
Research Article | DOI: https://doi.org/10.31579/2578-8965/042
*Corresponding Author: Martin Mumuni Danaah Malick, University for Development Studies, School of Medicine and Health Sciences, Department of Pharmacy
Citation: Danaah Malick M M, Maaleku A, Rivera O. (2020) Prevalence and factors associated with anemia in pregnancy among women receiving antenatal care at the West Gonja District Hospital of Northern Ghana. J Obstetrics Gynecology and Reproductive Sciences, 4(3): DOI: 10.31579/2578-8965/042
Copyright: © 2020. Martin Mumuni Danaah Malick. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 20 June 2020 | Accepted: 20 July 2020 | Published: 14 September 2020
Keywords: prevalence; anemia in pregnancy; risk factors; socio demographics; nutritional status
Background:
Anemia in pregnancy is a major public health problem especially in Low and Middle-income countries (LMIC) including Ghana and is defined by the World Health Organization (WHO) as being present when the hemoglobin concentration in the peripheral blood is 11g/dl or less. In most African countries anemia in pregnancy occurs if the hemoglobin concentration falls below 10g/dl. Pregnant women are at a higher risk of developing anemia due to several factors such as hemodilution, nutritional factors, multiple gestation, socio-economic status and malaria infestation. Anemia in pregnancy is an important cause of maternal mortality and affects half of pregnant women worldwide; with 56% of West African pregnant women being anemic. The objective of this study is to assess the prevalence and identify the risk factors associated with anemia among pregnant women receiving antenatal care at the West Gonja Hospital (WGH)
Methods: A cross-sectional was conducted with 136 pregnant women receiving antenatal care at the WGH between January 2017 to February 2018. Random sampling was used to select participants and data was collected using a structured questionnaire. Data was analyzed using the SPSS Version 24.0.
Results: A total 71(52.2%) of the study population were anemic, while 65 (47.8%) were not anemic. 20(74.1%) of the 27 pregnant housewives were anemic, while 11(64.7%) of the pregnant farmers were anemic. 27 (96.4%) of the 28 pregnant women who took their iron/folate supplement only some few days were anemic. 12 (100%) of the 12 participants who took their iron/folate supplement a few times a week were anemic. 4 (80%) of the 5 participants who never took their iron/folate supplement were anemic. 21 (70%) of those who did not sleep under ITN were anemic. 33 (84.6%) of the 39 patients who were diagnosed with malaria were also anemic. 28 (87.5%) of the 32 participants who took only 2 meals a day were anemic. 27 (79.4%) of the 34 patients who took liver, beef, chicken and fish only twice weekly were anemic. 15 (88.2%) of the 17 patients who drank tea some days in a week were anemic.
Conclusion: Although most of the pregnant women were adequately educated on the most relevant aspects of anemia in pregnancy, more than half of them were still anemic. Anemia was more prevalent among pregnant uneducated housewives with poor nutritional habits. All the pregnant sickle cell disease patients as well as those diagnosed with malaria were also anemic.
Anemia is defined as a decrease in the oxygen carrying capacity of blood due to a decrease in blood volume, a decrease in the total number of red blood cells, a decreased concentration of hemoglobin or a combination of any of the three. The World Health Organization (WHO) defines anemia in pregnancy as being present when the hemoglobin concentration in the peripheral blood is 11g/dl or less [1]. In most African countries anemia in pregnancy occurs if the hemoglobin concentration falls below 10g/dl [2]. Pregnant women are generally at an increased risk of developing anemia due to scientifically determined factors such as nutritional status, grand multiparity, multiple gestation, low socio-economic status, inadequate child spacing, chronic blood loss, hookworm infestation, hemoglobinopathies, malaria infestation and hemodilution [3]
The symptoms of anemia are usually non-specific and vague but generally include fatigue, weakness, dizziness, breathlessness, headache, and when severe enough, there may be hypotension, dyspnea, palpitations, lethargy and paresthesia [4]. Although Anemia is a condition that can be easily prevented, it constitute a major cause of mortality and morbidity among pregnant women; and accounts for about 20% of maternal deaths worldwide [5].
About 24.8% of the world population is affected by anemia representing 1.62 billion people [6]. Anemia in pregnancy is a major public health problem especially in Low and Middle-Income Countries such as Ghana; and It has been estimated that 41.8% of pregnant women worldwide are anemic. In developing countries, the prevalence of anemia in pregnancy is 60.0% of which about 7.0% of these women are severely anemic [7]. In Africa 57.1% of pregnant women are anemic [8]. Sub-Saharan Africa is the most affected region, with prevalence of anemia estimated to be 17.2 million among pregnant women, which is about 30% of total global cases [9].
