TEEs was 66 days (range, 33 to 2000 days). TEEs were reviewed by a cardiologist blinded to the OAC agents received.
Ke et al conducted a randomized controlled trial of rivaroxaban 20 mg q.d. versus warfarin for LA thrombus detected on TEE in 80 subjects who were scheduled for catheter ablation for nonvalvular AF at The First Affiliated Hospital of Guangxi Medical University [33]. All subjects were free of OAC for one month prior to LA thrombus diagnosis and 80% were confined to the LA appendage. Repeat TEEs were performed at 6 weeks and 12 weeks. At 6 weeks, complete LA thrombus resolution was observed in six (15%) subjects in the rivaroxaban group and 0 (0%) subjects in the warfarin group (P = .01). At 12 weeks, complete resolution was observed in 32 (80%) subjects in the rivaroxaban group and 28 (70%) subjects in the warfarin group (P = .30).
Ultimately, multicenter randomized controlled trials to compare individual DOACs to warfarin or other DOACs should be performed.
The REsolution of Left atrial-Appendage Thrombus–Effects of Dabigatran [34] in patients with Atrial Fibrillation (RE-LATED AF) study was designed to randomize 110 subjects with nonvalvular AF and LA appendage thrombus diagnosed on TEE to dabigatran versus the VKA phenprocoumon34. Follow-up TEE will be performed after at least 3 weeks and up to a maximum of 6 weeks after the initial TEE. Patients with LA appendage thrombus that formed while receiving >3 months of a VKA will be excluded from enrollment.
From our knowledge this is the first report of a strategy in patients with previous and resistant LAA thrombus for the complete resolution of the issue. The empirical use of an antiplatelet drug such as Clopidogrel associated to a DOAC and in some cases the prescription of an off-label dosage of these medications can explain the high success rate of the manuscript.
A series of limitations must be addressed in the present study.
First this is an observational, small sample sized study with retrospective analysis. Second it was a non-randomized and with no control group. Third the lack of the LA appendage emptying speed and thrombus size weight in the fact that these two features may impact in thrombus resolution.
In the present study when we performed the modification of vitamin-K antagonists to direct oral anticoagulants and change the mechanism of action of these drugs in association to an antiplatelet thienopyridine derivate demonstrates to be a successful strategy in a large number of patients with previous resistant left atrial thrombus and secure since the low adverse event rates.
For their dedication and effort in data collection and patience, we appreciate the dedication of Christiane Amaral and Vanessa Rodrigues from the administration staff and Edevaldo da Silva, Rafael Zeni and Anderson Barcelos from the biomedical team.
Financial support: This study had no source of financial support.
All authors declare no conflicts of interest.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
