
Research Article | DOI: https://doi.org/10.31579/2639-4162/158
1 University Medical Sciences Sancti Spíritus Department of Postgraduate and Research. Holy Spirits, Cuba.
2 Sancti Spiritus Provincial Center for Hygiene and Epidemiology, Sancti Spiritus, Cuba.
3 Sancti Spiritus Provincial Health Sector, Cuba.
*Corresponding Author: Adrian González Méndez, Department of Postgraduate and Research, University of Medical Sciences of Sancti Spiritus, Cuba.
Citation: Adrian G. Méndez, Perez Flowers CM, Yesneris B. Lizano, Niuvis F. Martin, Laida G. Matos , (2024), Preparation Of Families of Children Diagnosed with Spastic Childhood Cerebral Palsy for the Development of Occupational Therapy, J. General Medicine and Clinical Practice, 7(5); DOI:10.31579/2639-4162/158
Copyright: © 2024, Adrian González Méndez. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 07 March 2024 | Accepted: 15 March 2024 | Published: 19 March 2024
Keywords: cerebral palsy; preparation of families; occupational therapy
Introduction: Infantile cerebral palsy is one of the 3 most common developmental disabilities that prevail throughout life. It cannot be defined as a single disease, but is a syndrome that encompasses a group of heterogeneous disorders.
Objective: To assess the preparation of families of children diagnosed with spastic infantile cerebral palsy.
Methods: An intervention study was carried out in nine families with children diagnosed with Spastic Infantile Cerebral Palsy, from zero days old to five years and eleven months with prior consent belonging to the Dr. Juan Miguel Martínez Puentes Polyclinic in the northern area of the Province of Sancti Spiritus, Cuba.
Results: In this study, it was possible to obtain an increase in the knowledge necessary for the nine families with children diagnosed with Childhood Spastic Cerebral Palsy to manage it since one (77.8%) knew the role of the family in the development of occupational therapy, one (88.9%) learned about the stimulation of communication in the family context and one (77.8%) became aware of the importance of preventing deformities in this group of children.
Conclusions: Related to assertive parental communication, it was stated that the category that had the most relevance was the use of respect, attention and trust, in passive parental communication it was noted that there is no organization to carry out family activities
Infantile cerebral palsy (ICP) is one of the three most common developmental disabilities that prevail throughout life. It cannot be defined as a single disease, but rather as a syndrome that is characterized by a group of persistent disorders of the development of movement and posture, which cause limitation in activity and are attributed to non-progressive, non-immutable lesions that occur in the immature brain due to pre-, peri- or postnatal injury. [1]
The global prevalence of cerebral palsy (CP) is around 1.5-3/1,000 live births. A study carried out in 2007 estimated a global prevalence of 2.4/1,000 live births. Thanks to current studies, it can be stated that this prevalence, currently estimated at 2.1/1,000 live births, has remained stable over the last 10 years. 1 In Cuba, the prevalence of CP is between 1.5 and 3 per 1,000 live births, and is usually classified as congenital or acquired, according to the time of occurrence of the brain damage. [2]
Spasticity and limitation in the execution of voluntary movement are the most frequent sequelae and affect the child's gross motor skills. According to the Gross Motor Function Classification Extended and Revised (GMFCS-ER), cerebral palsy is classified into five levels from highest to lowest functionality: from level 1 to level 5. [3]
The occupational impact of those diagnosed with this neuromotor disorder is of great magnitude, not only for those who experience it, but also for their family and environment, because there are considerable difficulties in the independence of the person in the various areas of life. occupation. Focusing on pediatric patients from 0 to 18 years of age, the most affected areas correspond to: basic and instrumental activities of daily living, education, play and social participation. This is why children and adolescents require continuous treatment to promote and/or facilitate their occupational performance and, above all, their social participation and inclusion. [4]
When an infant is diagnosed with PCI, the family begins to search for support based on the diverse needs stated by the specialist doctor. An unbalanced and uncertain period begins, due to the absence of state protocols and routes to follow. for the treatment of children with PCI. The guidance that parents obtain is usually partial; initial referral only to physical therapy tends to be the most frequent. [5] Children with cerebral palsy have complex medical care needs, and often require care by a multidisciplinary team, since in addition to neurological problems, other disorders are associated that will be more frequent as the degree of cerebral palsy increases. of affectation, which will be key in estimating life expectancy. [6] The diagnosis of a child with CP alters, to a greater or lesser extent, family life.
In many cases, parents have a series of feelings that paralyze them and that arise as a defense mechanism, such as denial. Parents usually have a very limited vision of the situation, they feel stunned and will require a period of adaptation, since many changes are generated both individually and in the entire family; New responsibilities, obligations and commitments are assumed, which will change daily routines, relationships among themselves and with others. [7]
In another order of ideas, occupational therapy (OT) draws on the performance components (sensory-motor, cognitive and psychosocial) to help people achieve greater independence and autonomy, maintain functions and correct deficits through of AVDS (Activities of Daily Living). Psychomotricity is a very useful tool since it starts from the body and movement as a global expression of the individual. It adjusts to the evolutionary moment, offering security, pleasure and affection. [8]
OT is a socio-health modality that, from its theoretical and practical bases, focuses its intervention on enhancing the autonomy and independence of people in their daily lives, based on meaningful occupations. This profession uses the term occupation to refer to ADLs, and is based on retraining those necessary capacities so that daily activities can be carried out with the greatest possible autonomy. The treatment of Spastic infantile cerebral palsy from OT can be proposed from different approaches and intervention frameworks that will determine what the guidelines will be followed during the recovery process and will also serve to encompass the professional's practice. within the theoretical framework that bases it. [9]
The objective of this work is to assess the preparation of families of children diagnosed with spastic infantile cerebral palsy.
