
Research Article | DOI: https://doi.org/10.31579/2690-4861/228
1 Medical Biology Laboratory of the National Hospital Center-Nouakchott.
2 Faculty of Medicine of Nouakchott.
3 Nephrology-Hemodialysis Department of the National Hospital Center-Nouakchott.
*Corresponding Author: Mohamed Lemine Ould Salem, Medical Biology Laboratory of the National Hospital Center-Nouakchott.
Citation: Mohamed Lemine Ould Salem, Moctar Elbou Bellamech, Mah Sidi Mohamed, Ghaber Sidi Mohamed (2022) Prevalence and Clinico-Biological Characteristics of Viral Hepatitis B and C in Chronic Hemodialysis Patients at the National Hospital Center of Nouakchott-Mauritania. International Journal of Clinical Case Reports and Reviews. 11(4); DOI: 10.31579/2690-4861/228
Copyright: © 2022 Mohamed Lemine Ould Salem, This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 02 June 2022 | Accepted: 09 June 2022 | Published: 16 June 2022
Keywords: CRF; HBV; HCV;nouakchott; mauritania
Introduction: Chronic renal insufficiency is a common pathology both nationally and worldwide, infections with hepatitis B and C viruses are the most common infectious complication in chronic hemodialysis patients.
Objective: The objective of this study was to determine the prevalence of hepatitis B and C in chronic hemodialysis patients at the National Hospital Center of Nouakchott and to identify the risk factors for these infections as well as their clinical and biological complications in this population
Material and Methods: This is a prospective study carried out at the nephrology-hemodialysis department of the National Hospital of Nouakchott over a period of one year from 1st, 2016 to December 31st, 2016
Demographic, clinical, epidemiological, and biological data were collected using a pre-established survey form
The search for HBsAg was done by the ELISA technique and the detection of anti-HCV antibodies was done by the CMIA technique (Abbott®), the HCV RNA was searched for by real-time PCR (Abbott)
Results
The average age of our patients was 52 years old with a female predominance
The prevalence of hepatitis B was 24.27% and that of hepatitis C was 5.82%, 1.92% of patients were coinfected with HBV and HCV
The duration of dialysis and the number of transfusions were the main risk factors for catching these infections.
Conclusion the risk factors found in our study were comparable to the literature; the high prevalence of hepatitis B in our series could be linked to its high prevalence in the general population but also to a nosocomial infection.
Viral hepatitis B and C are systemic infections that preferentially affect the liver, they cause inflammatory lesions and hepatocyte alterations, they constitute a public health problem [1] the seriousness of the infection by the hepatitis B and C viruses lies in the risk of evolution towards chronicity and the occurrence of complications such as cirrhosis and hepatocarcinoma [2]. This results in an increase in morbidity in this population. The usual mode of transmission of hepatitis B is parenteral or percutaneous exposure such as blood transfusions, hemodialysis, use of unpasteurized plasma products, accidental needle sticks, injections with unsterilized instruments, ear piercing and dental procedures. Among health professionals, hepatitis B has become the first occupational disease [3].
The hepatitis C virus is a positive-sense single-stranded RNA Flavivirus [3]. The HCV genome is highly variable at present, 6 different genotypes have been observed. The prevalence of hepatitis C in hemodialysis remains high in developing countries; it was 32.6% in Tunisia [4] and 19.2% in Senegal in 2009[3], and that of hepatitis B in hemodialysis ranging from 2 to 15.38% [3.5], in Senegal it was 3.4% in 2009 [3].
In Mauritania, a country endemic for hepatitis B, the prevalence of HBV in the general population is 16 to 25% and that of hepatitis C is 1.1% [6,7].
End-stage chronic renal failure (ESRD) represents the ultimate evolution of any nephropathy [3]. CKD is a public health problem and its incidence has been increasing in recent years worldwide [8].
In Mauritania, and despite the absence of a study, about 1,200 patients are on chronic hemodialysis, ie a prevalence of about 341 per million inhabitants.
At the end stage of CRF, a replacement treatment is unavoidable (hemodialysis; peritoneal dialysis) or kidney transplantation [3,9].
This technique exposes to multiple complications including infection by hepatitis B and C viruses [2,3,5].
