
Research Article | DOI: https://doi.org/10.31579/2641-0419/373
1Thoracic and cardio-vascular surgery department (Andre Festoc center, bamako)
2Cardiology department of the "Luxembourg" mother-child hospital in Bamako (Mali)
3Faculty of Medicine and Odontostomatology, University of Technical Sciences and Technologies of Bamako; Mali
4Thoracic surgery department « hopital du mali »
5Non-governmental organization chain of hope (France)
*Corresponding Author: Baba Ibrahima Diarra,Thoracic and cardio-vascular surgery department
Citation: Diarra B I, Doumbia M, Keita A, Bouaré L, Touré M, et al, (2024), Preliminary Results of Conservative Mitral Valve Surgery at The Andre Festoc Center of The Mother -Child "Luxembourg" In Mali, J Clinical Cardiology and Cardiovascular Interventions, 7(6); DOI: 10.31579/2641-0419/373
Copyright: © 2024, Baba Ibrahima Diarra. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 22 April 2024 | Accepted: 28 May 2024 | Published: 20 June 2024
Keywords: conservative; mitral surgery; result
In developed countries rheumatic disease has become a virtual disease. On the other hand it remains the most frequent cause of cardiovascular morbidity and mortality in people under 40 years of age in our developing countries.
The aim of this work is to present the preliminary results of mitral valve repair in a developing country. This is a 52-month mono-centric retro-prospective descriptive study from September 10, 2018 to December 31, 2022.The study was carried out at the André Festoc center of the mother-child university hospital center ‘ Le Luxembourg’ in Bamako. During the period of our study 490 patients underwent heart surgery, 174 patients or 35.51% had mitral surgery and mitral plasty on rheumatic valvulopathy was performed in 35 patients or 20.11% of mitral surgeries and 7.14% of all cardiac operations.
We collected 33 cases, 2 patients were lost to follow-up. 72% of patients were female, with a sex ratio of 0.4. Mean age was 12.9 ±3.9 years, with extremes of 5 and 25 years.
Valvular retraction was the most common lesion, accounting for 81.8% of cases. All patients underwent surgery under CEC ranging from 81 to 245 min, with an average of 131.40 ± 40 min. The mean aortic clamping time was 87.72 ± 31.60 min, with extremes of 26 and 169 min. Attendance time ranged from 7 to 105 min, with a mean of 31.33 ± 20.94 min.
Mitral plasty is a preferred alternative to valve replacement in children. The complexity of the lesions involved makes this procedure difficult, and good results can only be achieved through rigorous patient selection and precise lesion analysis.
Rheumatic fever (RF) or BOUILLAUD's disease is an inflammatory disease complicating infection with group A streptococcus [1].
Of all the conditions secondary to rheumatic fever, rheumatic valvulopathy is the most dreaded, and currently represents one of the main causes of cardiovascular disease in schoolchildren and young adults in most developing countries [2].
Of all the conditions secondary to AAR, rheumatic valvulopathy is the most dreaded and currently represents one of the main cardiovascular disorders in school-age children and young adults in most developing countries [2].
The frequency of these rheumatic valvulopathies is estimated at 21.5 per 1000 in Cambodia; 30.4 per 1000 in Mozambique; 7.5 per 1000 in Senegal [24].
The development of Doppler echocardiography has led to better assessment of cardiac valve damage, improved follow-up and thus a clear improvement in the management of rheumatic valve disease. [25]
Mitral plasty, also known as mitral reconstructive or reparative surgery, is a preferred alternative to mitral valve replacement. The advantages of this type of reconstructive surgery are low postoperative mortality, better preservation of left ventricular function and conservation of the native valve, thus avoiding the problem of anticoagulant treatment [3]. This surgery is well suited to developing countries, where the cost of cardiac prostheses, with or without lifelong anticoagulation, is exorbitant.
The complexity of rheumatic mitral valve lesions and their potential for evolution mean that repairs are often more difficult than in degenerative or ischemic pathology. Short- or long-term results may be altered by possible lesion evolutivity in a fairly young population. [23]
To date, no such study has been carried out in our country.
This was a 52-month mono-centric retro-prospective descriptive study from September 10, 2018 to December 31, 2022.
The study was carried out at the André Festoc center of the mother-child university hospital center le Luxembourg in Bamako.
- Study population:
All patients with rheumatic mitral valve disease who had been to the ANDRE FESTOC center of the mother and child hospital « le Luxembourg ».
- Inclusion criteria:
Patients who underwent mitral plasty for rheumatic valvulopathy at of the mother and child hospital « le Luxembourg » in Bamako were included in this study.
- Exclusion criteria:
The following were not included in this study:
- Patients having undergone mitral valve replacement in another country.
- Patients who had undergone mitral valve replacement
- Patients with incomplete records
Dyspnea on exertion was the main symptom observed in all patients, followed by palpitations (45.5%) (Figure 1).