Despite the fact that the Government of Ghana through the Ghana Health Services has implemented several policies and interventions to reduce the prevalence of Anemia in Pregnancy; the country still has a prevalence rate of about 62.4%, with higher prevalence rates being recorded in the rural areas [10]. To the best knowledge of the researchers, the prevalence of anemia in pregnancy specific for West Gonja District of the Savannah Region of Ghana has not yet been studied. The purpose of this study was to determine the prevalence and identify the risk factors associated with anemia in pregnancy in the West Gonja District
This was a cross-sectional study conducted with 136 pregnant women receiving antenatal care at the west gonja District hospital between 28th January 2018 to 15th February, 2019. Study participants were randomly selected as they were waiting to receive care at the antenatal care unit. To avoid data duplication, a unique code was assigned to each study and recorded on the questionnaire to help identify them. An interview was conducted using a structured questionnaire to obtain data about the socio-demographic characteristics, obstetric history, antenatal visits, iron and folic acid supplementation, health conditions during the pregnancy, nutritional assessment and finally, knowledge of anemia assessed by the mother’s ability to correctly name at least one symptom, two causes, and two preventive measures of anemia. Hemoglobin levels were obtained from their antenatal records. Data was analyzed through the IBM Statistical Package for Social Sciences(SPSS) version 24.0 to obtain frequencies and cross tables for all relevant Variables. Univariate and multivariate analysis were used to explore associations between the individual factors (independent variables) and the outcome variable. Chi square was used as the statistical test to test associations between the independent variables and the outcome variables using regression analysis. Each study participant gave their written informed consent to participate in the study and were assured of full confidentiality with their personal health related information. Written Permission to conduct the study was fully granted by the hospital management team and since the study did not involve any medical intervention nor did it pose any health risk on respondents, there was no need for an ethical clearance from the district health directorate.
Inclusion and Exclusion Criteria
Only pregnant women who had evidence of recently (during the study period) determined hemoglobin level documented and were compliant with their scheduled antenatal care appointments (based on details from their antenatal records); were included in this study. Pregnant women who were not compliant with their scheduled antenatal care appointments as well as those who were being prepared for labor and delivery were all excluded from the study.
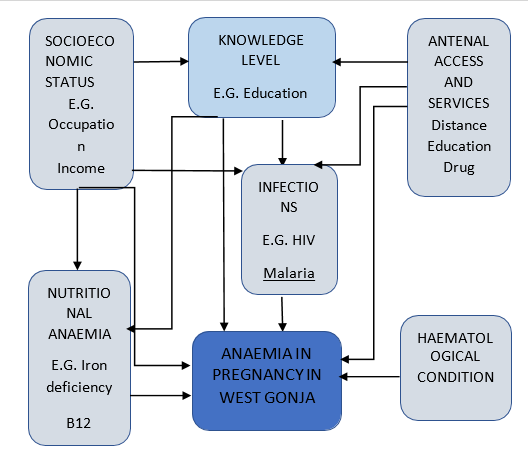
Figure. 1: Conceptual Framework
1.0: Socio-demographic characteristics of study participants.
The mean age range of the 136 respondents was 24-28, 41(30%) and closely followed by 19-23, 38(29%), with both age ranges representing more than 50% of the distribution. Only 8 (5%) were 18 years and below, and 49 (35%) were above 28 years. Most, 108 (79%) of the expectant mothers were married while the remaining 28 (21%) were single. 39 (29%) of the respondents were traders and 9(7%) were government workers. 69 (51%) of respondents were Christians while 67 (49%) were of the Islamic faith. 57 (41%) attained primary education, 29 (21.32%) had no education, 8 (5.88%) attained vocational training, 23 (16.91%) were secondary school graduates while 19(13.97%) completed tertiary education secondary and tertiary education (Table. 1)
| Variable | Frequency | Percentage (%) | ||
| Age Group |
Less thanor Equal to 18 |
8 |
5.88 | |
| 19-23 | 38 | 27.94 | ||
| 24-28 | 41 | 30.15 | ||
| 29-33 | 26 | 19.12 | ||
| 34-38 | 14 | 10.29 | ||
| Greater than 39 | 9 | 6.62 | ||
| Marital Status | ||||
| Single | 28 | 20.59 | ||
| Married | 108 | 79.41 | ||
Occupational Status Trader |
39 |
28.68 | ||
| Housewife | 27 | 19.85 | ||
| Farmer | 17 | 12.50 | ||
| Government worker | 9 | 6.62 | ||
| Others | 44 | 32.35 | ||
| Religion | ||||
| Christian | 69 | 50.74 | ||
Muslim Educational Status | 67 | 49.26 | ||
| None | 29 | 21.32 | ||
| Primary | 57 | 41.91 | ||
| Secondary | 23 | 16.91 | ||
| Vocational | 8 | 5.88 | ||
| Tertiary | 19 | 13.97 | ||
| Total | 136 | 100.00 | ||
Table. 1.0: Socio-demographic characteristics of study participants.
