
Research Article | DOI: https://doi.org/10.31579/2692-9759/048
1 Chairman Cardiac Science Department, College Of Medicine, King Saudi University, Saudi Arabia.
2 King Fahad Cardiac Center, College of Medicine, King Saud University, Riyadh.
3 Cardiac sciences department, college of medicine King Saud University Riyadh.
4 King Fahad Cardiac Center, College of Medicine, King Saud University, Riyadh.
*Corresponding Author: Mostafa Q Al Shamiri, Chairman Cardiac Science Department, College Of Medicine, King Saudi University, Saudi Arabia.
Citation: Mostafa Q Al Shamiri, Waleed Alharbi, Nouf Abdulaziz Alanazi, Ayman M. Alsaleh, Mobarak M, Alsaluli (2022) Prevalence and Baseline Characteristics of Patients with Heart Failure and Preserved Ejection Fraction at Outpatients Sitting in Saudi Arabia Cardiology Research and Reports 4(3): DOI: 10.31579/2692-9759/048
Copyright: © 2022, Mostafa Q Al Shamiri, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 28 January 2022 | Accepted: 26 February 2022 | Published: 14 March 2022
Keywords: arab population; heart failure; outpatient;systolic function
Objective: The present study aims to estimate the prevalence of heart failure (HF) with preserved ejection fraction (HF-PEF) in patients with HF. The study also compares their clinical characteristics with heart failure and reduced ejection fraction among Saudi out patients.
Methods: A Cross sectional, observational study was conducted by recruiting heart failure patients, who had an echocardiography within one year and the left ventricular ejection fraction >45%. The case report forms monitored for source documentation and accuracy.
Results: The population sample included 26% women; with mean age 58 ±10 years (range 32 to 82). Of these patients, 66 did not have an EF measurement. Of the 330 patients with EF values, 168 had an EF of >45% and were classified as having HF-PEF and 162 had an EF < 45% and were classified as having HF-REF. Calcium channel blocker, thiazides diuretic and ARBs were more frequently used in HF-PEF.
Conclusion: The study concluded that there is a need to develop safe and cost-effective methods for screening high-risk patients with multiple risk factors for the early detection and treatment of heart failure.
Heart failure (HF) increasingly contributes to old edematous condition, dropsy, the pathophysiological role of heart was evident from the definition provided by Lewis in 1933, when HF was recognized as the leading cause of dyspnea and edema. According to Lewis, HF is defined as a condition, when heart fails to pumps the blood adequately [1]. Regardless of the cause, the hemodynamic measurements showed that HF occurred as the result of increase in the cardiac filling pressures. This crucial aspect is highlighted by a recent definition of HF stating that HF is characterized as inability to pump blood at the cost of high filling pressures [2]. HF is associated with increase morbidities and mortalities [3]. A substantial percentage of patients with HF have a normal or preserved left ventricular (LV) ejection fraction (EF) [4]; whereas, almost half of patients with HF have left ventricular ejection fraction (LVEF) that is not markedly abnormal [5].
Heart failure is presented with ejection fraction (EF) of 40% and 50%. The prevalence of HF-PEF varying from 13% to 74% is influenced by the cut off is used to define reduced systolic function from preserved systolic function (HF-PEF) [4, 6]. The prognosis of patients with heart failure and reduced EF (HF-REF) compared to that of patients with HF-PEF is variable [4, 7]. The information related to HF with preserved systolic function in Saudi Arabia, Middle East, and Latin America is scarce. However, the epidemic of coronary artery disease as a result of lifestyle evolution is likely to increase incidence of heart failure [8, 9]. The HF epidemiology in Saudi as middle- East country with population that have different ethnic, cultural, and socio-economic background, which could be different from other parts of developed countries. Therefore, the present study aims to identify patients with HF-PEF and estimate the prevalence of heart failure (HF) with preserved ejection fraction (HF-PEF). The study also compares the clinical characteristics of these patients with heart failure and reduced ejection fraction in Saudi Arabia.
Study Design and Setting
A multi-center, cross-sectional, observational study was conducted in Saudi Arabia to evaluate the prevalence of HF-PEF in ambulatory outpatient visitors.