A pre-experimental study was carried out at the University of Medical Sciences of Sancti Spiritus on nine families with children diagnosed with spastic infantile cerebral palsy from zero days of birth to five years and eleven months belonging to the Dr. Juan Miguel Martínez Puentes Polyclinic in the northern area. from the province of Sancti Spiritus, Cuba.
The study sample was made up of nine families belonging to the health area of the center under study, belonging to several Family Medical Clinics. The independent variable was the activities related to occupational therapy for the preparation of families with children diagnosed with spastic infantile cerebral palsy.
The dependent variables were structured as follows:
Taking into account the accomplished bibliographic research, the meticulous examination of documents from the specialized literature and the regulations established from the initial diagnosis made, those who presented a proposal for activities related to the related topic, which were characterized by being designed from a conceptual reflective and socializing, which allowed promoting the conscious, responsible and systematic intervention of the family and their continuity in the home, with a level of satisfaction from a psychological point of view. Different methods were used, among which the following stand out: workshops, educational talks, family education schools and participatory techniques (psychodrama). A diagnosis was carried out where the state of knowledge of indicators was verified through a pre-test. The researchers kept in mind the reflections that come from the daily life of each family; family members assume an active position by expressing their opinions at home, asking questions, arguing their points of view, so that new knowledge and They remodel the existing ones around the related theme. Specific actions were guided to be carried out in pairs, subsequently they were analyzed in different exchanges. Each family presented their experience regarding what was oriented. To the extent possible, optimal conditions were created for them to sit in a horseshoe shape or in a circle, so as to facilitate close communication between everyone. The starting point was strict attention to the individual needs and potential of each of the families to achieve their maximum development within the scope of the proposed objectives.
The precision of the control, self-control and self-assessment actions of each of the families was taken into account. This allowed us to know the errors that may be being made during the sessions, as well as the aspects with the best results. The families that had the greatest difficulties in providing treatment required a climate of trust, respect and security, in which the forms of Communication generated relationships of collaboration and cooperation between everyone. The authors declared their commitment to confidentiality and protection of the information collected during the research through informed consent. Authorization and approval were also requested from the Research Ethics Committee and the Scientific Council of the University of Medical Sciences for the execution of the research.
We see the comprehensive evaluation of each sampled family in the indicators of the operational variable as a result of the application of the pre-test. In indicator one: Knowledge about the role of the family in the development of occupational therapy, it was found that, of nine families sampled, only one expressed mastery in this sense at the beginning and is evaluated at the high level (11.1%) and Seven families did not have any domain to essentially distinguish the characteristics that conceptualize occupational therapy as a treatment and were found at the low level (77.8%). In indicator two: Knowledge about the activities basically included in occupational therapy, it was found that in the sample only one family is always updated on the problem addressed and is evaluated at the high level (11.1%), it is also seen that Some of these are updated on the problem addressed, but with inaccuracies in distinguishing their main characteristics, being at the medium level (11.1%) (Table 1).
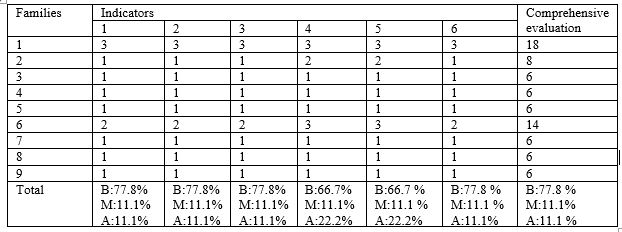
Table 1. Comprehensive evaluation of each sampled family in the indicators of the operational variable as a result of the application of the pre-test
Source: Data obtained from the diagnosis of the study sample In indicator three: Motivation to participate in the activities included in occupational therapy, it was possible to verify before the intervention that only one family is motivated to participate adequately in the activities, being evaluated at the high level (11.1%), a family is motivated to participate in activities, but with inaccuracies in delimiting active participation, being at the medium level (11.1%). In indicator four: Stimulation of communication in the family context, it was found that only two families always achieve the stimulation of communication by delimiting the corresponding actions, being at the high level (22.2%). In indicator five: Correct postural management in the family context, it was found that two families always manage to adequately carry out postural management by defining the actions to be carried out, which is why they are at the high level, (22.2%), one family Sometimes they achieve postural management, but with inaccuracies in defining the actions to be carried out in the process, which is why they are at the medium level (11.1%). In indicator six: Prevention of deformities in the family context, it was found that one family always prevents deformities, which is why it is at the high level (11.1%), the remaining seven families do not prevent deformities, being at the low level (77.8%).
