
case report | DOI: https://doi.org/10.31579/2690-4861/614
1Department of Cell and Molecular Biology, Faculty of Chemistry, University of Kashan, Kashan, Iran.
2Department of Medical Genetics, Kashan University of Medical Sciences and Health Services, Kashan, Iran.
*Corresponding Author: Zahra Rezvani, Department of Cell and Molecular Biology, Faculty of Chemistry, University of Kashan, Kashan, Iran.
Citation: Arezou Heydari, Zahra Rezvani, Mohamad Ali Dowlati, (2024), Prenatal Diagnosis of Congenital Diaphragmatic Hernia with Mosaicism Level 1 of Chromosomes 17q and 18q in Iran: a case report, International Journal of Clinical Case Reports and Reviews, 20(5); DOI:10.31579/2690-4861/614
Copyright: © 2024, Zahra Rezvani. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 22 November 2024 | Accepted: 13 December 2024 | Published: 20 December 2024
Keywords: congenital diaphragmatic hernia; prenatal diagnosis; mosaicism; amniocentesis; genetic testing
Congenital diaphragmatic hernia (CDH) is a common birth defect with high mortality and morbidity and is defined as the protrusion of abdominal contents into the chest cavity through an abnormal opening in the diaphragm of the fetus or infant. This abnormality is caused by multiple factors, including both genetic and environmental components, and can also be associated with several syndromes. Among the chromosomal abnormalities associated with CDH, trisomy 21, 18, and 13 are the most common. Also, complex chromosomal aberrations such as mosaicism have been reported. We present a case of prenatally diagnosed CDH with level 1 mosaicism of chromosomes 17q and 18q in a 34-year-old Iranian woman. The diagnosis was made at 16 weeks of gestation using ultrasound and confirmed by amniocentesis. In light of the presence of mosaicism of chromosomes in this instance, it is suggested that a potential genetic factor may play a role in the emergence of CDH, necessitating additional research. This case underscores the significance of genetic testing in the prenatal diagnosis of CDH and emphasizes the necessity for comprehensive counseling for affected families.
Congenital diaphragmatic hernia (CDH) is a rare congenital structural disease in which the diaphragm develops incompletely, leading to herniation of the abdominal organs in the chest of the fetus. Its characteristics include hyperplasia, blood pressure after birth due to vascular remodeling, and cardiac dysfunction [1,2]. CDH occurs in approximately 2.3 out of every 10,000 live births in Europe and 3.2 out of every 10,000 live births in the USA and may be detected before birth, at birth, or in some cases only in later infancy [3,4]. The mortality rate in these patients varies between 20% and 40% [5].
The etiology of CDH remains largely unclear, and it is generally believed to be influenced by a variety of factors [6]. These factors include genetic components [7], environmental exposure, and nutritional insufficiencies, which have been suggested as potential causes for the development of CDH [6].
The following case report presents a case of CDH with mosaicism level 1 of chromosomes 17q and 18q that was detected prenatally.
A healthy, 34-year-old Iranian female patient presented herself at a hospital during her 16th week of pregnancy, accompanied by an ultrasound scan that revealed a fetal diaphragmatic hernia. This couple was already parents to a healthy 8-year-old daughter and had no history of miscarriage or genetic family diseases. At the beginning of her pregnancy, the mother was hospitalized for seven days due to influenza with a fever. In the first trimester of pregnancy, the mother underwent screening, which yielded normal results according to the table below. It is worth noting that the risk of Down Syndrome and trisomy 18 in this patient is lower than the screening cut-off (Table 1).
| CLINICAL RESULTS | ||
| Assay | Results | Mom |
| PAPP-A † | 3.80 mlU/mL | 1.50 |
| Free β-hCG | 49.10 ng/mL | 1.26 |
| NT †† | 1.40mm | 1.20 |
| Risk Assessment (at term) | ||
| Down Syndrome | 1:4110 | |
| Age alone | 1:473 | |
| Equivalent Age Risk | <15> | |
| Trisomy 18/13 | 1:99000 | |
† PAPP-A, Pregnancy-associated plasma protein A
†† NT, Nuchal Translucency
Table 1. Clinical Results Screening at the end of the twelfth week. The results are normal. The risk of Down syndrome is LESS than the screening cut-off. The risk of Trisomy 18 is LESS than the screening cut-off.