The lack of data on the prevalence of HBV and HCV in this population in our country prompted us to carry out this study, which aims to:
- to determine the prevalence of hepatitis B and C in chronic hemodialysis patients at the level of the nephrology-hemodialysis service of the National Hospital Center of Nouakchott;
- and to identify the main risk factors for hepatitis B and C in chronic hemodialysis patients.
2.1 Study material
2.1.1. Study framework:
The study took place in the hemodialysis nephrology department of the National Hospital Center of Nouakchott (CHN).
2.1.2. Study population
2.1.2.1. Inclusion criteria
Were included, all patients with end-stage chronic renal failure who have been regularly on hemodialysis for more than 3 months.
2.1.2.2. Exclusion criteria
Patients with acute renal failure and vacationers were not included in this study.
2.1.2.3. Dialysis tools
The generators used in the service were of the GAMBRO-k95 type
The various products used for the sterilization of the generators and the enclosure of the hemodialysis unit were bleach and citric acid.
The generators were sterilized according to the manufacturer's recommendations.
There were specific generators for patients with hepatitis B.
Hepatitis B and HIV viral serologies were systematically performed before patients were admitted for their first hemodialysis sessions.
There were no dedicated generators for HCV patients
2.1.2.4. Type and period of study
This is a descriptive cross-sectional study of the period from January 1 to December 31, 2016
2.1.2.5. Collection of data
For each patient included, the information was collected on a pre-established form.
2.1.2.6. Parameters studied
For each patient included were studied:
Age, address, sex and marital status.
The duration of hemodialysis (in months), the number of sessions per week, the number of hours per session, causal nephropathy, number of transfusions.
Clinical parameters: the clinical data of hepatitis have been collected, these are:
- Transaminases, Alkaline Phosphatase (ALP), Gamma Glutamyl Transferase (GGT), Total Bilirubin (BT), Conjugated Bilirubin (BC), Prothrombin Level (TP), Complete Blood Count (NFS).
- Hepatitis B and C serology:
Were considered carriers of the hepatitis B virus patients whose Hbs Ag was positive and were considered carriers of the hepatitis C virus patients whose search for HCV RNA was positive.
► Imaging:
Abdominal ultrasound results.
Hepatitis C viral replication assessment was performed only in patients with anti-HCV antibodies.
Detection of HCV RNA was done by a standardized method of reverse transcription followed by amplification by DNA polymerase chain reaction.
Serum HCV RNA concentration was measured using a standardized RT-PCR method.
The search for hepatitis B virus: the detection of (AgHBs) was made by the ELISA technique.
Anti-HCV antibodies (AC) were screened with the CMIA-ARCHITECT ® anti-HCV version 2 kit (Abbott diagnostics), using a microparticle immunoassay by chemiluminescence for the automated qualitative detection of AC directed against HCV in plasma. or human serum. It uses two recombinant proteins.
The search for and quantification of viral RNA were carried out using the Abbott Kit called (Abbott Real Time HCV) for patients whose search for antibodies was positive.
2.2.1. Statistical analysis
The data collected was entered and analyzed with SPSS Statistic 20 and Excel 2013 software.
2.2.2 . Limits of the study: Hepatitis C genotyping was only done for two patients due to lack of resources
3.1 Prevalence:
During the study period, 105 patients were on chronic hemodialysis, among whom one hundred and three patients had benefited from hepatitis B and C serologies, among them the following results were recorded:
- Six patients were in contact with the hepatitis C virus, a prevalence of 5.82%.
- Twenty-five patients with HBV, a prevalence of 24.27%.
- Two patients who were both carriers of HBV and HCV, a prevalence of 1.94%.
In total, the number of patients who were affected by hepatitis B or C or B and C at the same time was 33 patients with a prevalence of 32.03%.