1.1: Obstetric and Antenatal background of study participants
43 (31.6%)of expectant mothers were primigravida whiles 93 (68.30%) were multigravida. 48 (35.5%) respondents were nulliparous. 88 (64.7%) respondents were multiparous of which only 3 (2.1%) had more than four deliveries past 28 weeks. 62 (45.6%) study participants had their youngest child two years ago or more while 24 (17.6%) had the youngest child less than two years of age. The rest, 50 (36.8%) were either nulliparous or had lost their child during their neonatal period. 65 (47.8%) were in their second (2nd) trimester, 36 (26.5%) in their third (3rd) trimester, and 35(25.7%) in their first (1st) trimester at the time of data collection. 99 (72.8%) had their first antenatal visit in their first (1st) trimester, 36 (26.5%) in their second (2nd) trimester and 0.7% (1) in their third (3rd) trimester. 38 (27.9%) had never had any prior antenatal visit. 3 (2.1) had more than 4 antenatal visits while 8 (5.9%) had four (4) antenatal visits. 91 (66.9%) were currently on iron/folate tablets supplementation, 45(33.1%) were not on any supplementation tablets. Of the 91 taking the iron/folate tablets supplementation, 69 (75.82%) started in their first (1st) trimester, 21(23.07%) in their second (2nd) trimester and only 1(1.1%) started in her third (3rd) trimester. In terms of compliance with iron/folate supplementation, 52 (38.2%) took twice daily, 39 (28.7%) had not yet taken and 5 (3.7%) had never taken though they have had more than one antenatal visit (Table. 1.1)
| Variable | Frequency | Percentage (%) | |||
| Gravidity | |||||
| One (1) | 43 | 31.6 | |||
| Two (2) | 29 | 21.3 | |||
| Three (3) | 29 | 21.3 |
| Four (4) | 17 | 12.5 | |||
| Greater than Four (>4) | 18 | 13.2 | |||
| Variable | Frequency | Percentage (%) | |||
| Parity | |||||
| None | 48 | 35.3 | |||
| One (1) | 33 | 24.3 | |||
| Two (2) | 22 | 16.2 | |||
| Three (3) | 17 | 12.5 | |||
| Four (4) | 13 | 9.6 | |||
| Greater than Four (>4) | 3 | 2.1 | |||
| Age of Youngest Child | |||||
| Less than Two(<2> | 24 | 17.6 | |||
| Greater or equal to Two (≥2) | 62 | 45.6 | |||
| None | 50 | 36.8 | |||
| Current Gestational Age | |||||
| 1stTrimester | 35 | 25.7 | |||
| 2ndTrimester | 65 | 47.8 | |||
| 3rd Trimester | 36 | 26.5 | |||
| Gestational Age at 1st ANCvisit | |||||
| 1st Trimester | 99 | 72.8 | |||
| 2nd Trimester | 36 | 26.5 | |||
| 3rd Trimester | 1 | 0.7 | |||
| Number of Antenatal visits | |||||
| None | 38 | 27.9 | |||
| One (1) | 34 | 25 | |||
| Two (2) | 13 | 9.6 | |||
| Three (3) | 13 | 9.6 | |||
| Four (4) | 8 | 5.9 | |||
| Greater or equal to five (≥5) | 30 | 22 | |||
| Are you Currently on Iron/Folate Tablets | |||||
| Yes | 91 | 66.9 | |||
| No | 45 | 33.1 | |||
| When did you start taking them | |||||
| 1st Trimester | 69 | 50.7 | |||
| 2nd Trimester | 21 | 15.4 | |||
| 3rd Trimester | 1 | 0.7 | |||
| None | 45 | 33.1 | |||
| How many do you take in a week | |||||
| Twice Everyday | 52 | 38.2 | |||
| Some days | 28 | 20.6 | |||
| Few times a week | 12 | 8.8 | |||
| Never | 5 | 3.7 | |||
| Not yet | 39 | 28.7 | |||
| Total | 136 | 100 | |||
Table. 1.1: Obstetric and Antenatal background of study participants
1.2: Health and Nutritional background of study participants