A prenatal ultrasound examination was conducted during the 16th week of pregnancy to assess the fetal anomalies. The fetal biometric measurements indicated a biparietal diameter of 37mm, a head circumference of 110mm, a femur length of 22mm, amniotic fluid level of 84mm, fetal heart rate of 149 beats per minute, and an estimated fetal weight of 170g. Additionally, all fetal soft markers for trisomy were normal, and no gross anomalies were observed. However, a left-sided diaphragmatic hernia containing the stomach and no umbilical cord was detected, along with abdominal wall defects. As a result, the patient decided to undergo amniocentesis for genetic analysis.
Amniocentesis was carried out. In fetal karyotype analysis, 1.5% of cells were found to have 46 chromosomes, including an isochromosome 17q, 1.5% of cells had 46 chromosomes with an isochromosome 18q, and 97% of cells had 46 normal male chromosomes (with monosomy 17p and trisomy 17q in some cells, and monosomy 18p and trisomy 18q in other cells). This indicates a mosaicism level of 1 for isochromosomes 17q and 18q (Figure_1).
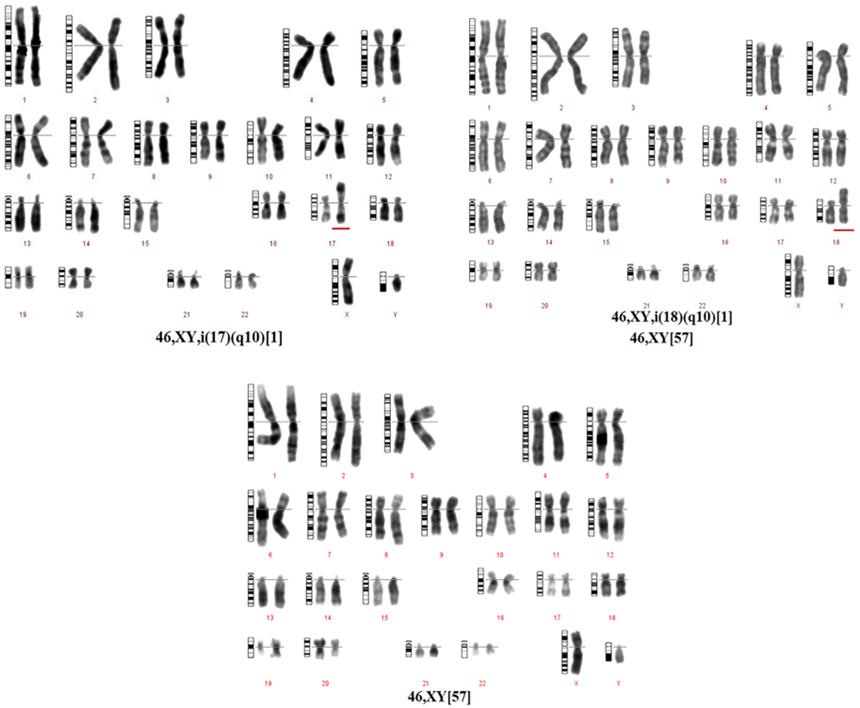
Figure_1. The initial image depicts cells exhibiting isochromosome 17q, while the subsequent image showcases cells displaying isochromosome 18q. The third photo portrays cells with standard chromosomes, which suggests a mosaicism level of 1 for isochromosomes 17q and 18q.
It is important to note that the percentages mentioned may differ in other tissues and could potentially lead to noticeable symptoms. This case may be unique in another pregnancy, but there is a possibility of a genetic condition. Therefore, it is recommended to examine the chromosomal changes and gene mutations in this instance.
The recommendation for the couple's karyotype was put forth, and both karyotypes were found to be typical. Nevertheless, the pregnancy was not terminated. At the 28th week ultrasound, the left-sided fetal diaphragmatic hernia was again observed, along with an amniotic fluid level of 162mm, which indicated polyhydramnios.
The cytomegalovirus IgG and toxoplasma IgG tests for the mother revealed values of 31 and 57, respectively. These values are considered high. The infant was born at 38 weeks' gestation and was unfortunately stillborn.