3.2 Epidemiological aspects
3.2.1 Age:
The age of the patients varies between 30 and 65 years old and the average age is 52 years old;
The age groups of (50-59), (40-49) and (60-69) were the most represented. The distribution of patients by age group is shown in Table I
| Age | Number | Percentage |
| 30 –39 | 8 | 24.25% |
| 40−49 | 4 | 12.12% |
| 50−59 | 11 | 33.33% |
| 60−69 | 10 | 30.30% |
| Total | 33 | 100% |
Table I: Distribution of patients according to age groups
3.2.2 Gender:
3.2.3 Initial nephropathy:
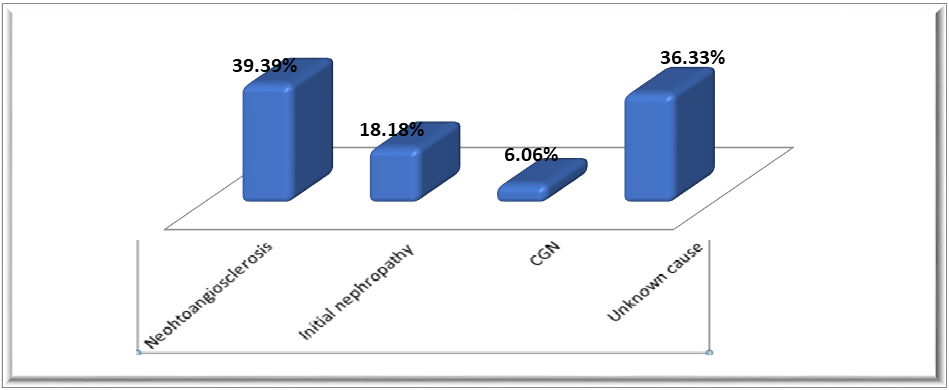
The first causative nephropathy in our study population was nephro-angiosclerosis (39.39%) followed by diabetic nephropathy (18.18%) and in (36.33%) cases the cause was undetermined, while the chronic glomerulonephritis (CNG) represent (6.06%). The distribution of patients according to the type of initial nephropathy is shown in Figure 1.
3.2.4 Duration in hemodialysis:
The average duration in hemodialysis is 50.52 months with extremes of 7 months and 228 months, patients on hemodialysis for more than two years
represented the largest slice 48.48% and those who were on dialysis for more than nine years represented 9 .09%, The distribution of patients according to the duration of hemodialysis is shown in Table II
| Duration of dialysis in months | Number | Percentage |
| 05– 30 | 16 | 48.48% |
| 31−50 | 09 | 27.27% |
| 51−100 | 05 | 15‚15% |
| 101−230 | 03 | 09.10% |
| Total | 33 | 100% |
Table II: Distribution of patients according to duration in hemodialysis
3.2.5 Transfusion status:
Twenty-three patients (23) had been transfused with red blood cells with more than 5 transfusion sessions. The distribution of patients according to their transfusion status is shown in Table III:
| Transfusions | Number | Percentage |
| Patients transfused more than 5 times | 23 | 69.70 % |
| Patients transfused less than 5 times | 10 | 30.30 % |
| Total | 33 | 100 % |
III: Distribution of patients according to transfusion status
3.3.1. Signs of liver damage:
- Seven patients had ascites, i.e. a rate of 21.2%:
It is often a distended abdomen with no protrusion of a hernial orifice, or unfolding of the umbilicus with sloping dullness of the mobile flanks when changing position.
- Two patients had jaundice, i.e. a rate of 6.06%
- Three patients had hepatomegaly, a rate of 09.09%
It is a hepatomegaly of hard consistency, nodular surface with a sharp lower edge (one patient), the other two patients had a homogeneous hepatomegaly of firm consistency with a soft lower edge
- Two patients had collateral venous circulation, i.e. a rate of 06.06%
3.4. Biological aspects
PT | Patients | Percentage % |
Normal | 27 | 81.81% |
<70> | 06 | 18.19% |
Total | 33 | 100% |
Table IV: Distribution of patients according to hemoglobin (Hb) level
3.4.1. Hemoglobin (Hb) level
The average hemoglobin level in patients was 8.5 g/dl ±1.83 with extremes of 4g/dl and 13g/dl, the distribution of patients according to their hemoglobin levels is represented by Table IV.
