
Research article | DOI: https://doi.org/10.31579/2693-4779/119
1 Department of Genetic Engineering and Biotechnology. School of Life Sciences, Shahjalal University of Science and Technology, Sylhet, Bangladesh.
2 Department of Pharmacy, Daffodil International University, Dhaka, Bangladesh.
3 Department of Internal Medicine, Jalalabad Ragib Rabeya Medical College and Hospital, Sylhet, Bangladesh.4 Department of Cardiology, MAG Osmani Medical College and Hospital, Sylhet, Bangladesh
*Corresponding Author: Riyan Al Islam Reshad, Department of Genetic Engineering and Biotechnology. School of Life Sciences, Shahjalal University of Science and Technology, Sylhet, Bangladesh.
Citation: Sayedatun Nesa Sumaia, Riyan Al Islam Reshad, Fawzia Tabassum, Sabrina Khan Mim, Mohammad Golam Rob Mahmud. Et all, (2023), Present Status of Newborn Screening in Bangladesh through the Participation of Health Professionals Clinical Research and Clinical Trials. 7(1) ; DOI :10.31579/2693-4779/119
Copyright: © 2023 Riyan Al Islam Reshad, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Received: 18 October 2022 | Accepted: 21 November 2022 | Published: 16 January 2023
Keywords: motion analysis; joint torque; range of motion; biomechanical measurements
This paper suggests a biomechanical analysis of the joint motion of the arm based on the 3-dimensional motion analysis technique in the steering wheel action. The three-dimensional motion trajectory of the arm is obtained using the motion capture system, and the inverse kinematic analysis and inverse dynamics analysis are performed on the musculoskeletal model of the arm using this result. By doing this, the displacement of the arm joint and the magnitude of the joint torque are calculated. The rotational motion of each joint occurs simultaneously and in the joint motion, it can be confirmed that pronation-supination of the elbow joint, adduction-abduction of the shoulder joint, flexion-extension and flexion-extension of the wrist joint are the main movement parameters.
Using this biomechanical motion analysis of joint segmental range of motion, it can be extended to analyze the behavior of passengers indoors in the autonomous vehicles.
Newborn screening is a simple test that can be used to identify healthy babies shortly after they are born. NBS enables healthcare professionals to detect and treat the certain disease before they cause a newborn to get sick. The goal of NBS is to find potentially fatal or disabling abnormalities in infants as soon as possible, usually before the baby shows any signs or symptoms of the disease or condition. Because of the early detection, treatment can begin immediately away, reducing or even eliminating the repercussions of the disorder. Many of the disorders found during newborn screening can cause lifelong nervous system damage, intellectual, developmental, and physical problems, as well as death if left untreated. NBS is a well-established program in developed countries as well as several Asian countries for the early detection of numerous avoidable diseases. With the control of contagious and communicable diseases under control, the Bangladesh government is now focusing more on health prevention [1]. In Bangladesh, newborn screening began in 1999. The initiative began as part of an International Atomic Energy Agency (IAEA) regional project to screen for congenital hypothyroidism (CH). The IAEA initially provided equipment, filter papers, reagents, training, and expert services to the country. Two pilot initiatives to test babies for CH have been performed since 1999. 30,000 babies were screened as part of these projects, and 16 were found to have hypothyroidism [2].
In July 2006, the Bangladesh government approved a national campaign to screen infants for CH in a few designated districts of the country. 200,000 infants will be screened as part of the program, and laboratory facilities for NBS will be expanded. Bangladesh has a population of 140 million people. Every year, over 2 million new babies are born at the current birth rate. The country's socioeconomic position is also distinctive. The country's per capita income is among the lowest in the world. Approximately 85% of babies are still born at home [3]. As a result, Bangladesh faces a significant problem in terms of neonatal screening. However, the country should make every effort to overcome these obstacles [4].
Many cross-sectional studies have already been conducted in several different countries throughout the world to study the attitudes of the general public concerning the circumstances for which NBS is available, including in North America [5-12], Europe [13], the Middle East and North Africa [14-18], Asia Pacific [19-23] and India [24]. However, newborn screening practice is relatively limited in Bangladesh, even though the program has already been initiated (Hasan, Nahar, Moslem, & Begum, 2008). Therefore, this study aimed to look at the present scenario of newborn screening through the contribution of health professionals' knowledge, practices, and attitudes concerning newborn screening in different parts of Bangladesh.
