
Research Article | DOI: https://doi.org/10.31579/2578-8965/254
1Obstetrician and Gynecologist at Ashmoun General Hospital, Ashmoun, Menoufia, Egypt.
2Senior specialist registrar family medicine, PHCSS -AlMizhar Health Center-Dubai Health, UAE.
3Resident physician Obstetrics and Gynecology, Latifa Hospital-Dubai Health, UAE.
4Specialist registrar Obstetrics and Gynecology, Latifa Hospital-Dubai Health, UAE.
5Physiology department, Faculty of Medicine, Al-Azhar University, Assiut, Egypt.
*Corresponding Author: Mohamed Zaeim Hafez, Obstetrics and Gynecology Department, Faculty of Medicine, Menoufia University, Menoufia, Shebin El-Kom 32511, Egypt.
Citation: Colleen M. McCully, Rehab B. Mohamed, Ahmed Abdalla HH, Mohamed Z. Hafez, (2025), Prevalence and Associated Factors of Breast Cancer Women’s Quality of Life, J. Obstetrics Gynecology and Reproductive Sciences, 9(1) DOI:10.31579/2578-8965/254
Copyright: © 2025, Mohamed Zaeim Hafez. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 26 December 2024 | Accepted: 31 December 2024 | Published: 06 January 2025
Keywords: breast cancer, quality of life, hospital anxiety, depression scale, FSFI
Abstract:
Background: Breast cancer is the leading cause of cancer deaths in women. (BC) is the second-most prevalent type of cancer overall and the most common malignancy in women. Around 2.1 million people received breast cancer diagnosis globally in 2018, and the disease claimed the lives of about 627,000 people. In the contemporary healthcare system, quality of life has become a key concern for evaluating people's subjective perceptions of their lives. There have also been reports of psychological effects such as anxiety, melancholy, dread, and a decline in life satisfaction. These outcomes adversely affect both health and quality of life (QoL).
Objective: to determine the Prevalence of breast cancer and the associated risk factors with QoL among women diagnosed with breast cancer (BC).
Methods: A cross-sectional study included 200 women patients with breast cancer admitted to Al-Azhar University Hospitals from April 2023 to October 2024. the quality-of-life index-cancer ranged from 17.54-24.12 with a mean of 21, 70±3.89.
Results: Out of the 200 patients who were allocated in the current retrospective study, 35 women with stage 1, 60 women with stage 2, and 50 women with stage 3 as well as 55 women with stage 4. While monthly income had a highly significant positive correlation with the quality of life in soccer (r=0.613, p=0.021) and (HADS depression, HADS anxiety, MFIS, PSQI total score, FSFI, IPAQ) there was a significant negative correlation between them. Cox-regression analysis indicated that the most important independent risk factors associated with breast cancer women’s quality of life were cancer stage. However, the duration of disease and cancer stage had a highly significant negative correlation with the quality-of-life score (r= -0.455, p=0.036) and (r= -0.392, p=0.39), respectively. Cox-regression analysis indicated that the most significant independent risk factors associated with breast cancer women’s quality of life were cancer stage (OR:2.45, 95%CI, 0.098-0.298, p=0.013), HADS depression (OR:2.812, 95%CI, 0.987-3.761, p=0.007), PSQI total score (OR:5.16, 95%CI, 2.54-9.21, p=0.006), and IPAQ (OR:1.09, 95%CI, 0.158-1.499, p=0.013).
Conclusions: QoL assessments could help professionals prioritize problems, communicate more effectively with patients, minimize adversity, and determine patient preferences. We discovered a bad quality of life among people with breast cancer under study. The stage of cancer, anxiety and despair scale, modified fatigue effect scale, and female sexual function index all had a substantial impact on breast cancer women's quality of life.