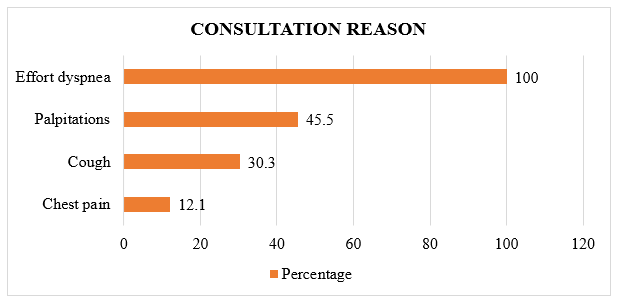
Figure 1: Distribution of patients by reason for consultation
Physical signs were dominated by the systolic murmur of mitral insufficiency and hepatomegaly, with 87.9% and 24.2% respectively (figure 2).
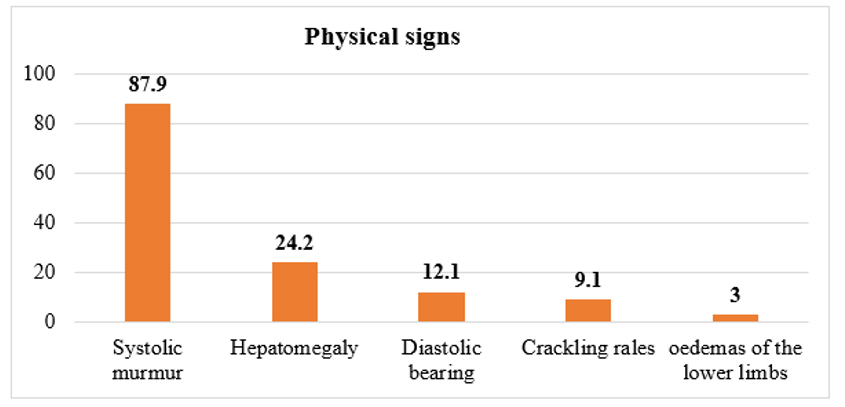
Figure 2: Physical signs
Cardiomegaly was found in 90.9% of patients. The mean cardiothoracic index was 0.63 ±0.09, with extremes of 0.80 and 0.44 (figure 3).
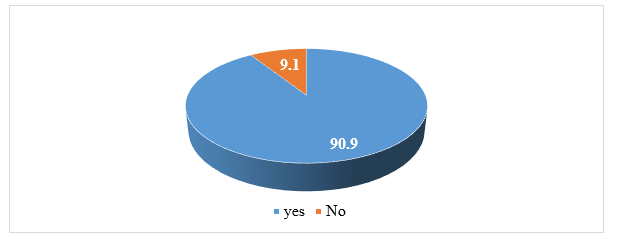
Figure 3: Cardiomegaly in percentage
Sinus rhythm was present in 96.9% of patients, and only one patient was in atrial fibrillation. (Figure 4).
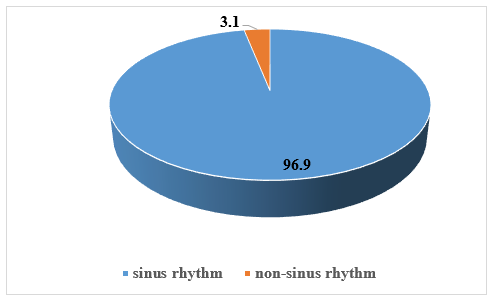
Figure 4: electrocardiography
Mitral insufficiency was the predominant valvulopathy, with 28 cases (84.8%) (Figure 5).
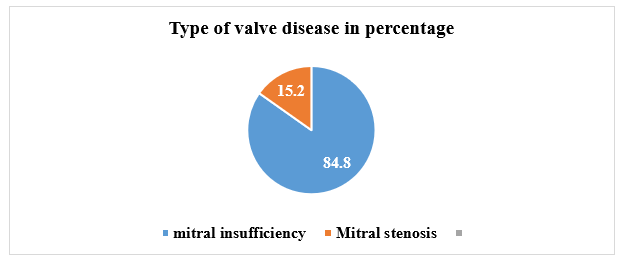
Figure 5: type of valve disease in percentage
Tricuspid insufficiency was the valvulopathy most associated with mitral insufficiency, accounting for 36.4% of cases (figure 6).
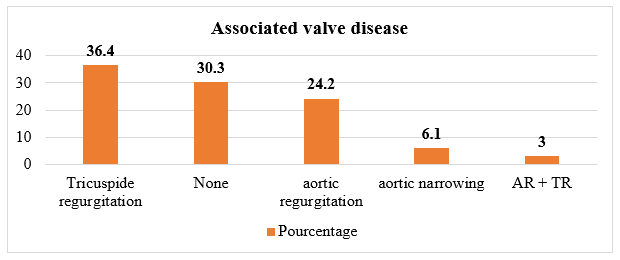
Figure 6: Distribution of patients according to associated valvulopathy
Valvular retraction was the most common lesion (81.8%) (Figure 7).