3.4.2. Transaminases:
3.4.2.1. Aspartate-aminotransferase (ASAT):
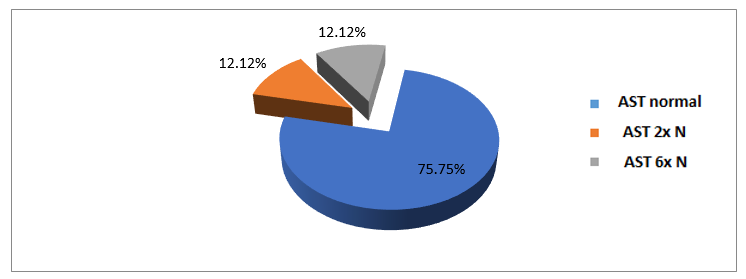
The average AST level was 59.8 IU/l, with extremes of 15 and 290 IU/l. The distribution of patients by AST level is shown in Figure 2.
3.4.2.2. Alanine-aminotransferase (ALT):
The average ALT level in our patients was 59.9 IU/l, with extremes of 10 and 316 IU/l. The distribution of patients according to ALT level is shown in Table V.
ALT | Number | Percentage |
normal rate | 24 | 72.73% |
Rate 2x normal | 05 | 15.15% |
Rate 5 x normal | 02 | 06.06% |
Rate 7 x normal | 02 | 06.06% |
Total | 33 | 100% |
Table V: Distribution of patients according to ALT level
3.4.3. Bilirubin:
The average level of total bilirubin in patients was 6mg/l with extremes of 3mg/l and 121mg/l.
The average level of conjugated bilirubin in patients was 3.6 ± 2.63mg/l with extremes of 2mg/l and 18mg/l.
Twenty-seven (27) of the patients had a normal bilirubin level, i.e. a rate of 81.81% and 06 patients had a conjugated hyperbilirubin, i.e. a rate of 18.18%.
3.4.4. Gamma GT rate:
The average level of gamma GT in our patients was 94.5UI/l with extremes of 11UI/l and 385UI/l
3.4.5 Alkaline Phosphatase (ALP)
The average level of ALP in patients was 139.18 IU/l with extremes of 45UI/l and 406UI/l .
3.4.6. Prothrombin TP rate:
The TP was low in six patients, i.e. 18.19%; the distribution of the patients according to the rate of TP is represented in table VI .
PT | Patients | Percentage % |
Normal | 27 | 81.81% |
<70> | 06 | 18.19% |
Total | 33 | 100% |
Table VI : Distribution of patients according to PT rate
3.5. Morphological aspects:
3.5.1 Appearance of the liver on abdominal ultrasound
Twelve point thirteen percent (12.13%) of patients had an ultrasound appearance of hepatic cirrhosis.
3.6. Virological aspect
Twenty-five (25) patients are carriers of HBsAg, i.e. a prevalence of 75.75%.
The virus | Number of patients | Percent | prevalence |
HCV | 06 | 18‚18% | 05.45% |
HBV | 25 | 75.75% | 22.57% |
HCV-HBV co-infection | 02 | 06.07% | 01.85% |
Total | 33 | 100% |
Picture VII : Distribution of patients according to their virological status
3.6.2. Distribution of patients according to viral replication
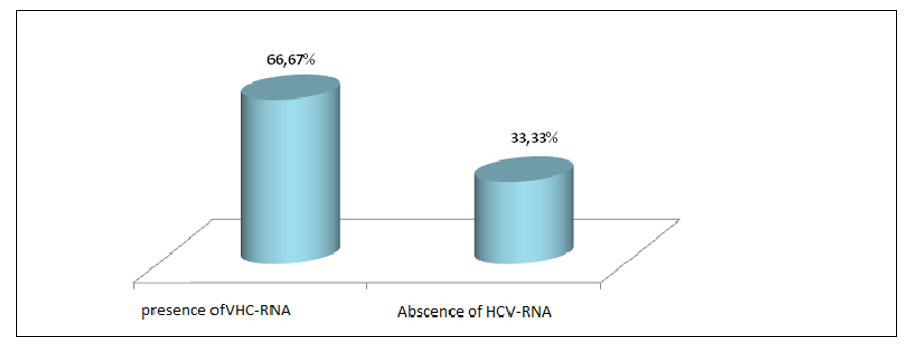
The viral load was made only for HCV, in these the presence of the RNA of this virus was noted in 66.66% (four patients), and the average viral
load was 67369 IU/ml with extremes of 10559 IU/ml and 542819 IU/ml FIG. 3 represents the distribution of patients according to viral replication.