According to Xia et al., (2022), breast cancer is the primary cause of cancer-related mortality among women. Patients with breast cancer have had longer survival times in recent years because of advancements in medical technology and heightened knowledge of breast cancer self-examination (Thewes et al., 2012). The long-term uncertainty of their health condition before and after cancer treatment, however, can be a major psychological burden, since research has revealed that many cancer survivors suffer from a chronic fear of cancer recurrence (FCR) (Tong et al., 2024). Breast cancer (BC) is the second most frequent type of cancer worldwide and the most common cancer among women (Bray et al., 2020, Al-Sharman et al. 2024). Breast cancer has the greatest death rate and is the most common cancer diagnosed in women worldwide, according to statistics from the Global Cancer Observatory 2020 (Globocan Cancer Statics, 2021). However, 5-year net survival odds are typically more than 80% in high-income nations (Carreira et al. 2021).
On a worldwide scale almost 2.1 million people had a breast cancer diagnosis in 2018, and the disease claimed the lives of about 627,000 people (Bray et al., 2020). According to (Boquiren et al., 2013) and (Iddrisu et al., 2020), women with BC have several physical, psychological, and social repercussions. Physical effects of BC include fatigue, discomfort, lymphedema, sexual dysfunction, and sleep disturbances (Taghian et al., 2014; Schmidt et al., 2018). Moreover, psychological effects such as worry, melancholy, dread, and a decline in life satisfaction have been shown (Maass et al., 2019). Both health and quality of life (QoL) are adversely affected by these outcomes (Campbell-Enns and Woodgate, 2015).
Quality of life has become a prominent issue in the current healthcare system to assess the subjective perception of individuals’ life (Megari, 2013). Investigating QOL in people with chronic diseases as per BC may help improve patient health as it might guide policies, interventions, and services (Bamm et al., 2013). Furthermore, investigating QOL is very important for improving clinical research and clinical practice. However, the concept of QoL is not universally agreed upon; it has evolved, gaining depth across various fields (Fayers and Machin, 2013). Overall, several research from many countries have reported on the underlying contributing variables that may affect QoL among women with BC, and other factors have been presented (El Haidari et al., 2020). However, the factors related with QoL recorded in various European and North American studies may not be the same as those affecting QoL in Jordanian women with BC. This gap is caused by disparities in patients' goals, expectations, worries, religious beliefs, financial status, healthcare, and social systems.
To our knowledge, only minimal quantitative data on the quality of life of breast cancer patients in Arabian nations has been published using the ICF model. As a result, the purpose of this study was to determine the prevalence of breast cancer, and the risk variables related with quality of life among women who had been diagnosed with it.
Study design
A cross-sectional study included 200 women patients with breast cancer admitted to Al Azhar University Hospitals from April 2023 to October 2024. We included only women aged 18 or above and diagnosed with breast cancer. We excluded women who were unable to follow the instructions.
Interview questionnaire sheet
The research assistant conducted interviews with participants and completed the informed consent process before their enrolment in the study. All participants received detailed explanations about the study. Those who agreed to take part were invited to complete questionnaires in a serene, distraction-free environment. This setting aimed to enhance participants’ focus and encourage free and confidential responses. The investigator administered the questionnaires during face-to-face interviews. The information collected was categorized into impairment, activity, participation, and contextual factors. Impairment was assessed by the clinical characteristics of the BC (including the stage of BC, the onset of the diagnosis, and having surgery or not) and the presence of complications including depression, anxiety, fatigue, and sleep impairment). Physical activity level was assessed to reflect participation. Contextual factors include age, marital status, number of family members, educational level, income level (World Salaries, 2024), and employment status (whether they are employees or not).
All women with breast cancer were subjected to the following:
The Quality-of-Life Index-Cancer
The Cancer Quality-of-Life Index (QLI-c) is divided into two parts. Participants are asked about how satisfied they are with several areas of their lives in the first section, and the significance of those aspects is evaluated in the second. Better QoL is indicated by a higher total score, which goes from 0 to 30. For assessing the quality of life of clients who speak Arabic, the Arabic version of the Quality-of-Life Index is extremely dependable and has adequate content validity (Halabi, 2006; Omar and Alnahdi, 2023).