Discussion
As mentioned, CDH is a multifactorial condition for which the environmental and genetic contributions have not yet been fully elucidated [6, 7].
Advanced maternal age increases the risk of chromosomal anomalies, which are estimated to affect 10% of CDH cases. Additionally, young maternal age is associated with smoking, alcohol use, pregestational diabetes, maternal underweight, and delay in antenatal care. Additionally, young maternal age is associated with smoking, alcohol use, pregestational diabetes, maternal underweight, and delay in antenatal care [7, 8].
A prenatal diagnosis of CDH can be achieved as early as 12 weeks into the first trimester through ultrasound screening, with approximately 60% of cases being diagnosed in this manner. To provide a comprehensive diagnostic evaluation and accurate counseling, genetic testing, such as karyotyping, array comparative genomic hybridization, and targeted resequencing, should be conducted. Genetic testing is necessary for accurate counseling, future pregnancies, and eligibility for prenatal therapy. However, it is important to note that many newborns are born without a prenatal diagnosis which is typically detected within the first month following birth. However, a small percentage of CDH patients, roughly 10%, are diagnosed at a later stage in life [9-13]. Magnetic resonance imaging (MRI) may be utilized to assess fetal anomalies, especially when lung hypoplasia is a possibility [14].
Based on the location of the defect in the diaphragm, hernias can be classified into different types. Bochdalek hernias are the most prevalent type, accounting for 70% to 75% of all cases. These hernias arise from a defect in the postero-lateral part of the diaphragm and are most commonly found on the left side, with fewer occurrences on the right side. Morgagni hernias, which stem from a defect in the anteromedial part of the diaphragm, represent 20% to 25% of all cases. Central hernias comprise 2% to 5% of all hernias, and it is worth noting that 70% to 90% of all congenital diaphragmatic hernias (CDHs) occur on the left side. Bilateral defects are extremely rare and are associated with a poor prognosis [15, 16].
Many patients with CDH have no family history of the condition, leading to it being commonly interpreted as a sporadic occurrence. the majority of CDH cases are believed to be multifactorial and the exact cause of most cases remains unknown. However, there is growing evidence that genetic factors may play a role in the development of CDH [9].
CDH can occur either in isolation (50% of cases) or in combination with other congenital anomalies (non-isolated CDH or CDH +). This can occur as part of a genetic syndrome, a chromosome abnormality, or a nonsyndromic collection of major congenital malformations [9].
Anomalies can include various components of the body, such as the heart, urogenital system, limbs, nervous system, orofacial region, and gastrointestinal system [2].
Chromosomal abnormalities have been identified in approximately 33% of cases involving CDH. These abnormalities include trisomies, microdeletion syndromes, and unbalanced translocations. Several defined syndromes, such as trisomies 13, 18, and 21 [17], Pallister-Killian syndrome, monogenic disorders like Craniofrontal nasal syndrome, Donnai-Barrow syndrome, Simpson-Golabi-Behmel syndrome [18], Denys–Drash Syndrome, Marfan Syndrome [9], Coffin-Siris syndrome and Cornelia de Lange syndrome, or associations like Fryns syndrome, comprise CDH as a component of malformations [17].
Low-level mosaicism of the co-occurrence of isochromosome 17q and 18q has not been reported in the literature to date. However, there are a few reports that suggest the implication of chromosome 18 dosage imbalance in the formation of diaphragmatic hernia in fetuses [19, 20].
It was noted that the precise cause of CDH remains unidentified. Given the life-threatening nature of this condition, efforts are being made to improve the prognosis rate before birth. To support these efforts, this article presents a case of CDH accompanied with mosaicism level 1 of isochromosomes 17q and 18q.
Ethical Approval and Consent to participate
Not applicable
Not applicable
Not applicable
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Not applicable
Arezou Heydari: Contributed to the study's conception, data collection, and manuscript drafting. Acted as the lead author and coordinated all aspects of the research and writing process.
Zahra Rezvani (Corresponding Author): Guided the study's scientific direction, reviewed the manuscript thoroughly, and also performed critical revisions of the manuscript.
Mohamad Ali Dowlati: Provided clinical and genetic data of the patient referring to the laboratory, reviewed and refined the manuscript, and offered expert insight.
Not applicable
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