3.6.3. Distribution of patients according to genotyping
Genotyping was only done for two patients, they were type 4.
4.1. Epidemiology
4.1.1 Prevalence
4.1.1.1. Hepatitis B :
Out of 33 affected patients, 25 patients were carriers of the hepatitis B virus, ie a rate of 75.75%, with a prevalence of 24.27%.
In Senegal, Alaoui M had found a rate of 6.7% [1], in Mali Ould Bezeid had found a rate of 15.38% [10], Boulaajaj K et al in Morocco found a rate of 12.3% [5], Hamida in Tunisia had found a rate of 8% [11] , in Libya Christiana T et al found a rate of 31.1% [12] .
The prevalence of hepatitis B varies between 2.6% in Iran [13], 6% in Russia [14].
Data published in the Dialysis Outcomes and Practice Patterns Stud (DOPPS) in 2003 on 308 hemodialysis centers in Europe and the United States showed that the prevalence of HBsAg was between 0 and 7% [15].
The prevalence of hepatitis B in the different countries of the sub-region is shown in table VIII
| Author | Country | Prevalence |
| Christiana T [12] | Libya | 31.1% |
| Alaoui M [1] | Senegal | 6.7% |
| Ould Bezeid [10] | mali | 15.38% |
| Hamida [ 11 ] | Tunisia | 8% |
| Boulaajaj K [5] | Morocco | 12.3% |
| Our series | Mauritania | 24.27% |
Table VIII : Prevalence of hepatitis B in chronic hemodialysis patients
This very high rate of hepatitis B among hemodialysis patients in our series is undoubtedly related to the very high prevalence of hepatitis B in the general population in Mauritania (16-25%) [7], and also related with very high prevalence among blood donors (20.3%) [7]. This does not exclude the very existence
probable nosocomial transmission within the hemodialysis department by infection of the dialysis equipment and by the use of heparin injections in several patients.
These HBsAg positive patients should benefit from complete hepatitis B serology (anti-HBc AC, HBeAg, anti-HBe AC, viral load, etc.) to allow proper monitoring of this infection in this vulnerable population.
4.1.1.2 Hepatitis C
Six patients among our 33 patients were in contact with the hepatitis C virus, i.e. a prevalence of 5.82%,
Hepatitis C virus RNA was present in 4.
In two patients among the HCV seropositives, the search for viral RNA was negative.
Due to the very high cost, genotyping was only done for two patients, they were type 4.
This prevalence of hepatitis C was very high compared to that of the general population in Mauritania (1.1%) [6,7],
Hepatitis C is a common complication of chronic hemodialysis. Her
prevalence is highly variable in dialysis patients from one country to another.
In Africa, it was respectively 19.3%, 26.5%, 68.3% and 32.6% in Senegal, Benin, Morocco and Tunisia [1,2, 16,17,19]. Cassidy in South Africa found a rate of 23% [18].
In developed countries, this prevalence is lower. The study
Prospective Observational DOPPS performed in hemodialysis patients
taken randomly from 308 dialysis centers in France, Germany, Italy, Japan, Spain, the United Kingdom and the United States showed an average prevalence of HCV infection of 13% [15].
A meta-analysis published in 2008 in (the American journal of nephrology) which grouped together all the studies which reported the prevalence of HCV in chronic hemodialysis patients published from 1980 to 2005 showed that the highest prevalences been observed in Peru, Brazil, Senegal, Syria, Tunisia, Pakistan, Saudi Arabia and Iran [19] .
However, this prevalence recorded in our series remains lower compared to that recorded in certain African countries, and certain developed countries. The prevalence of HCV in hemodialysis patients is shown in Table IX
| Country | Year | Prevalence |
| France [20 ] | 2008 | 1.7% |
| Tunisia [19] | 1996 | 40% |
| Morocco [17] | 2008 | 35.5% |
| Senegal [1] | 2009 | 19.3% |
| Our series | 2016 | 5.82% |
Table IΧ: Prevalence of hepatitis C in hemodialysis patients
This relatively high prevalence in our series compared to the general population could be related to the repetitive blood transfusions in the majority of our patients but also the seniority in hemodialysis.