The Pittsburgh Sleep Quality Index
The Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality, it is a self-reported 19-item questionnaire about (subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction). Scoring for each item ranges from 0 to 3, where 0 indicates no difficulty, and 3 is severe difficulty. The total score of PSQI is calculated by combining seven domain scores, ranging from 0 to 21. A score ≤5 points considered good sleep quality, while a score of ˃5 considered as poor sleep quality (Suleiman et al., 2010). The Arabic version of the PSQI demonstrated adequate reliability and validity for assessing sleep quality in Arabic-speaking patients diagnosed with cancer (Al Maqbali et al., 2020).
The Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) was used to evaluate the level of anxiety and depression. It is a 3-point Likert-type scale consisting of 14 items, 7 items for each anxiety, and depression. The total score of each subscale is out of 21. A higher score indicates a high level of anxiety and depression. A score of ≥ 11 is considered a clinically significant disorder, whereas a score between 8 and 10 suggests a mild disorder (Spielberger, 2013; Stern, 2014). The Arabic version of HADS is reliable and valid (Terkawi et al., 2017).
Modified Fatigue Impact Scale
Fatigue was assessed using the Modified Fatigue Impact Scale (MFIS). The MFIS is a 21-item instrument that measures the impact of fatigue over the past 4 weeks on activities of daily living. FSFI covers three domains: physical, cognitive, and psychological. Respondent rate on a 5-point Likert-type scale is the frequency of fatigue symptoms within the past 4 weeks. Item rated from (0) never to (4) always. The score provides a total fatigue score with a range from 0 to 84. A higher score indicates greater fatigue symptoms, a score of 38 is considered the cut-off point for scoring (Lundgren-Nilsson et al., 2019). The valid Arabic version of MFIS was used in this study (Alawami and Abdulla, 2021).
Physical Activity Questionnaire
The International Physical Activity Questionnaire (IPAQ-short form) was used, which has 7 items assessing physical activity over the previous 7 days by asking about the number of days and hours people spent walking, performing moderate or vigorous levels of physical activity (Craig et al., 2003).
Ethics approval and consent to participate
All procedures were carried out by the 1964 Declaration of Helsinki and its amendments, including the ethical principles established by national and institutional research committees and comparable conventions. The study procedure was approved by the Faculty of Medicine's ethical council at Al-Azhar University (Assiut).
Sample size estimation
To detect the null hypothesis, a sample size of 200 patients would be required, with a drop-out rate of 10% and a research power of 80%. Bray et al., (2020) reported that approximately 2.1 million people worldwide were diagnosed with breast cancer, and approximately 627,000 people died from it.
Statistical analysis
The tabulated findings were statistically analyzed using Microsoft Excel 2019 and SPSS v. 25 (SPSS Inc., Chicago, IL, USA). Categorical variables are represented using relative frequency statistics, such as the independent t-test (t), Pearson correlation, and COX regression analysis. Statistical significance is defined as p < 0>
Figure 1 displays a flowchart of 213 women with breast cancer in our study; 13 patients were eliminated from the study due to incomplete questionnaire responses (8 patients and 5 patients did not match inclusion criteria). Out of the 200 patients who were assigned in the current retrospective analysis, 35 women with stage 1, 60 with stage 2, 50 with stage 3, and 55 with stage 4.

Figure 1: Flowchart of the studied women diagnosed with breast cancer.
Our study included 200 women diagnosed with breast cancer, ranging in age from 43 to 65 years, with an average of 48.32±11.07 years. We noticed that women with breast cancer whose duration of disease was >1 year widely distributed (105,52.5%) and whose length of disease was 6-12 months women who were subjected to surgery were more frequent (157,78.5%) than those who were not subject to surgery (43,21.5%). (Table 1). Also, Breast cancer in married women is more common (140.70%) than in others (60.30%). Working women are more numerous (148.74%) than those who do not work (52.26%)., (Figure 2). Figure 2 indicates that most of our women under study had stage II breast cancer (30%), followed by women with stage IV by 28% and those with stage III by 25%; nevertheless, women with stage I were the least prevalent by 17%. (Figure 3).
| Variable | Mean ± SD | Range |
| Age at diagnosis/year | 48.32±11.07 | 43-65 |
Duration of disease ˂6 months 6-12 months ˃1 year |
26 69 105 |
13.0% 34.5% 52.5% |
Surgery Yes No |
157 43 |
78.5% 21.5% |
Table 1: Demographic data among the studied women diagnosed with breast cancer (n=200).