Study Participants
The patients visiting outpatient clinic aged _> 21 years or more, with HF either newly diagnosed or documented previously as chronic HF were included during a 3-month recruitment period. Framingham clinical criteria used for diagnosis of chronic HF. The inclusion criteria for this study were patient who smoked or had smoked within the previous 12 months, with 1 cigarette/day or more. Moreover, former smokers were those who had stopped smoking >12 months before getting enrolled in the study. Exclusion criteria for this study were patients younger than 21 years and the ones who refused to give consent for being enrolled in the study or were already enrolled in other clinical trial.
Ethical Consideration
The study was conducted in accordance with the principles of Declaration of Helsinki. Moreover, the study had received approval from the local IRB committee. Consent was obtained from each patient before recruiting them in the study.
Study Procedure
The clinical data at the outpatient clinic was collected using standardized international Case Report Form (CRF) that included; patient’s demographics, medical history, cardiovascular risk factors, and associate co-morbidities. Along with this, chest radiography, electrocardiography, Echo-cardiograph, Doppler, and laboratory tests were also studied, if performed, within 12 months preceding the visit. Those with an EF of < or>
Study Parameters
Left ventricular hypertrophy (LVH) by electrocardiography was defined as a Socolow index of >35 mm or Cornell index of > or equal to 28 mm in men and 20 mm in women. The Penn formula used to estimate LV mass and normalized by the body surface area. Echocardiographic LVH was defined as an LV mass index of more than 134 g/m2 for men and 110 g/m2 for women. Concentric and eccentric LVH was defined by a relative wall thickness of > 0.44. The medical practitioners involved in this study randomly were selected at the sites, among an initial representative list of office- or hospital-based internists and cardiologists.
Data Analysis
The statistical analysis was performed using SAS software, version 9.1 (SAS Institute, Cary, North Carolina). The continuous variables were expressed as the mean ± SD and categorical data as the absolute numbers and percentages. Differences between groups were evaluated using the Student t test for continuous data (or the Wilcoxon test if appropriate), the chi-square test for binomial or nominal variables (or Fisher’s exact test, if appropriate), and the Cochran-Mantel-Haenszel test using rank scores for ordinal data. Statistical significance was considered as a 2-tailed Probability of P value= 0.05.
A total of 396 patients were selected in this study to conduct the analysis. The population sample included 26% women with mean age was 58 ±10 years (range 32 to 82). Of these patients, 66 did not have an EF measurement. Thus, the remaining 330 patients (82.5%) constituted the study population. Of these, 43.6% had New York Heart Association functional class III or IV. Of the 330 patients with EF values, 168 had an EF of >45% and were classified as having HF-PEF and 162 had an EF <45>

The HF-PEF population was similar to the HF-REF but HF-REF was presented with dilated cardiomyopathy and heart failure at least one year before being recruited in the study. The blood pressure = 140/90 mm Hg was recorded 24.7% in the HF-PEF patients and 42.2% in the HF-REF group patients (p=0.029). Dilated cardiomyopathy was reported as etiology more frequent in those with HF-REF (31% vs 63%) that was statistically significant at p-value=0.001. HF-PEF was equal to HF-REF considering the age, body mass index (BMI), heart rate (HR), blood pressure (BP), atrial fibrillation (AF), diabetes mellitus (DM), smoking, coronary artery disease (CAD), hypertension, peripheral artery disease (PAD), valvar disease, cerebrovascular disease (CVA), chronic kidney disease (CKD), chronic obstructive pulmonary disease (COPD), and alcohol consumption. The characteristics of the patients with HF without EF values were close to that of those with HF-PEF.
HF-PEF equal to HF-REF in the level of serum sodium, potassium, and creatinine was reported to be 40%, 44%, and 43%, respectively. No significant difference was found between the two groups. However, hemoglobin reported in 40% of patients, with significant reduction in HF-PEF compared to HEF-REF with mean value of 126.6 ± 18.6 and 133.4 ± 19.2, respectively (p-value = 0.038). However, brain natriuretic peptides (BNP) were higher in HF-REF in addition to cardiomegaly revealed through by chest X-ray and left ventricle hypertrophy (LVH) revealed through ECG.