106 (77.9%) out of the 136 study participants sleep under insecticide treated nets and 30 (22.1%) do not sleep under insecticide treated nets. 39 (28.7%) were diagnosed with malaria in the past six (6) months while 97 (71.3%) did not suffer from any malarial infection. only 2 (1.5%) out of the 136 study participants were sickle cell disease positive while 134 (98.5%) were negative. 78 (57.4%) had averagely three meals a day, 32 (23.5%) averagely had 2 meals a day and 26 (19.1%) had averagely more than three (>3) meals a day. For the weekly intake of heme containing foods such as liver, beef, etc., 56 (41%) had averagely three (3) times per week, 42 (30.9%) had more than three (>3) times per week and Only 4 (2.9%) had the heme containing foods once a week. Regarding the weekly intake of non-heme containing foods such as beans, nuts etc., 65 (47.8%) had about three (3) times per week, 51 (37.5%) had more than three (>3) times per week and 4 (2.9%) had the non-heme containing foods only once a week. 77 (56.6%) did not consume tea weekly while pregnant, 40 (29.4%) consumed it a few days a week (about <3>(Table. 1.2)
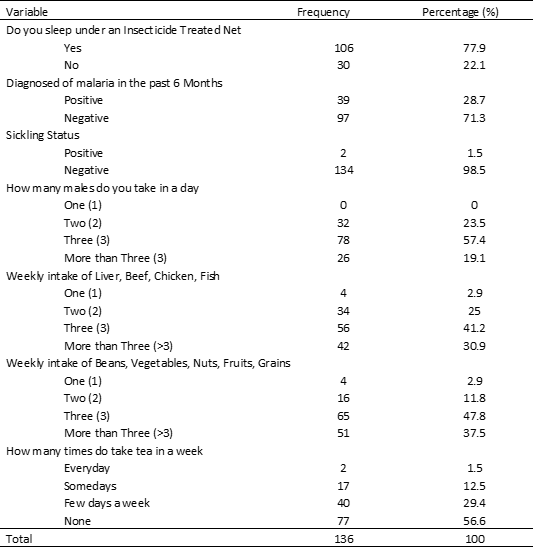
Table. 1.2: Health and Nutritional background of study participants
1.3: Hemoglobin Concentration of Study Participants
65 (47.8%) of all respondents presented with normal Hemoglobin (Hb) of ≥11.0 g/dl, 42 (30.9%) respondents had mild anemia with Hb of 10.0-10.9 g/dl, 27 (19.9%) were moderately anemic with Hb of 7.0-9.9 g/dl and only 2 (1.5%) had severe anemia Hb of <7>Table. 1.3 /Figure.1)
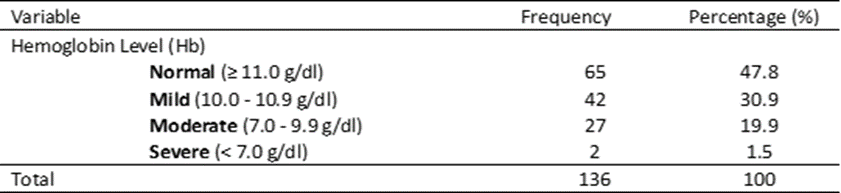
Table. 1.3: Hemoglobin Concentration of Study Participants

Figure. 1: Hemoglobin Concentration of Study Participants
1.4: Anemia Prevalence among Study Participants
The overall prevalence of anemia within the sampled study population was 71 (52.2%) as shown in (Table. 1.4/Figure. 2)

Table. 1.4: Anemia Prevalence among Study Participants
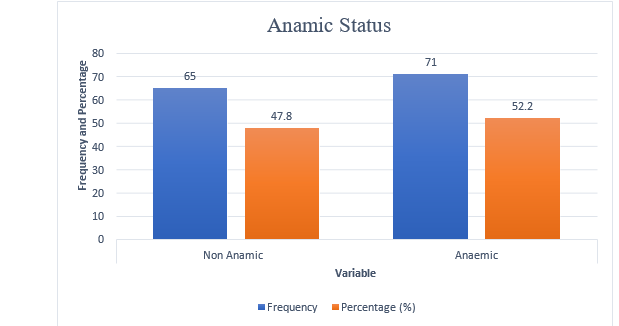
Figure. 2: Anemia Prevalence among Study Participants
1.5: Distribution of Knowledge Level on Anemia in Pregnancy among Study Participants
The majority 94 (69.1%) of respondents had ever been educated about anemia in pregnancy while 42 (30.9%) had never been educated. Of the 94 respondents who had been educated on anemia, a significant number, 69 (50.7%) were educated at the ANC unit, 12 (8.8%) through the media, 6 (4.4%) were educated by friends and family while others where educated from other sources. Concerning knowledge level of respondents on the signs/symptoms of anemia in pregnancy, 88 (64.7%) scored poorly, 44 (32.4%) scored fairly and 4 (2.9%) scored very well.
Regarding knowledge level of respondents on the causes/ risk factors of anemia in pregnancy, majority, 74 (54.4%) scored poorly, 49 (36%) scored fairly and 13 (9.6%) scored very well. In the area of knowledge level of respondents on the preventive measures of anemia in pregnancy, 67 (49.3%) scored poorly, 39 (28.7%) scored very well and 30 (22.1%) scored fairly. (Table 1.5/Figure. 3)
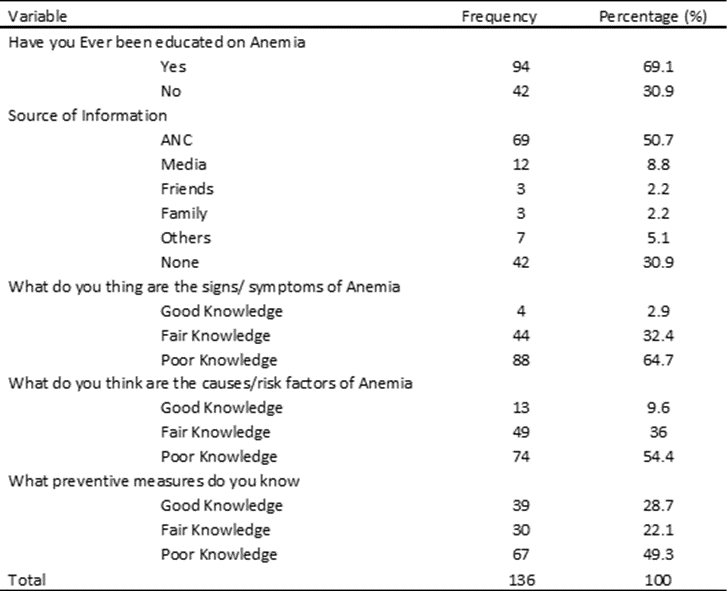
Table. 1.5: Distribution of Knowledge Level on Anemia in Pregnancy among Study Participants
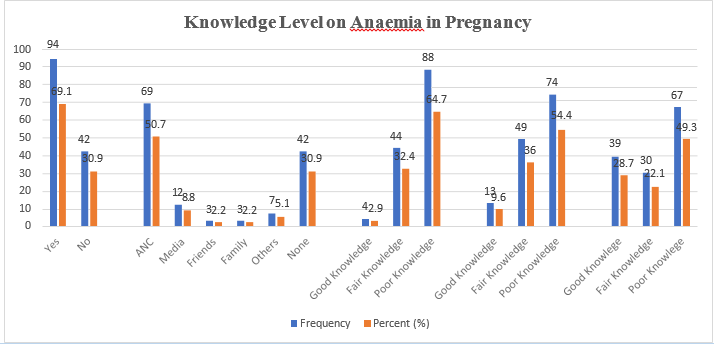
Figure. 3: Distribution of Knowledge Level on Anemia in Pregnancy among Study Participants
1.6: Distribution of Anemia by Knowledge Level about Anemia in Pregnancy.