Figure 2: Personal data distribution of the studied women diagnosed with breast cancer.

Figure 3. Distribution of breast cancer stages among the studied women.
In our study, the quality-of-life index for cancer ranged from 17.54-24.12, with a mean of 21.70±3.89 (Table 2). There was also no significant relationship between the Quality-of-Life score and the other variables evaluated (age at diagnosis, marital status, educational status, and employment status) (p > 0.05). Monthly income had a significant positive link with soccer quality of life (r=0.613, p=0.021), as shown in (Table 3).
| Mean ±SD | Median (Range) | |
| HADS depression | 7.23±5.11 | 7.56(3.65-11.98) |
| HADS anxiety | 8.10±3.21 | 8.2(6.2-11.4) |
| MFIS (unit) | 41.24±15.33 | 40.9 (26.10-57.30) |
| PSQI total score (unit) | 8.34±3.29 | 8.25 (5.90-12.01) |
| FSFI | 10.16±8.95 | 9.86 (4.89-19.15) |
| IPAQ | 5312±2670 | 5400 (2865-7366) |
| QLI-c | 21.70±3.89 | 21.2(17.54-24.12) |
QLI-c, Quality of Life Index-Cancer; HADS, Hospital Anxiety and Depression Scale; MFIS, Modified Fatigue Impact Scale; PSQI, Pittsburgh Sleep Quality Index; FSFI, Female Sexual Function Index; IPAQ, International Physical Activity Questionnaire
Table 2: Outcome among the studied women with breast cancer (n=200).
| Quality of life score | ||
| Pearson correlation (r) | P value | |
| Age at diagnosis/year | 0.014 | 0.810 |
| Marital status | 0.160 | 0.762 |
| Educational status | -0.105 | 0.820 |
| Occupational status | 0.041 | 0.933 |
| Monthly income | 0.613 | 0.021* |
QLI-c, Quality of Life Index-Cancer; HADS, Hospital Anxiety and Depression Scale; MFIS, Modified Fatigue Impact Scale; PSQI, Pittsburgh Sleep Quality Index; FSFI, Female Sexual Function Index; IPAQ, International Physical Activity Questionnaire
Table 3: Relation between quality of life and the studied variables.
The current study found no significant relationship between quality of life and surgery (p=0.812). However, the duration of disease and cancer stage had a highly significant negative connection with the quality-of-life score (r= -0.455, p=0.036 and r= -0.392, p=0.39), respectively (Table 4).
| Quality of life score | ||
| Pearson correlation (r) | P value | |
| Duration of disease | -0.455 | 0.036* |
| Cancer stage | -0.392 | 0.039* |
| Surgery | -0130 | 0.812 |
QLI-c, Quality of Life Index-Cancer; HADS, Hospital Anxiety and Depression Scale; MFIS, Modified Fatigue Impact Scale; PSQI, Pittsburgh Sleep Quality Index; FSFI, Female Sexual Function Index; IPAQ, International Physical Activity Questionnaire
Table 4: Relation between quality of life and characteristics of diseases.
The study found a substantial negative correlation (p<0>
| Quality of life score | ||
| Pearson correlation (r) | P value | |
| HADS depression | -0.599 | 0.011* |
| HADS anxiety | -0.738 | 0.001* |
| MFIS (unit) | -0.390 | 0.040* |
| PSQI total score (unit) | -0.522 | 0.012* |
| FSFI | -0.293 | 0.045* |
| IPAQ | -0.6.10 | 0.001* |
QLI-c, Quality of Life Index-Cancer; HADS, Hospital Anxiety and Depression Scale; MFIS, Modified Fatigue Impact Scale; PSQI, Pittsburgh Sleep Quality Index; FSFI, Female Sexual Function Index; IPAQ, International Physical Activity Questionnaire
Table 5: Relation between quality of life and presence of complications.