Nevertheless, the risk of nosocomial transmission cannot be ruled out, especially for vacationing patients who have benefited from hemodialysis sessions in other centers both inside and outside the country.
4.1.1.3 Hepatitis B and C co-infection
The prevalence of hepatitis B and C co-infection in our series was 1.85% (two patients) in Senegal this prevalence was 0.03% [1], this high prevalence may be linked to the very high prevalence of HBV in the general population in Mauritania [7]. Adane T et al. found the pooled overall prevalence of HBV and HCV infection in HD patients in Africa was 9.88%[21] .
4.1.2 Age:
The average age of the patients was 52 years old with extremes of 30 and 69 years old.
Twenty-three patients were aged between 30-59 years, a rate of 69.69%.
It is therefore a relatively young population joining the data of the literature in the countries of the sub-region [1].
In Africa, the average age of patients varies according to the studies [5,18].
In Senegal, Alaoui [1] had found an average age of 49 years.
Yacoub in Tunisia had found an average age of 54.7 years ans [19].
Ben Amar in Morocco had found an average age of 43 ans [9]
In Mali, Baby M had found an average age of 42 ans [21].
These results observed in developing countries nevertheless contrasted with those found in developed countries where CKD is more common in the elderly. Fabrizi in Italy found an average age of 62.6 ans [22].
Nakayama in Japan, had found an average age of 54.7 ans [23]
In the United States, Kalantar-Sadeh found an average age of 55.7 [24].
The average age in our patients was relatively lower than that found in the West, this could be explained by a relatively young IRC population in Mauritania [25].
The emergence of a large elderly population in hemodialysis centers in the West and the increase in their life expectancy during dialysis could be another explanation for this age difference, table X represents the average age found in different studies.
| Author | Country | Year | Middle age |
| Alaoui [1] | Senegal | 2009 | 49 |
| Yacoub[19] | Tunisia | 1999 | 54.7 |
| Baby M [22] | mali | 2011 | 42 |
| Kalantar Sadeh[25] | USA | 2005 | 55.7 |
| Our series | Mauritania | 2016 | 52 |
Table X: Different mean ages found in different studies
4.1.3 Sex
In our study, there was a female predominance with a sex ratio (M/F) of 0.65.
In Senegal, Alaoui had found a female predominance with a sex ratio of 0.6 [6]. In Mali, Baby M had found a sex ratio of 1.44 [8].
In France, Cledes et al had found a sex ratio of 1.5 [8]. The female predominance in our series can be explained by the frequency of hypertension and diabetes in Mauritanian women, this frequency would be linked to factors socio-cultural (obesity), on the other hand could be linked to the sex ratio of the general population of Mauritania, which was estimated at 0.97 in 2013 or 50.7% of women according to the National Office of Statistics (Mauritania ) [15].
4.1.4 Duration in hemodialysis
The average duration in hemodialysis in patients was 50.52 months with extremes 7 months and 228 months.
Patients on hemodialysis for more than 2 years represented the largest slice 48.48%, and those on hemodialysis for more than 9 years represented the smallest slice 9.09%.
In Senegal Alaoui had found an average duration of 82.4 months [4].
In Mali, Baby M et al had found that patients with a duration of dialysis of less than 3 years were the most represented, i.e. 83.3% [6], while in Morocco Ben Amar et al had found 89.4 % of hemodialysis patients with a hemodialysis duration of 5 years [9].
This relatively short average duration in hemodialysis found in our series could be explained by the opening of new hemodialysis centers inside the country and the transfer of many former dialysis patients to their towns of origin. It could also have as an explanation the non-compliance with the treatment and the high mortality rate among our dialysis patients linked to cardiovascular complications.
This positive association between the duration of hemodialysis and the occurrence of hepatitis C in this work has already been reported several times in the literature [30] .
For Dussol, in a multicenter study conducted in the south of France, the duration of dialysis beyond eight years appeared to be the main factor in hepatitis C [28].
This duration in hemodialysis in HCV(+) varies from one country to another.