Bangladesh has relatively limited newborn screening procedures, even though the program has already been initiated [4]. Few activities have already been conducted in the Department of Genetic Engineering and Biotechnology at Shahjalal University of Science and Technology, Sylhet, Bangladesh considering the detection and mutation patterns of sickle cell anemia, thalassemia, hemophilia, and chromosomal disorders in the lab condition [25-30]. However, newborn screening awareness has not progressed in terms of socio-economic aspects. Many surveys have already been conducted in different parts of the world to demonstrate parental or health professional participation, knowledge, attitude, consent time, cost, consent format, and perception of NBS [31]. Therefore, this study aimed to investigate health professionals' knowledge, practices, and attitudes concerning newborn screening in different parts of Bangladesh.
2.1 participants and procedures
A cross-sectional internet survey was conducted, and a convenience sampling technique was used to draw the sample from a different region of Bangladesh. This online engagement was held to collect information from participants to avoid alienation during Covid-19. Individuals are required to be health professionals from all around Bangladesh, according to the participants' requirements. After obtaining informed consent, 281 health professionals were interviewed, and their data were analyzed. Participants were informed about the procedure and purpose of the study and the confidentiality of information provided. Every participant consented willingly to be a part of the study during the interview period.
2.2 Measures
The questionnaire containing informed consent along with three sections i.e., Participants' characterization, knowledge, and attitude were utilized to collect data during the interview period.
2.3 Survey Utensils
In this study, the respondent was categorized by their gender (male/female), their occupation (Doctor/Medical student/Nurse/Medical Science related people/others), and their working institution type (Government/Non-Government).
Participants’ knowledge, attitude, and hospital facilities toward the NBS were measured using a total of 15 items structured questions (including the accessibility, and economic feasibility of this process) based on other prior studies conducted in Bangladesh as well as other countries. A pilot study was conducted before the inauguration of the final data collection. The knowledge section was comprised of 8-item option-based questions concerning the present condition of NBS in Bangladesh (hospital facilities) and health professional perspectives towards NBS. The attitudes section included 5-item questions about NBS (e.g., “What do you think about the parents act towards Newborn Screening?” etc.). The economic feasibility section questions concerning cost-effectiveness and cost estimation were also included there (e.g., “What do you think about the cost-effectiveness of NBS in Bangladesh?). All option of those answers was coded by a number (i.e., “Yes was coded as 1”, “No was coded as 2”, and “Maybe was coded as 3”).
2.4 Statistical Analysis
All data were coded and analyzed using two statistical software packages (Microsoft Excel 2019, and IBM SPSS Statistics version 25). Microsoft Excel was used to perform data cleaning, coding, editing, and sorting. An excel file including all variables was imported into SPSS software. Descriptive statistics (e.g., frequencies, percentages, etc.) and some first-order analysis by Cross tab (e.g., Chi-square tests, Fisher’s Exact test) were performed using SPSS software. Those tests were performed to examine the significant relationship between categorical variables and estimate their significance level. In addition, multiple response analysis was performed to define “multiple response sets” which shows the facilities of the hospital toward NBS.
2.5 Ethical Consent
All procedures of the present study were carried out following the principle of human investigation (i.e., Helsinki Declaration). Furthermore, the study was conducted under the ethical guidelines of the Institutional research ethics committee. Formal ethics approval of this research protocol [Reference Number: IEC-101(1)003] was granted by the institutional Ethical Review Board (ERB) of Shahjalal University of Science and Technology, Sylhet-3114. Participants were informed about the procedure and purpose of the study and the confidentiality of information provided. Every participant consented willingly to be a part of the study during the interview period.
3.1 general characteristics of participants
a total of 281 participants were included in the final analysis among them 59% were male and 41% were female (Table 1). Of all participants, 29.9% were doctors, 55.9% were medical students, 7.8% were nurses, 3.6% were medical science-related department students and 2.8% were other health professionals (Table 1). Among male participants, 63 people were working in government institutions and 83 people were working in non-government (private) institutions. Of Female participants, 52 people were working in government institutions and 83 people were working in non-government (private) institutions (Figure 1) In total, 48% were government medical working health professionals and 52% are non-government medical working health professionals (Table 1).