In the current study, Cox-regression analysis indicated that the most significant independent risk factors associated with breast cancer women's quality of life were cancer stage (OR:2.45, 95%CI, 0.098-0.298, p=0.013), HADS depression (OR:2.812, 95%CI, 0.987-3.761, p=0.007), PSQI total score (OR:5.16, 95%CI, 2.54-9.21, p=0.006), and IPAQ (OR:1.09, 95%CI, 0.158-1.499 ( p=0.013), (Table 6, Figure 4).
| B | SE | Wald | Sig. | Exp(B) | 95.0% CI for Exp(B) | ||
| Lower | Upper | ||||||
| Monthly income | -.109 | .701 | 0.04 | .098 | .0.130 | .004 | .675 |
| Duration of disease | .0223 | .855 | 0.60 | .102 | 0.140 | .1.050 | 1.932 |
| Cancer stage | -.764 | .011 | 6.093 | .013* | 2.450 | .098 | .2.980 |
| HADS depression | 1.09 | .042 | 4.110 | .007* | 2.812 | 0.987 | 3.761 |
| HADS anxiety | -.809 | .721 | .0310 | .955 | .201 | .022 | 0.144 |
| MFIS (unit) | -.982 | .932 | 1.04 | .076 | .914 | .811 | 1.320 |
| PSQI total score (unit) | .0855 | .002 | 4.321 | .006* | 5.16 | 2.540 | 9.210 |
| FSFI | -.0110 | .502 | .037 | .882 | .021 | .015 | 0.946 |
| IPAQ | -.418 | .012 | 3.660 | .013* | 1.09 | .1580 | 1.499 |
QLI-c, Quality of Life Index-Cancer; HADS, Hospital Anxiety and Depression Scale; MFIS, Modified Fatigue Impact Scale; PSQI, Pittsburgh Sleep Quality Index; FSFI, Female Sexual Function Index; IPAQ, International Physical Activity Questionnaire.
Table 6: Cox regression analysis of the risk factors associated with Breast Cancer Women’s Quality of Life.
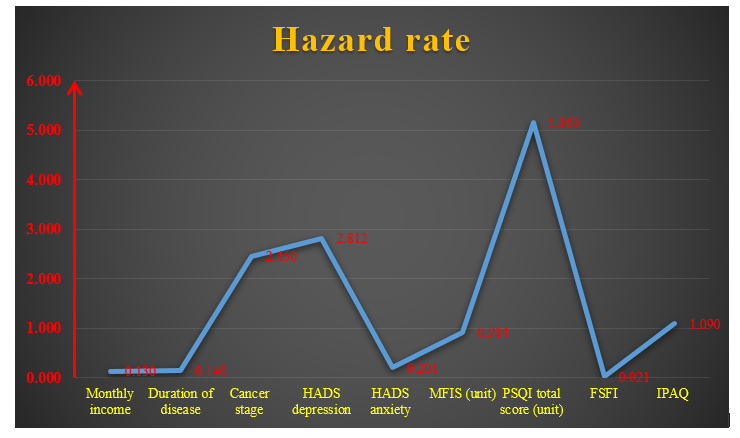
Figure 4: Hazard risk distribution associated with Breast Cancer Women’s Quality of Life.
Today, quality-of-life surveys are a significant healthcare concern, particularly in oncology research. Cancer has a wide-ranging impact on quality of life and is today a serious global issue. Patients have physical and emotional challenges during the diagnosis, early stages of treatment, and months after therapy completion (Rahman et al., 2014). During these times, breast cancer patients may experience poor adjustment and a lower quality of life. As a result, healthcare practitioners must understand how a breast cancer diagnosis and treatment affect a patient's quality of life (Engel et al. 2003; Theofilou, 2012). To our knowledge, only minimal quantitative data on the quality of life of breast cancer patients in Arabian nations has been published using the ICF model. As a result, the purpose of this study was to assess the prevalence of breast cancer, and the risk variables related with quality of life among women who had been diagnosed with it. In our study, the Quality-of-Life Index-Cancer varied from 17.54-24.12, with a mean of 21.70±3.89, little lower than in previous studies. In research conducted in Brazil using the same questionnaire, the mean scores were higher than 65 in all domains. Though not comparable because other questionnaires were used to assess QOL, a Malaysian study revealed a mean global health status of 65.7, which most likely represented domains 1 and 2 in the WHOQOL-BREF (Ganesh et al., 2016). A systematic evaluation of QOL in Arab breast cancer patients revealed mean scores ranging from 45.3 to 74.6 (Rahou et al., 2016). The mean score, however, was found to be 42.2 in one of the Indian investigations by (Kannan et al., 2011), and 77.93 in another research of individuals younger than 35 years (Damodar et al., 2014).