A Chi-Square Test of independence was run to determine whether there is an association between the anemic status of the study participants and some variables assessing the knowledge level on anemia. With a chosen significance level of 0.05, if the p-value is less than 0.05 then the association between the two variables is statistically significant hence the null hypothesis is accepted. If the p-value is greater than 0.05 then there is no association between the two variables hence the null hypothesis is rejected. (Table. 1.6)
| Variable | anemic Status | Total | Chi-Squad, x², P- Value | |
| Non-anemic | anemic | |||
| Have you Ever been educated on Anemia | 16.929, 1, <0.001 | |||
| Yes 56 (59.6%) | 38 (40.4%) | 94 | ||
| No 9 (21.4%) | 33 (78.6%) | 42 | ||
| Source of Information | 20.807, 5, <0.001 | |||
| ANC 39 (56.5%) | 30 (43.5%) | 69 | ||
| Media 10 (83,3%) | 2 (16.7%) | 12 | ||
| Friends 1 (33.3%) | 2 (66.7%) | 3 | ||
| Family 2 (66.7%) | 1 (33.3%) | 3 | ||
| Others 4 (57.1%) | 3 (42.9%) | 7 | ||
| None 9 (21.4%) | 33 (78.6%) | 42 | ||
| What do you thing are the signs/ symptoms of Anemia | 26.423, 2, <0.001 | |||
| Good Knowledge 4 (100%)0 0 (0.0%) | 4 | |||
| Fair Knowledge 33 (75.0%) 11 (25.0%) | 44 | |||
| Poor Knowledge 28 (31.8%) 60 (68.2%) | 88 | |||
| What do you think are the causes/ risk factors of Anemia | 36.120, 2, <0.001 | |||
| Good Knowledge 9 (69.2%) 4 (30.8%) | 13 | |||
| Fair Knowledge 38 (77.6%) 11 (22.4%) | 49 | |||
| Poor Knowledge 18 (24.3%) 56 (75.7%) | 74 | |||
| What preventive measures do you | 37.46, 2, <0.001 | |||
| Good Knowledge 32 (82.1%) | 7 (17.9%) | 39 | ||
| Fair Knowledge 18 (60.0%) | 12 (40.0%) | 30 | ||
| Poor Knowledge 15 ((22.4%) | 52 (77.6%) | 67 | ||
Table.1.6: Distribution of Anemia by Knowledge Level about Anemia in Pregnancy.
1.7: Distribution of Anemia among Study participants by their Socio-demographic characteristics
Only occupation of the respondents had a statistically significant association with their anemic status as the P-value was less than 0.05. Hence, anemia was significantly high 20 (74.1%) out of the 27 housewives and 11(64.7%) out of the 17 farmers. There was no association between anemia in pregnancy and the remaining socio-demographic variables since their p-value was > 0.05. (Table 1.7)
| Variable | anemic Status | Total | Chi-Squad, x², P- Value | |
| Non-anemic | anemic | |||
| Age Group | 9.061, 5, 0.107 | |||
| Less or Equal to 18 | 2 (25.00%) | 6 (75.0%) | 8 | |
| 19-23 | 14 (36.8%) | 24 (63.2%) | 38 | |
| 24-28 | 18 (43.9%) | 23 (56.1%) | 41 | |
| 29-33 | 16 (61.5%) | 10 (38.5%) | 26 | |
| 34-38 | 10 (71.40%) | 4 (28.6%) | 14 | |
| Greater than 39 | 5 (55.6%) | 4 (44.4%) | 9 | |
| Marital Status | 0.344, 1, 0.557 | |||
| Single | 12 (42.9%) | 16 (57.1%) | 28 | |
| Married | 53 (49.1%) | 55 (50.9%) | 108 | |
| Occupational Status | 12.435, 4, 0.014 | |||
| Trader | 24 (61.5%) | 15 (38.5%) | 39 | |
| Housewife | 7 (25.9%) | 20 (74.1%) | 27 | |
| Farmer | 6 (35.3%) | 11 (64.7%) | 17 | |
| Government worker | 7 (77.8%) | 2 (22.2%) | 9 | |
| Others | 21 (47.7%) | 23 (52.3%) | 44 | |
| Religion | 1.077, 1, 0.299 | |||
| Christian | 36 (52.2%) | 33 (47.8%) | 69 | |
| Muslim | 29 (43.3%) | 38 (56.7%) | 67 | |
| Educational Status | 26.085, 4, <0.001 | |||
| None | 9 (31.0%) | 20 (69.0%) | 29 | |
| Primary | 18 (31.6%) | 39 (68.4%) | 57 | |
| Secondary | 16 (69.6%) | 7 (30.4%) | 23 | |
| Vocational | 7 (87.5%) | 1 (12.5%) | 8 | |
| Tertiary | 15 (78.9%) | 4 (21.1%) | 19 | |
Table 1.7: Distribution of Anemia among Study participants by their Socio-demographic characteristics
1.8: Distribution of Anemia among Study participants by their Obstetric and Antenatal background.