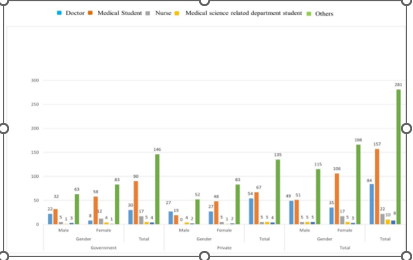
Figure 1 : General Characteristics of Participants

Table 1: Characteristics of participants
3.2 Knowledge About Nbs in Bangladesh Among Participants
The knowledge level of Health Professionals on NBS was mainly categorized into three groups that are good knowledge, poor knowledge
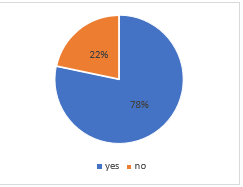
whilst few people would simply give a response to these survey questions by “may-be”, when they are confused about their answer or not sure. In general, 78% of participants had heard of newborn screening earlier, whereas 22% had never heard of it before (Figure 2).
Figure 2 : Percentages of heard about NBS
Different knowledge level was observed in association with Gender, occupation, and working institution (Table 2). In respective of gender, the knowledge level of Newborn screening was better among males than the female (79.1% for male participants and 77.7% for the female participants). On the other hand, by comparing the medical sector (both Government and Private), we found that private medical working health professionals have better knowledge (79.3%) than government medical working health professionals (77.4%). But this relationship was not significant. The Present occupation had a significant relationship with knowledge (p<0>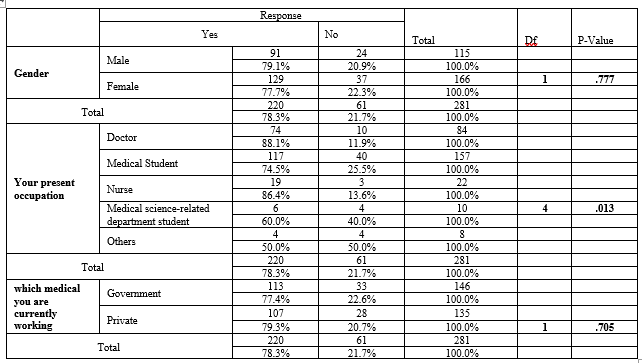
Table 2: Relation between participant general characteristics with heard about NBS
Disclaimer: If you do not wish to receive any email from us, please give a reply as Unsubscribe
3.4. Views of Hospital Facilities in Bangladesh for NBS
We also analyzed the Hospital condition in Bangladesh (how the tests are done, how the samples are collected, which diseases are screened etc.). But for this, firstly we need to examine the condition of hospitals in Bangladesh. Is NBS available or not in these particular hospitals (Table 3), these hospitals keep the records of NBS or not.
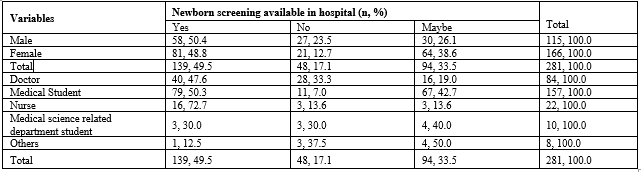
Table 3: Screening availability of newborns in Bangladesh Hospitals utilizing characteristics of the respondents
There were 44.5% of Government medical keeps records of Newborn Screening which was higher than Private medical 39.3% (Table 4). Chi-square analysis was done to assess the significant relationship between the types of medical you are currently working on and is your medical keeps the record of Newborn screening. The P-value is .029 which is >.05.
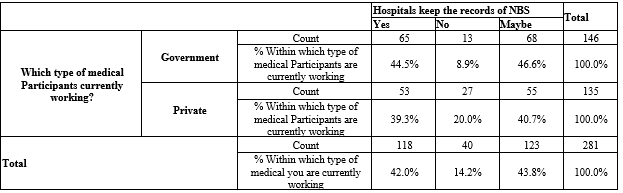
Table 4: which type of medical you are currently working * your hospital keeps the records of NBS cross-tabulation
Multiple response analysis was done to know about the hospital facilities toward NBS and to exhibit the rate of what kind of tests were done for NBS and which diseases were screened by NBS (Table 5, Table 6). Blood tests were mostly done for NBS in the Hospital of Bangladesh (31.6%) also many other tests were performed. (Table 5). As well as we can identify that Congenital Hypothyroidism disease was mostly screened by NBS (18.7%) also many other diseases were screened by NBS (Table 6).