Our study found an extremely substantial positive link between monthly income and soccer quality of life (r=0.613, p=0.021). A Korean study by (Fang-Rong et al., 2012) found that lower income is associated with decreased QOL. Patients with higher incomes were more likely to have better access to knowledge and tools for issue solutions, as well as stronger coping abilities, which may explain the higher QOL among women with higher socioeconomic status. As a result, decreased income may have an impact on breast cancer patients' quality of life (Fang-Rong et al. 2012). (Rahman et al., 2014) observed that cancer survivors' QOL was influenced by both socioeconomic difficulties and cancer concerns. Lower family income, nutritional status, occupation, and age have a greater impact on QOL following mastectomy in breast cancer patients in this study. Everyone has a bad impact. Higher monthly income was found to be positively associated with scores in the psychological, social relationship, and environmental categories of QOL, which is consistent with previous research. (Yan et al., 2016; Broeckel et al., 2000; Kannan et al. 2011) Higher income has been associated to many features of improved patient care, including faster treatment, access to better rehabilitation, and less concern about the financial consequences of treatment and absence from work (Yan et al., 2016). Al-Naggar et al. (2011) discovered a substantial link between family monthly income and overall QOL. Our earlier study found that family monthly income has a significant impact on overall quality of life (Rabin et al. 2008). The findings are like a prior study by (Ganz et al., 2002) found that income was a strong predictor of QOL. Merkin et al., 2002) also observed that poor income hindered access to primary preventive interventions and early detection of breast cancer. This current study was also consistent with (Uzun et al., 2004), who discovered that women with intermediate income had a higher total QOL. Esbensen et al., (2004) observed a similar conclusion, indicating that a bad economy is related to a low quality of life. Pandey et al., (2006) found that family income has a substantial influence on overall quality of life. Another study from China confirmed this finding, showing that wealth was highly associated with overall QOL (Lu et al. 2007). This is most likely because income may have had interacting impacts. These findings, however, contradicted a study conducted by Pinar et al., (2003), which revealed no effect of financial position on quality of life.
In our study, disease duration and cancer stage were found to have a highly substantial negative connection with quality-of-life scores. Women with early-stage breast cancer are twice as likely to be depressed as the general female population, particularly in the first year after diagnosis (Anna et al., 2013). Including the ICF evaluation in the standard psychological examination allows for a more comprehensive knowledge of the psychological-clinical implications (Anna et al., 2013). Fang-Rong et al., (2012) discovered that advanced-stage cancer and poorer income are linked to reduced QOL. Advanced-stage cancer is associated with increased pain, chemotherapy treatment, intense physical activity, and psychological issues. As a result, advanced stage disease and poor income may have an impact on breast cancer patients' quality of life (Fang-Rong et al. 2012). However, another study by Gangane et al., (2017) found no association between patient delay, clinical stage, and QOL, as did our study. While no other studies have investigated patient delays, multiple studies have found no link between disease stage and quality of life (Yan et al., 2016; Ashing-Giwa et al., 1999). One possible explanation is that most of these studies have just looked at the illness stage; a more thorough investigation, including treatment regimen and the clinical stage of the disease that correlates with QOL, may be required to detect a line. In our study, the quality-of-life score had a significant negative correlation with HADS depression, HADS anxiety, MFIS, PSQI total score, FSFI, and IPAQ. Our findings align with those of KOÇ et al., (2024), who found that telehealth programs in women with breast cancer reduced fear of relapse, depressive symptoms, distress, intrusive thoughts, anxiety, sleep disorder, insomnia, improved quality of life, cognitive functions, psychological strength, and sleep quality. Furthermore, research showed that these programs improved psychological health, functionality, optimism and control over the future, pleasant mood and life enjoyment, and drug compliance. Furthermore, depression was a strong predictor of both general and QoL. Furthermore, breast cancer patients with menopausal symptoms and low emotional well-being were more likely to experience anxiety and sadness (Han et al., 2019; Shim et al., 2020). These findings underlined the importance of psychosocial support programs for BC women's psychological well-being, which may improve their quality of life. These findings highlight the need of psychosocial support programs designed to improve the psychological well-being of women with breast cancer. These activities may include a variety of supporting measures such as counseling, therapy sessions, support groups, and educational programs targeted at addressing the emotional and psychological issues that women with breast cancer encounter (Hodge and Lonsdale, 2011; Turner et al., 2011). Incorporating exercise into these programs could considerably reduce emotional distress and improve overall QoL in this population (Burke et al. 2012).