Chest radiographic data were available for 250 patients (63%). Cardiomegaly was more frequently reported in the HF-REF group (68.9 % vs 81.2%; p-value = 0.092); although, the rate of pulmonary edema was the same (43%). Furthermore, the HF-PEF patients were significantly more anemic. Electrocardiography performed in the previous year among 372 patients (94%). The heart rate was equal in both group of patients i.e. 98.3 ± 19.1 beats/min. Electrocardiographic LV hypertrophy, assessed using the Socolow index, was present in 41.9% of patients with no difference between the two groups. LVH was present in 32% of patients and was more frequent in HEF-REF (38.8% vs 19.5 %; p-value = 0.047), using the Cornell index (Table 2).

Echocardiographic Findings
The mean EF was in the normal range among 52.1% of HF-PEF 33.1% in those with HF-REF. Echocardiographic LV hypertrophy was less frequent in the patients with HF-REF (Table 3). Posterior wall of LV and inter-ventricular septum were thicker in HF-PEF, meanwhile LV systolic and diastolic dimension were larger in HF-PEF. Left atrial dimension were equal but left atrial area was greater in HF-PEF. Table 3 shows that E/A ratio was equal in both the groups; however, E/e’ ratio was higher in HF-REF.

Table 4 lists the medication used according to LVEF. The HF-PEF group had a greater prescription rate of calcium channel blockers, angiotensin 2 receptor blockers, and thiazide diuretic; however, angiotensin-converting enzyme inhibitors (ACEI), aldosterone receptor antagonists, loop diuretics, and digoxin were prescribed more often in patients with HF-REF.

The present cross-sectional study has provided the prevalence of HF-PEF among outpatients with HF and a comparison of the clinical characteristics and treatment of patients with HF-PEF versus those with HF-REF encountered in routine clinical practice in Saudi Arabia. The results confirmed that HF-PEF was common and accounted for a significant proportion of patients with HF, because 51% of the patients had preserved EF. Few studies have reported the prevalence of HF-PEF in Saudi Arabia, which was mainly observed among the patients admitted in hospital (Table 5). EF cutoff of 45% (ranging between 40%-55%) was used to compare the result of present study with previous studies conducted on local, regional, and international level.
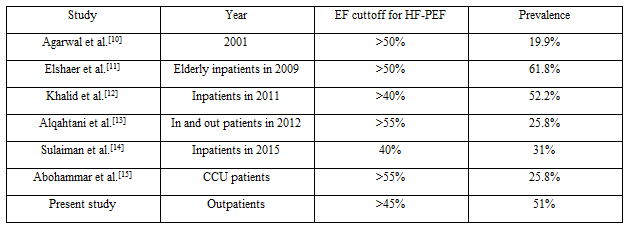
The present study considers outpatients that represent the actual prevalence of HF-PEF. This is as far as the first study that has considered the outpatients populations. The prevalence of HF-PEF recorded in this study was greater than the prevalence reported among the Omani population (19.9%) [10]. A similar study conducted in Latin America recorde prevalence of HF-PEF to be 28%. A review of 30 studies conducted in United States and Europe from 1970 through 1995 noted that the HF-PEF prevalence ranged from 13% to 74% (median value 40%).[16] In 11 studies published from 1998 through 2003, the HF-PEF prevalence ranged from 40% to 71% (mean 54%) [4, 17]. The Euro-Heart Failure Survey reported a percentage of 46.3%, which was probably influenced by the method used to assess LV systolic function and the threshold dividing “preserved” from “reduced” [18]. The present study has recorded different characteristics from the patients with HF-PEF reported in the literature to have advanced age, elevated body mass index, and a more frequent history of hypertension and atrial fibrillation.
The baseline characteristic of HF-PEF revealed no difference between the HF-REF and HF-PEF, except HF-REF is more likely to be diagnosed before first visit, have history of cardiomyopathy, and have controlled BP. The BP control probably relates to intensive anti-failure treatment given to HF-REF patients. The reason for the high proportion of patient already diagnosed HF may be secondary to the outpatient sitting was mostly stable. The hypertension occurrence in both groups was high with no statistical differences (86.9% vs 79%). This was different from other studies performed among older women with diabetes, hypertension, and dyslipidemia [5].