Table 5: Frequencies of tests which were done for NBS
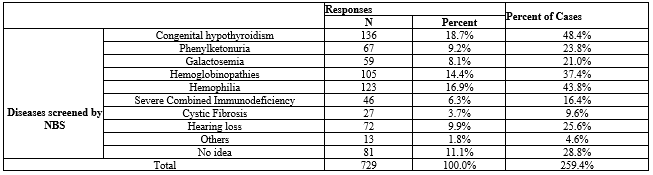
Table 6: Frequencies of diseases that were screened by NBS
From the perspective of occupation and working institution, we observed different types of tests that are done for NBS. These percentages and total are based on our responses (e.g., Doctors who were working in the Government hospital thought that 34.7% of Blood tests, 24.5% for Pulse Oximetry tests, 18.4% for Hearing tests, 8.2% of other tests are done for NBS in their hospital and 14.3% doctors have no idea what kind of tests are done
in their hospital) (Table 7). From the perspective of a working institution, different type of diseases is screened by NBS. These percentages and total are also based on our responses (e.g., Congenital Hypothyroidism was screened in Government hospitals at 18.8% and in Private hospitals at 18.5%) (Table 8)
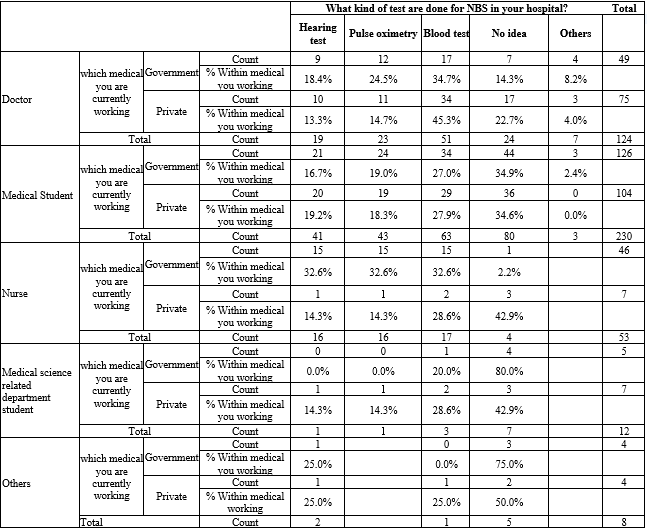
Table 7: Multiple response analysis for what kind of tests is done in the hospitals of Bangladesh
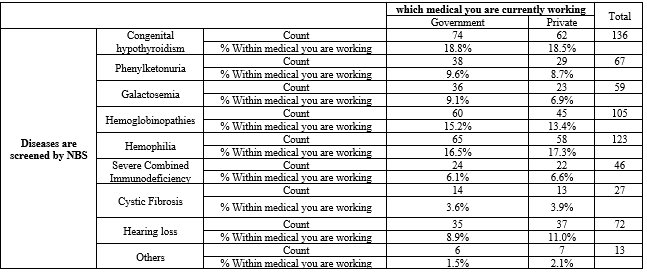
Table 8: Multiple response analysis for which diseases are screened in the hospitals of Bangladesh
3.5 Cost Analysis for NBS in Bangladesh
Cost is a great factor in establishing NBS for Bangladesh like poverty experienced in a developing country. The attitude toward the cost-effectiveness of Newborn screening was observed in association with the present occupation. Different thoughts about cost-effectiveness are shown in Figure 3. Among all the participants, medical students thought it was more cost-effective. Also, Occupation had a significant relationship with the cost-effectiveness of Newborn screening (p<0>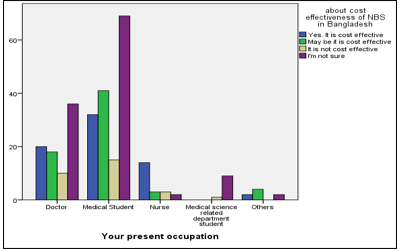
Figure 3: Relation between occupation and cost effectiveness of NBS in BD
The purpose of this study was to get a better understanding of newborn screening procedures and to provide information regarding newborn screening knowledge, views, and access among Bangladeshi health professionals. This study's contribution, we believe, will be not only in determining what health professionals know and don't know about newborn screening, how the tests are performed, which diseases are screened by NBS, and the importance of NBS, but also in understanding why some of them don't know about these issues and the possibility of developing an approach to enhance education and awareness among health professionals and expand the hospital's facilities for prophylactic screening.