Only number of folate/iron intake as a variable had a statistically significant association with the anemic status of study respondent as the P-value was less than 0.05. There were more Non-Anemics, 45 (86.5%) among the 52 that took their supplement twice daily. Also, anemia prevalence was significantly high, 4(80%) among the 5 that had never taken any iron or folate supplementation. (Table. 1.8)
| Variable | anemic Status | Total | Chi-Squad, x², P- Value | |
| Non-anemic | anemic | |||
| Gravidity | 8.926, 7, 0.258 | |||
| One (1) | 21 (48.8%) | 22 (51.2%) | 43 | |
| Two (2) | 13 (44.8%) | 16 (55.2%) | 29 | |
| Three (3) | 11 (37.9%) | 18 (62.1%) | 29 | |
| Four (4) | 9 (52.9%) | 8 (47.1%) | 17 | |
| Greater than Four(>4) | 11(61.1%) | 7 (39.9%) | 18 | |
| Parity | 5.718,7, 0.573 | |||
| Zero (0) | 23 (47.9%) | 25 (52.1%) | 48 | |
| One (1) | 13 (39.4%) | 20 (60.6%) | 33 | |
| Two (2) | 10 (45.5%) | 12 (54.5%) | 22 | |
| Three (3) | 10 (58.8%) | 7 (41.2%) | 17 | |
| Four (4) | 8 (61.5%) | 5 (38.50%) | 13 | |
| Greater than Four(>4) | 1 (33.3%) | 2 (66.7%) | 3 | |
| Age of Youngest Child | 4.572, 2, 0.102 | |||
| Less thanTwo (2) | 7 (29.2%) | 17 (70.8%) | 24 | |
| Greater or equalto Two | 34 (54.8%) | 28 (45.2%) | 62 | |
| (≥2) | ||||
| None | 24 (48.0%) | 26 (52.0%) | 50 | |
| Current Gestational Age | 0.781, 2, 0.677 | |||
| 1st Trimester | 18 (51.4%) | 17 (48.6%) | 35 | |
| 2nd Trimester | 32 (49.2%) | 33 (50.8%) | 65 | |
| 3rd Trimester | 15 (41.7%) | 21 (58.3%) | 36 | |
| Gestational Age at 1st ANC visit | 2.609, 2, 0.271 | |||
| 1st Trimester 51 (51.5%) | 48 (48.5%) | 99 | ||
| 2nd Trimester 14 (38.9%) | 22 (61.1%) | 36 | ||
| 3rd Trimester 0 (0.0%) | 1 (100.0%) | 1 | ||
| Number of timesattending ANC | 11.102, 8, 0.196 | |||
| Zero (0) | 18 (47.4%) | 20 (52.6%) | 38 | |
| One (1) | 13 (38.2%) | 21 (61.8%) | 34 | |
| Two (2) | 6 (46.2%) | 7 (53.8%) | 13 | |
| Three (3) | 9 (69.2%) | 4 (30.8%) | 13 | |
| Four (4) | 5 (62.5%) | 3 (37.5%) | 8 | |
| Greater or equalto five | 14 (46.7%) | 16 (53.3%) | 30 | |
| (≥5) | ||||
| Variable | anemic Status | Total | Chi-Squad, x², P- Value | ||
| Non-anemic | anemic | ||||
| Are you Currently on Iron/Folate Tablets | 0.837, 1, 0.360 | ||||
| Yes 46 (50.5%) | 45 (49.5%) | 91 | |||
| No 19 (42.2%) | 26 (57.8%) | 45 | |||
| When did you start taking them | 1.80, 2, 0.411 | ||||
| 1st Trimester 37 (53.6%) | 32 (46.4%) | 69 | |||
| 2nd Trimester 9 (42.9%) | 12 (57.1%) | 21 | |||
| 3rd Trimester 0 (0.0%) | 1 (100.0%) | 1 | |||
| How many do you take in a week | 65.806, 4, <0.001 | ||||
| Twice Everyday 45 (86.5%) | 7 (13.5%) | 52 | |||
| Some days 1 (3.6%) | 27 (96.4%) | 28 | |||
| Few times a week 0 (0.0%) | 12 (100.0%) | 12 | |||
| Never 1 (20.0%) | 4 (80.0%) | 5 | |||
| Not yet 18 (46.2%) | 21 (53.8%) | 39 | |||
Table. 1.8: Distribution of Anemia among Study participants by their Obstetric and Antenatal background.