The comprehensive evaluation of each family sampled in the indicators of the operational variable as a result of the application of the post-test, where in indicator one: Knowledge about the role of the family in the development of occupational therapy, after the intervention obtained favorable results related to this indicator, being (77.8%) at the high level. In indicator two: Knowledge about the activities basically included in occupational therapy, with the activities carried out it was possible to see the positive change in the families related to this indicator (77.8%) at the high level. In indicator three: Motivation to participate in the activities included in occupational therapy, seven families felt motivated to participate in the activities (77.8%), being at the high level (Table 2).

Table 2. Comprehensive evaluation of each sampled family in the indicators of the operational variable as a result of the application of the post-test
Source: Data obtained from the diagnosis of the study sample
In indicator four: Stimulation of communication in the family context, after the intervention, one (88.9%) of the families managed to learn a better way to stimulate communication. In indicator five: Correct postural management in the family context, after the intervention this indicator improved to (88.9%) at the high level. In indicator six: Prevention of deformities in the family context, a score (77.8 %) was obtained, so this indicator improved positively.
We see the distribution of frequencies of the evaluation of the indicators in the initial or pre-test stage and final verification or post-test of the pedagogical pre-experiment where in all the indicators their state of knowledge improved (Table 3).

Table 3. Frequency distribution of the evaluation of the indicators in the pre-test and post-test stage
Source: Data obtained from the diagnosis of the study sample this research
Over the years, occupational therapists have had to modify and devise techniques to meet the needs of clients and their families and thus be facilitators during the therapeutic process to promote active participation in the community and carry out their occupations. significant. In saying this, it is considered that the context in which one works influences what professionals do, generating knowledge and new practices for the profession. The occupational therapist is responsible for carrying out specific treatments, always using activity as a means, for the user's functional recovery. 10,11
With this study it was observed that, of all the indicators evaluated in the nine families with children with spastic infantile cerebral palsy in their diagnostic stage, only one family had knowledge about the role of the family in the development of occupational therapy. This result was transformed after the intervention that was carried out. In the indicator stimulation of communication in the family context, it was previously possible to verify that a low percentage achieved the stimulation of communication by delimiting corresponding actions, where after the intervention the majority of families managed to learn a better way to stimulate communication. In the indicator prevention of deformities in the family context, it was possible to verify before the intervention that he always prevented deformities, the remaining families did not, something that changed with the intervention since a favorable result was obtained for this indicator.
It is worth noting that these motor disorders are usually linked to comorbidities such as epilepsy, alterations in sensitivity, perception, cognition, deterioration in communication and behavior, and secondary musculoskeletal problems that largely contribute to a greater burden. on the health of children and families. For this reason, it is considered the most common cause of motor disability in pediatric age and the second cause of severe mental retardation. 1
In a study by Pintado,[12] at the University of Zaragoza The transformation of the family is highlighted when learning about the diagnosis of their child with PCI and the psychological impact it has on their actions, which is why many families overprotect their child and thus distance themselves from the role they must assume in caring for them. something that coincided with this study since only one family initially expressed dominance in this sense.
In a research carried out by Vidal, [13] at the University of La Coruña, it was evident that parents of children with PCI felt tired and demotivated with the lifestyle they led from the birth of the child until the date the research was carried out. , where in our research at the beginning we were able to obtain that only two families used stimulation techniques to communicate with their child with PCI and two families only knew postural management defining actions to be carried out.
Otero, [14]at the Del Norte Technical University, the results of an investigation showed that it is very difficult for parents to get rid of the image they had of their child since no family member is prepared for something that they must assume without having any knowledge and they must abandon and put aside their activities at the same time. which they were used to.
Regarding nursing care in parents and guardians of children with cerebral palsy by Lira, [15]at the Andean University of Cusco, it was found that parents with children diagnosed with PCI indicate that they do not fully know theoretical aspects about the knowledge and skills that should be applied by Nurses and it is mostly pointed out that Nursing professionals do not use techniques to increase the quality of life of their family member. In our study, it was possible to contact in the diagnostic stage that only one family knew the work of Occupational Therapy in the PCI.
Acapnia, [16]in a psychoeducation program for the management of parental and marital communication in families of children diagnosed with cerebral palsy, carried out at the Salesiana Polytechnic University, It could be seen that the parents were female with 94.12% and that only 5.88% were male, which proved that women are the most representative of their children with Cerebral Palsy.
Related to assertive parental communication, it was stated that the category that had the most relevance was the use of respect, attention and trust, in passive parental communication it was observed that there is no organization to carry out family activities and where it was observed that factors such as scolding were present in that type of communication. Many of those who participated pointed out that minors like to participate, but the parents' anger, reproach, disinterest and seriousness in intervening can be seen. Finally, reference is made to how in aggressive parental communication a large part of the interviewees maintained a negative attitude, where there were also participants who proceeded positively with motivation, conversation and other ways of proceeding.
The authors have no conflicts of interest in relation to the research presented.
The authors did not receive funding for the development of this research
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