Several countries have taken different tactics, and the situation varies widely around the world. In North America, each state has its screening process, including a minimum IEM. However, there is no agreement in the European Union concerning which IEMs should be screened [32]. For the past 50 years, Australasia has had an effective newborn screening program. Phenylketonuria, hypothyroidism, galactosemia, and cystic fibrosis were initially screened for, with even more recently expanded screening for fatty acid oxidation disorders, amino acid disorders, as well as organic acidemias’. All Australasian laboratories currently screen for more than 25 disorders [33]. Screening for seven genetic abnormalities, including four IEM, was made mandatory in the Spanish National Health System in 2013. PKU (phenylketonuria), MCADD (medium-chain acyl-CoA dehydrogenase deficiency), LCHADD (long-chain 3-hydroxy acyl-CoA dehydrogenase deficiency), and GA-1 (glutaric aciduria type 1). Yet, in practice, NBS is dictated by regional regulations, therefore there is a lack of consistency in testing for abnormalities at birth across the country. In 2011, the Community of Madrid launched an extended NBS (ENBS) with MS/MS, which included 17 metabolic disorders [34]. In this study, our participants responded by mentioning which diseases are currently being screened in Bangladesh. Congenital hypothyroidism, Phenylketonuria, Galactosemia, Hemoglobinopathies, Hemophilia, Severe Combined Immunodeficiency Syndrome, Cystic Fibrosis, hearing loss, Congenital heart disease, Microcephaly, Hydrocephalus, Down syndrome, Neonatal jaundice, LBW, Congenital Heart Diseases, and others are among the diseases on the list. Congenital Hypothyroidism (18.7%), Hemophilia (16.9%), Hemoglobinopathies (14.4%), Hearing Loss (9.9%), Phenylketonuria (9.2%), Galactosemia (8.1%) are among the most frequently tested disorders, according to our participants.
In the United States, all states take blood samples from newborns to conduct screening tests. These specimens or sections of them (often known as blood spots) are typically preserved for a length of time. At the moment, each state decides what happens to each blood sample after the screening tests. It is exceedingly difficult to acquire accurate national data because newborn screening regulations vary among states. Different nations' protocols differ in many ways, including specimen collection, diagnosis, organization, follow-up, and therapy. The NBS program is implemented in Spain, as it is in other European countries such as Belgium, Bosnia, Germany, Italy, and the United Kingdom. The Newborn Bloodspot Screening Working Group (NBSWG) was created by the Standing Committee on Screening in 2014 to produce a national policy framework for newborn screening in Australia [35]. National programs in New Zealand, the United States, the United Kingdom, Canada, and the Netherlands are being examined as possible precedents. The NBSWG's main task is to provide an evidence-based decision-making framework for determining whether conditions should be added to or removed from the newborn screening panel [7]. The results of the investigation indicated the current state of newborn screening in the hospital. When we examine the responses of the participants, we see that several tests were performed for newborn screening. Hearing test, Pulse oximetry test, Blood test, Karyotyping, Echo, Anomaly scan, X-Ray Arm/Leg, Blood grouping, CRP, S. Electrolytes, S. Creatinine, S. Calcium, CBC, S. Bilirubin, LXL, Portable CXR, and others are some of the tests available. The majority of individuals in this research said that blood tests are usually done for NBS (31.6%). Pulse oximetry (19.4%) and hearing tests are also conducted frequently. The majority of participants also stated that the preponderance of blood samples was acquired by heel prick (26%) and cord blood (14%) (25.3 %). As a result, we looked at the percentages of those tests and illnesses that were screened at various hospital types to determine our hospital condition for newborn screening. This survey confirms earlier research, which has consistently revealed highly positive attitudes towards NBS. NBS is seen as a regular element of the birthing process, with minimal discussion among HCPs and parents. In Bangladesh, there is currently an inadequate study on newborn screening. As a result, there is currently insufficient information available on the internet. Health professionals' Knowledge, Perspectives, Practices, and Hospital Facilities are critical in a resource-constrained nation like Bangladesh. By analyzing the data, this study contributes new information. Further research into these findings might give insight on aspects of the research that assist parents to become more conscious and make more informed decisions, as well as promote an understanding of NBS programs and save many children's lives.