1.9: Distribution of Anemia among Study participants by their Health and Nutritional background
Anemia was significantly high in 21 (70%) of the 30 respondents who did not sleep under insecticide treated nets. Also, non-anemic respondents were significantly high in 59 (60.8%) of the 97 who were not diagnosed with malaria in the last six (6) months. (Table.1.9)
| Variable | Anaemic Status | Total | Chi-Squad, x², P- Value | ||
| Non Anaemic | Anaemic | ||||
| Do you sleep under an Insecticide TreatedNet | 4.884, 1, 0.027 | ||||
| Yes 56 (52.8%) | 50 (47.2%) | 106 | |||
| No 9 (30.0%) | 21 (70.0%) | 30 | |||
| Diagnosed of malariain the past 6 Months | 23.019,1, 0.000 | ||||
| Positive 6 (15.4%) | 33 (84.6%) | 39 | |||
| Negative 59 (60.8%) | 38 (39.2%) | 97 | |||
| Sickling Status | 1.858, 1, 0.173 | ||||
| Postive 0 (0.0%) | 2 (100.0%) | 2 | |||
| Negative 65 (48.5%) | 69 (51.5%) | 134 | |||
| How many males do you take in a day | 20.904, 2, 0.000 | ||||
| Two(2) 4 (12.5%) | 28 (87.5%) | 32 | |||
| Three(3) 46 (59.0%) | 32 (41.0%) | 78 | |||
| More than Three(3) 15 (57.7%) | 11 (42.3%) | 26 | |||
| Weekly intake of Liver, Beef, Chicken, Fish | 20.325, 3, 0.000 | ||||
| One(1) 1 (25.0%) | 3 (75.0%) | 4 | |||
| Two(2) 7 (20.6%) | 27 (79.4%) | 34 | |||
| Three(3) 27 (48.2%) | 29 (51.8%) | 56 | |||
| More than Three(3) 30 (71.4%) | 12 (28.6%) | 42 | |||
| Weekly intake of Beans, Vegetables, Nuts,Fruits, Grains | 4.362, 3, 0.225 | ||||
| One(1) 2 (50.0%) | 2 (50.0%) | 4 | |||
| Two(2) 6 (37.5%) | 10 (62.5%) | 16 | |||
| Three(3) 37 (56.9%) | 28 (43.1%) | 65 | |||
| More than Three(3) 20 (39.2%) | 31 (60.80%) | 51 | |||
| How many timesdo take tea in a week | 18.902, 3, 0.000 | ||||
| Everyday 0 (0.0%) | 2 (100.0%) | 2 | |||
| Somedays 2 (11.8%) | 15 (88,2%) | 17 | |||
| Few days a week 15 (37.5%) | 25 (62.5%) | 40 | |||
| None 48 (62.30%) | 29 (37.7%) | 77 | |||
Table.1.9: Distribution of Anemia among Study participants by their Health and Nutritional backgroun
The overall prevalence of anemia among the pregnant women was 52.2%, of which 30.9% of all the pregnant women were mildly anemic, 19.9% were moderately anemic and 1.5% were severely anemic. (Table1.4/Fig. 2). This finding is similar to the prevalence of 52% of anemia in pregnancy within the Sub-Saharan Africa (11). The results from this study is also consistent with the finding from a study conducted in 2009 which revealed a 56- 61% prevalence of anemia in pregnancy in developing countries A report from the world Bank in 2016 revealed a 54% of prevalence of Anemia among pregnant Ghanaian Women, which is slightly higher than our 52%. However, the prevalence is far lower than the study in Gushegu (Also a rural town in Northern Ghana), that showed a prevalence of 76.8% among pregnant women (12) and results from a study conducted in Bimbilla (Another rural town in Northern Ghana), which yield a prevalence of 75.3% among pregnant women [13].
Knowledge on anemia in pregnancy was assessed on the basis of knowing the signs/symptoms, causes/risk factors, and preventive measures of anemia in pregnancy. In this study, 69.1% of the respondents had been educated on anemia in pregnancy, while 30.9% of the respondents had never been educated on anemia in pregnancy (Table.1.6). Those who were not educated explained that was their first time of antenatal care. Among those that had been educated on anemia in pregnancy, the majority of them received the education during their routine antenatal care visits, while the rest were educated by family and friends.
Our results revealed that there is an association between the respondents’ knowledge about anemia in pregnancy and the likelihood of them been anemic. (p -value <0.001 and 0.001). 59.6% of the those educated on anemia were not anemic, whiles 78.6% of those that had never been educated on anemia in pregnancy were anemic. Concerning knowledge on anemia in pregnancy, 64.7% of the pregnant participants had poor knowledge on the signs/symptoms of anemia in pregnancy while only 2.9% had good knowledge, 54.4% of the pregnant participants had poor knowledge on the causes/ risk factors of anemia in pregnancy while 9.6% had good knowledge and 49.3% of the pregnant participants had poor knowledge on the preventive measures of anemia in pregnancy while 22.1% had good knowledge (Table 1.6 ) . This implies that more targeted educations efforts at the antenatal care unit are needed to help reduce the prevalence of anemia in pregnancy at the district level. This finding however differs from a study conducted in Ethiopia where 71.6% of the study participants were able to identify the symptoms of anemia, regarding causes, a combined 72.9% knew the causes of anemia and 57.3% had good knowledge towards the prevention of anemia in pregnancy [14].