Table XI represents the mean age on dialysis for the HCV positive patients in the various studies.
| Author | Country | Average age on dialysis in years |
| Alaoui [1] | Senegal | 7.03 |
| Yacoub[19] | Tunisia | 6.35 |
| Boulaajaj[5] | Morocco | 8.67 |
| Hashisha[29] | Tunisia | 2.75 |
| Huraib[30] | Saudi Arabia | 4.8 |
| Pol [31] | France | 9 |
| Our series | Mauritania | 4.16 |
Table XI: Mean duration of hemodialysis in HCV positive patients
4.1.5 Transfusion status
Blood transfusion (more than five times) was performed in 69.7% of
patients, in Senegal Alaoui had found an average transfusion of 3.8 times [1].
This figure varies from country to country, Hachicha in Tunisia had found an average of 5.5 [29]. Boulajaj had described in Morocco a higher average (16.5%) [5].
These repeated transfusions are worrying. Indeed, while the hepatitis B virus is systematically screened in blood donors, HCV screening only became systematic and regular in 1999 in the National Center for Blood Transfusion, as well as the transfusion of whole blood without virological tests previously carried out until today in the interior of the country suggesting a significant risk of transmission of HCV.
The incidence and prevalence of HCV contamination in the main European countries had decreased partly thanks to progress in screening blood donors for hepatitis C.
However, blood transfusion remains a classic risk factor for HCV infection in chronic hemodialysis patients. This has been corroborated by several authors in the literature including Nakayama in Japan [24], Alavian in Iran [13] and Ben Amar in Morocco [9].
It should be noted that it is difficult to completely eliminate the risk of transmission of HCV by blood, particularly because of the serological window.
The dosage of transaminases in blood donors and the eviction of those with high transaminase levels is an additional measure applied in some European countries for this purpose, without being perfect.
4.2. Clinical
4.2.1. Causal nephropathy.
4.2. Clinical
4.2.1. Causal nephropathy.
Nephroangiosclerosis (NAS) represented the most frequent causal nephropathy in our series 39.39%.
In Senegal it represented 44.8% [1]. This high frequency is also found in Mali 50% [22]. NAS represented 24%, 29% and 13% of initial nephropathies respectively in France, the United States and Morocco [5].
Diabetic nephropathy accounted for 18.18%, while chronic glomerulonephritis (CNG) accounted for 6.06%.
The rise of vascular and diabetic nephropathy at the expense of glomerular nephropathy in Mauritania as everywhere in the world could be explained by the improvement in the management of Glomerulonephritis but also by the increasing incidence of diabetes and hypertension.
In Morocco, Glomerulonephritis predominates with a rate of 29%, while diabetic nephropathy only represented 7.5% [5].
In France, among the renal diseases responsible for ESRD treated, the proportion of glomerulonephritis
has steadily decreased over the past 30 years, dropping from more than 50 to 13% [7], whereas in Japan Glomerulonephritis remains the most frequent nephropathy with 53.7% [23]. In the United States, half of patients entering dialysis had type 2 diabetes [25].
Indeterminate nephropathies were strongly represented in our series 36.33%. This fact has been reported by other authors , in Morocco these nephropathies represented 37% of cases [5].
This high rate in our study could be explained by the diagnostic delay of IRCT and by the weakness of the technical platform preventing the practice of a renal biopsy which represents the best means of etiological diagnosis.
4.2.2 Clinical manifestations:
Ascites is present in 21.2%, it is probably the essential ascites of dialysis patients. Two patients are jaundiced, a rate of 6.06%. Collateral venous circulation was present in 6.06%, and hepatomegaly in 9.09%.
4.3. Paraclinical
4.3.1 Biology
4.3.1.1 Blood count
Normochromic normocytic anemia, an essential sign of CKD, was found
in most of our patients, in fact the average level of hemoglobin in our patients was 8.5 g/dl ±1.83, despite the practice of blood transfusion, iron supplementation and the use of erythropoietin.
In Senegal, Alaoui found an average hemoglobin level of 8.3 g/dl [1]. These results are similar to those found by Kalantar-Zadeh in the United States [25].
Three patients, a rate of 9.09%, had mild hyperleukocytosis without fever or proven portal of entry, this hyperleukocytosis could be attributed to underlying infections.