Robert Guthrie, a researcher in the United States who is commonly regarded as the "father of newborn screening," pioneered newborn screening in the 1960s. Since descriptive research on how the offer of NBS is conveyed to parents is lacking, determining the experience of consent in practice is challenging. Understanding the perspectives of people who have directly participated in the consent process may provide useful descriptive data for NBS programs and providers [36].
This study looks into how parents act differently. Its affordability can play a significant role in making it more accessible. Even parents who are not well-off are interested in having their baby checked, provided it is cost-effective. The understanding and awareness of newborn screening methods among parents and professionals were minimal. Parents preferred concise, to-the-point information about newborn screening and its advantages, as well as the possibility of retesting and the significance of returning for retesting as soon as possible if the initial reports were abnormal. Parents, providers, and newborn screening providers all agreed that a simple, easy-to-read pamphlet with contact information would be beneficial. Parents should get this information before the baby is born, ideally in the third trimester of pregnancy, according to all focus group members. Providers requested a quick summary of information and tools to help them prepare for effective parent education [37].
Bangladesh is a growing country with so many additional problems to contend with. The global newborn screening program is a huge undertaking for a nation like Bangladesh. Finding adequate funding to carry out such a program will be the most difficult challenge. Another big obstacle is the social norm, which still sees over 80% of deliveries done at home. On the other hand, the enthusiasm of medical experts and the government is a very promising indicator in the direction of developing a newborn screening program. It now requires worldwide community collaboration. For a country like Bangladesh, the worldwide newborn screening program is a huge undertaking. The most challenging task will be obtaining sufficient financing to carry out such a program. Another significant big obstacle is the social norm, which still sees over 80% of deliveries made at home. On the other hand, medical professionals and the government's enthusiasm is a very encouraging indicator that a newborn screening program will be developed. It now requires global community cooperation.
and access to newborn screening. One of the variables that may contribute to a greater incidence of the disease reported in Bangladesh is a lack of awareness that leads to non-participation in screening. Action is needed at the levels of medical education, clinical care, health policy, and information systems to address this issue. Streamlined access to NBS results for parents and medical professionals, low-literacy information for parents, and clear communication guidelines for providers with guidance on how to properly communicate NBS results to parents are some of the potential solutions. The relevance of community knowledge and mobilization in the implementation of a newborn screening program is highlighted in this study. To increase screening uptake, all newborn screening programs must include a major teaching component. With the expansion of the NBS, there will be more opportunities to promote public health systems and improve child health screening and information. NBS in the population is a challenge that can be overcome by collaborating and working with the media and the use of e-health technology. Subsequently, wide-ranging awareness programs should be introduced among the general population, especially among women of childbearing age and their families, creating a demand, followed by a screening program that is accessible and cost-effective. To assemble diagnosed cases of NBS from both public and commercial health facilities across the nation, we must create a nationwide database. This will be the first step in ascertaining the general burden of NBS. This initiative will help inform the inception of a national newborn screening mechanism. Physicians will be required to come forward and contribute to this cause in collaboration with Ministry of Health initiatives.
We acknowledge the participants for providing the information and support to conduct this research. Also, we are thankful to the Department of Genetic Engineering and Biotechnology of Shahjalal University of Science and Technology, Sylhet-3114 for their support.
For this study, no research grants were received from funding agencies in the public, private, or non-profit sectors.
No potential conflict of interest
This work was a collaboration among all the authors. MFM, SNS and RAIR designed outlines of the manuscript. SNS and RAIR wrote the initial draft of the manuscript. SNS, RAIR, FT, SKM collected the data. MGRM, CMOF and MFM reviewed the scientific contents described in the manuscript. All authors read and approved the final submitted version of the manuscript.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