There was a significant association (p-value 0.014) between the occupational status and the anemic status of the pregnant participant, where 74.1% of housewives and 64.7% of farmer were anemic and, only 38.5% of traders and 22.2% of Government workers were anemic. This is consistent with a study conducted in Gushegu, where 53.4% of housewives were anemic (12) but not consistent with a study which showed that 33% of employed pregnant women were anemic as opposed to 39% unemployed pregnant women who were anemic [15]. There was also a significant association (p-value <0.001) between the educational status and the anemic status of the pregnant participant, where 69.0% of those without any formal education and 68.4% of those with only primary level education were anemic, while, 87.5% of those with vocational level education and 78.9% of those with tertiary level education were not anemic. This is similar to the study in Gushegu, where 67.4% of pregnant women who had not received any form of formal education were anemic (12). However, there was no association between anemic status of pregnant participants and age, marital status and religion. This is contrary to the findings from a study in Sekyere West District, Ghana where there was a significant association between age and the anemic status of the pregnant participant, where prevalence of anemia was lower prevalence with increasing age of women [16].
Under the obstetric and antenatal background, only the number of times of iron/folate intake was significantly associated with the anemic status of the study respondents, with a high anemia prevalence of 96.4% and 80.0% in pregnant women who took in the iron/folate supplements some days in a week and never taken at all respectively. However, variables such as gravidity, parity, number of antenatal care attendance and whether currently on iron/folate supplement were not significantly associated with the anemic status of the pregnant women. This result somehow does not correspond with a study conducted in Accra, Ghana where parity and number of antenatal care visits where significantly associated with anemia in pregnancy. In the same study, However, gestational age was not significantly associated with anemia in pregnancy [17].
There was an intrinsic association between the anemic status of the pregnant women and sleeping under insecticide treated nets, number of meals taken in day, weekly intake of heme containing meals and weekly intake of tea (p-value 0.027, < 0.001, <0.001 respectively). 70.0% of pregnant women not sleeping under insecticide treated nets were anemic, 87.5% of pregnant women who ate only twice a day were anemic, 75.0% and 79.4% of pregnant women who ate heme containing foods only once and twice a week respectively were anemic, while 100% and 88.2% of pregnant women who consumed tea every day and somedays in a week were anemic. This result is different from the findings of a study conducted in the Bolga Regional Hospital, Ghana where there was no significant association between the number of meals taken in a day and the anemic status of the pregnant women [18]. Furthermore, a study conducted in Northern Ghana showed that the use of insecticide treated nets and anemia in pregnancy had no significant association as it did not differ among anemic and non-anemic participants; meanwhile sickling status was not significantly associated (p-value = 0.173) with the anemic status of the pregnant women [19]. However, sickling status was not significantly associated (p-value 0.173) with the anemic status of the pregnant women.
Study Limitations
Due to the disparities in the gestational ages of our respondents, we could not get the hemoglobin (Hb) levels at 28 and 36 weeks of gestation rather, the current Hb Level and Hb level at booking were used for data analysis. Data on the Morphological characteristics of the red blood cells was not available to help identify and classify the types of anemias. Most respondents did not have stool and urine microscopy done to identify Schistosoma species, Entamoeba histolytica, hookworm ova as some of the possible causes of anemia. The sickling status of some respondent was also not readily available for assessment.
Though this study was solely conducted within the West Gonja hospital as it has the highest antenatal visit turnout, the study findings cannot be used to generalize for the entire district. The study methodology did not create a conducive environment for the researchers to follow up on some of the participants who were most likely to experience pregnancy related complications due to their anemic status
From our research, the prevalence of anemia among pregnant women attending antenatal care at the West Gonja Hospital was 52.2%. The majority of the expectant mothers claimed to have been educated about the most relevant and common characteristics of anemia in pregnancy. Despite this knowledge, a significant number of the pregnant women exhibited very poor knowledge especially regarding the possible causes, risk factors as well as practical strategies to prevent anemia in pregnancy. And since the knowledge was associated with the anemic status of the pregnant women, most pregnant women who had poor knowledge on the signs/symptoms, causes/risk factors, and preventive measures of anemia in pregnancy were also anemic. The risk factors of anemia in pregnancy identified were unemployment (housewife), low educational status, noncompliance with iron/folate supplementation, not sleeping under insecticide treated nets, eating less than three times a day, eating less than three heme containing meals a week, daily tea consumption everyday whiles pregnant.
Acknowledgement
The authors of this study want to officially acknowledge the Management Team and Staff of the West Gonja District Hospital, especially all the nurses at the antenatal care unit for all their support and cooperation during the data collection Period.
Declaration of conflict of interest
The authors have no conflict of interest to declare
Source of funding
No financial support was received from any public or private institution for the conduct of this research. The activities of this research were conducted using monies from the annual Book and research allowances allocated by the Government of the republic of Ghana to every researcher within the public academic/research Institutions
Data availability Statement
The processed mixed qualitative/quantitative data that supports the findings and conclusions of this study are readily available through the corresponding author.
The research idea was conceived by MMDM and approved by all authors after putting the research topic through a re-wording exercise. MA conducted the literature review and collected all the relevant data. OR performed the data analysis. The Manuscript was written by MMDM, reviewed by all authors who agreed with its content and made a collective decision to submit for consideration and possible publication
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