The Coronary artery disease (CAD) prevalence in HF-REF and HF-PEF is 69.1% and 58.3%, respectively with no significant difference. CAD is expected to be higher in HF-REF according to studies conducted locally (50.5% V 22%) [11] and internationally (51% V 27%) [19], (49% V 28%) [20], (63.7 % V 52.9) [21]. All these studies signified that CAD was more common in HF-REF, as compared to HF-PE. The absence of difference in the present study probably relates to the sitting, young patients, outpatients (stable cardiac status), and relation to equal prevalent of risk factors for CAD in both group including, hypertension, dyslipidemia, BMI, smoking and diabetes mellitus. The laboratory analysis revealed no differences between the two groups in term of sodium, potassium renal profile, and cholesterol level. However, HF-PEF patients are more likely to have anemia, LVH by Cornell voltage criteria, and reduced level of BNP. Anemia is common in HF patients and it is associated with increased long-term mortality rates in patients who have diastolic heart failure [22].
The present study revealed that anemia was common among HF-PEF patients and it was similar to one of the local study (35% in CCU hospitalized patient with HF-PEF) [15] and international study, where 43% of HF-PEF had anemia [23]. Previous studies have also shown that anemia was more common in HF-REF [20, 22, 24]. The present study showed that LVH was expected in HF-PEF, which is consistent with one of the previous studies stating that Cornell ECG criteria for the echocardiographic LVH had better performance than the Socolow [25]. BNP was higher in HF-REF than in HF-PEF that is also in agreement to the previous studies [26, 27]. The reason for high level in HF-REF is relates to precursor of BNP [28, 29]. Left ventricular ejection fraction (EF), left ventricular end-diastolic diameter (LVEDD), and left ventricular end-systolic diameter (LVESD) were significantly higher in HF-REF. The main diagnostic finding by Echocardiography and Doppler in HF-PEF were normal LVEDD, normal LVESD, higher posterior wall thickness, interventricular septum thickness and ratio of Left posterior wall thickness x2. However, there was no difference in the left ventricular mass index in both groups.
The patients with HF-PEF were less likely to receive angiotensin-converting enzyme inhibitors (ACEI), loop diuretics, or aldosterone receptor antagonist than patients with HF-REF. This is supported by few of the previous studies as well [11,15,18,20,21,23]. This might reflect a lack of evidence-based effective medication of HF-PEF. In contrast, calcium channel blocker and thiazide diuretic were used more in patients with HF-PEF, as compared to HF-REF. This clearly shows that these agents might be of benefit, especially for those with HF, hypertension, and calcium channel blocker may be harmful in HF-REF [11,18,21]. The present study showed that the use of Angiotensin II receptor antagonist (ARBs) was greater in those with HF-PEF, as compared to those with HFREF that is similar to one of the previous studies [30]. This could reflect the benefit of this therapeutic class suggested by the results of a previous study [31].
There is wide variation in the prognosis of patients with HF-PEF, as estimated rates of mortality and re-hospitalization are conflicting [30, 32]. However, the recognition of the associated risk of morbidity and mortality for these patients is increasing. In the Euro Heart survey, the incidence of all-cause Mortality during the 3-month follow-up period was 10%, and the need for re-hospitalization was 21% [18].
The present study was a cross-sectional non prospective study without follow-up data and it includes outpatients, who were at a low risk than hospitalized patients. As an observational study, the diagnosis of HF and the measurement of EF was not standardized or validated. The study collected nonrandomized data, and some information was missing or incomplete. The analysis was based on the presence of an EF value, and was not available for all patients.
The outpatient-based prospective cross-sectional study of symptomatic heart failure in Saudi Arabia revealed HF-PEF prevalence of 51% among all HF, with male preponderance, young age, and prevalent risk factors LVH, anemia, and LA area in HF-PEF patients. There is a need to develop safe and cost-effective methods for screening high-risk patients with multiple risk factors for the early detection and treatment of HF. Large scale Clinical trials across the Saudi Arabia are needed to identify risk factors and strategies of treatment. In the absence of evidence-based treatment of HF-PEF, the only option is the control of the prevalent risk factors in HF-PEF. In Saudi Arabia, it is hoped that the need for more organized research with combined effort from basic science and health care provider would be possible by raising the awareness of the medical community about HF-PEF and its risk factors.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