Exercise not only relieves psychological issues, but it also improves physical well-being by boosting mood, lowering stress, and enhancing mental health (Durosini et al., 2021). Park and Yoon, (2013) found a substantial relationship between BC women's sexual function and QoL. Safarinejad et al., (2013) found comparable results in their research of 390 women with BC. One possible reason for these findings is the interplay of BC medication, a lack of sexual desire and attractiveness, and poor partner interactions. A recent study discovered that decrease in sexual QoL in BC patients related to greater anxiety and depression levels, body image disturbance, and lower self-esteem (Brajkovic et al., 2021). Furthermore, poor social support from spouses negatively impacts sexual quality of life in breast cancer patients (Brajkovic et al., 2021). As a result, these data imply that tailored therapies to promote sexual function may aid in sexual health recovery and quality of life in women with BC. These findings support the findings of a prior Korean study, which found that depression was negatively related with QoL (Han et al., 2019). Another study conducted by Hsiao et al. in 2019 discovered that high anxiety and depression symptoms related to overall QoL degradation in Chinese BC women.
In the present study, the most significant independent risk factors associated with breast cancer women’s quality of life were cancer stage (OR:2.45, 95%CI, 0.098-0.298, p=0.013), HADS depression (OR:2.812, 95%CI, 0.987-3.761, p=0.007), PSQI total score (OR:5.16, 95%CI, 2.54-9.21, p=0.006), and IPAQ (OR:1.09, 95%CI, 0.158-1.499, p=0.013). This study highlights the significance of long-term issues faced by women with breast cancer and their impact on their quality of life. Understanding the association between various impairments (such as sleep quality, sexual function status, and anxiety and depression status) and QoL would enable healthcare practitioners to provide tailored interventions to women who are at high risk of poor QoL. These findings highlight the importance of doing larger-scale longitudinal investigations of demographics, behavioral, social, and clinical aspects that connect with QoL in various breast cancer groups. The ICF remains an important tool for determining how well BC survivors are doing in their recovery (Pinto et al., 2022), Al-Sharman et al., (2024) conducted a multiple regression analysis and found that sexual dysfunction, poor sleep quality, sadness, and anxiety were significant predictors of QoL (p<0>
It's also important to note some limits. Because most of the interviews took place in the patients' homes, certain responses particularly those pertaining to social relationships may have been hampered by the lack of privacy. No data on co-morbidities was gathered, which would have affected the patients' quality of life. The WHOQOL questionnaire is not available in Arabic, which may be another drawback.
Professionals may find that QoL assessments help them prioritize issues, communicate with patients more effectively, avoid adversity, and determine patient preferences. We observed that women with breast cancer in the study had a poor quality of life. The Pittsburgh sleep quality index, physical activity, anxiety, depression scale, modified tiredness impact scale, female sexual function index, cancer stage, monthly income, and length of disease were all strongly correlated with the quality of life of women with breast cancer. Patients with breast cancer should receive a lot of treatment that includes social monitoring and support from the right social groups and agencies.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