There was no leukopenia or thrombocytopenia in the patients studied.
4.3.1.2 Hepatic assessment.
4.3.1.2.1. Transaminases
The average ALT level was 59.9UI/l.
ALT was normal in 24 patients, i.e. a rate of 72.72%, it was twice normal in 5 patients, i.e. a rate of 15.15%
It was five times higher than normal in 2 patients and seven times higher than normal in 2 patients, these are the same patients mentioned above with a cirrhotic appearance of the liver.
In Senegal, Alaoui found an average rate of 45.54 IU/L [1]. This elevation of transaminases in HCV positives was moderate (< 2>
These data should be compared to those of Yacoub in Tunisia [19] and Saravanan in India [33].
In the literature, the level of transaminases is reputed to be a poor marker of HCV infection in chronic hemodialysis patients due to its poor sensitivity [17].
Pol et al had reported an increase in transaminases in only 31% of chronic hemodialysis patients with positive HCV viremia [31]. Salama et al had shown that 89% of chronic HCV RNA (+) hemodialysis patients had normal or subnormal ALT levels [34].
4.3.1.2.2. Bilirubin
The average level of total bilirubin in patients was 6mg/l and the average level of conjugated bilirubin in our patients was 3.6mg/l
Ten patients have hyperbilirubinemia, a prevalence of 30.3%. Among these patients, two are jaundiced, the others have no clinical manifestations.
4.3.1.2.3 Gamma-glutamyl-transferase
The average GGT level in our patients was 94.57 IU/l.
Eleven patients had a normal GGT level, i.e. a prevalence of 33.33%.
Eleven patients had a rate greater than 100IU/l, i.e. a prevalence of 33.33%.
Eight patients had a rate between 40-70 IU/l, i.e. a prevalence of 24.24%.
Three patients had a level between 70-100 IU/l
The increase in GGT can be linked to several factors, including drug causes.
Dalekos et al had suggested that GGTs were more sensitive than transaminases in cases of acute hepatitis C and that any increase in GGT in hemodialysis patients should lead to PCR-HCV [35].
4.3.1.2.4 Prothrombin count
The prothrombin level was lower than normal in 18.19% of our patients, thus evoking hepatocellular insufficiency probably linked to infection by HBV and/or HCV.
4.5.1 Ultrasound appearance of the liver
Four patients, a rate of 12.13%, had an ultrasound appearance of the liver compatible with cirrhosis. On ultrasound, the liver was enlarged in size with a heterogeneous parenchyma of bumpy surface.
Pathological anatomy, the only formal argument for diagnosis, has not been carried out. Its practice is not easy on this ground presenting disorders of the blood crasis and regularly receiving anti-coagulants. The other non-invasive tests (Fibrostest-Actitest, Elastometry) were also not carried out due to a lack of means and availability.
5.1. Conclusion :
Hemodialysis, a commonly used extra-renal purification technique, allows prolonged survival of patients with chronic renal failure who have reached the end stage.
However, it induces many complications, mainly infectious, including viral hepatitis B and C [36,37].
The epidemiological context of Mauritania, located in an area highly endemic for the hepatitis B virus, the terrain and the nature of the treatments, make these patients at high risk for these infections.
In order to determine the prevalence of these hepatitis and their risk factors in hemodialysis patients, we undertook this prospective study in the Nephrology-hemodialysis department of the National Hospital Center of Nouakchott.
During the study period, 105 patients were on chronic hemodialysis, among which one hundred and three patients had benefited from hepatitis B and C serologies.
among which 33 patients are carriers of HBV and/or HCV; in these it was found that the prevalence of hepatitis C in hemodialysis patients is five times higher than in the general population, on the other hand that of hepatitis B is comparable to the general population, the female predominance is noted in our study contrary to the data of the literature, the duration in hemodialysis as well as the number of transfusions are the main risk factors found in our study joining the data of the literature.
This preliminary study should be supplemented by a study over a longer period taking into account the initial viral infection status, particularly for hepatitis C.
Patients with HBsAg must also benefit from a complete serological assessment in order to consider possible therapeutic management.
5.2. Recommendations:
none
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