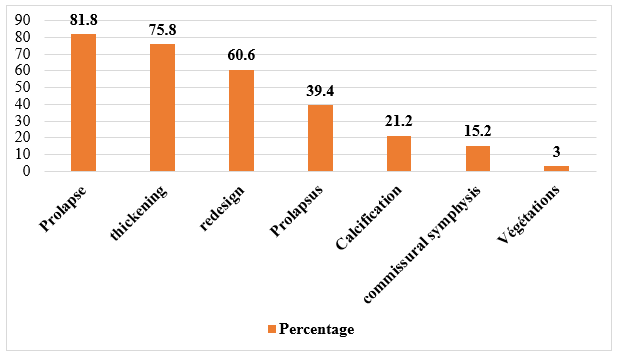
Figure 7: Distribution by type of mitral valve lesion
The subvalvular apparatus was intact in the majority of patients (54.5%), while 36.4% showed remodeling (figure 8).
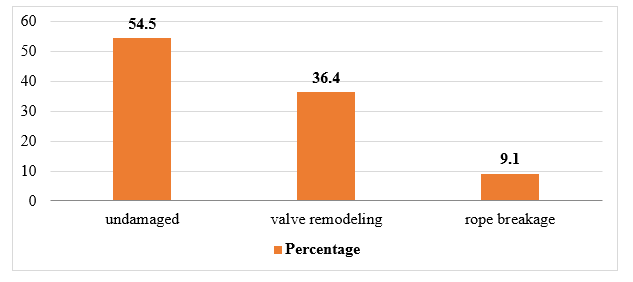
Figure 8: Distribution by type of subvalvular apparatus lesions
Grade 4/4 mitral leakage accounted for 82.1% of cases, while 17.9% were grade 3/4. All patients had OG dilatation with a mean surface area of 34.77 ± 13.2 cm² with extremes of 19 and 75 cm².The LV was dilated in 66.7% of patients. DV dilatation was found in 6.1% of patients.LV ejection fraction was preserved in 90.9% of patients, with a mean of 64.18 ± 8.42% and extremes of 46 and 78%.The majority of patients (51.5%) had no PAH, and 36.4% had significant PAH.A median sternotomy was the preferred approach in 97% of cases. Mini thoracotomy was performed in one patient (3%). All patients underwent bypass surgery ranging from 81 to 245 min, with an average of 131.40 ± 40 min. Mean aortic clamping time was 87.72 ± 31.60 min, with extremes of 26 and 169 min. Assistance time ranged from 7 to 105 min, with a mean of 31.33 ± 20.94 min. Annuloplasty plus cord release were the most common procedures performed in 21.2% of patients. Tricuspid plasty was the procedure most associated with mitral plasty, in 7 cases (21.2%).
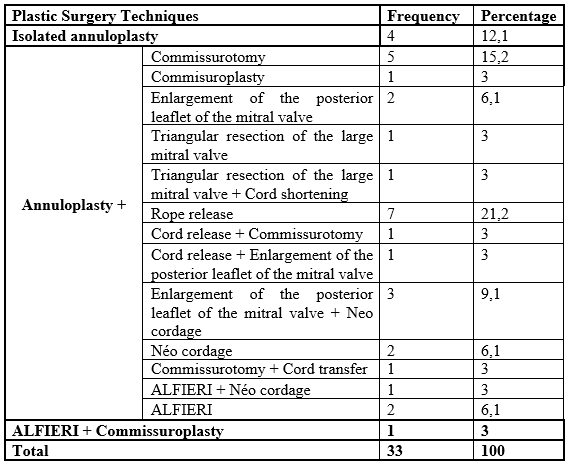
4- Table I: Surgical procedures :
1- Intensive care unit stay:
ICU stay ranged from 0 to 11 days, with an average of 4.45 ± 2.06 days.
Early postoperative morbidity was 21%.
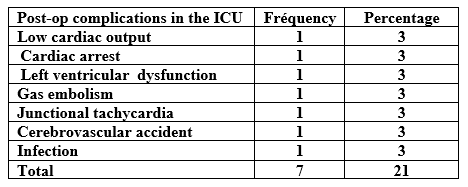
2-Table II: Early postoperative morbidity in the ICU:
Peri-operative mortality was 6%, or 2 patients.
3- Early transthoracic echocardiography on discharge from intensive care :
At ICU discharge, echocardiography was performed on 31 patients (94%).

3-Table III: Residual leak on mitral plasty :
Residual MI was present in all patients.
Grade 1 MI was in the majority, with 23 cases (74.2%).
The mean mitral valve gradient was ≤ 5 mmHg in 48.5% of patients, with a mean of 5.58 ± 2.32 mmHg and extremes of 2 and 13 mmHg.
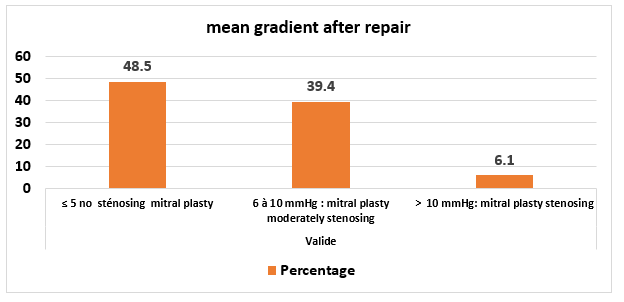
Figure 9: Distribution of patients by mean gradient for post-op mitral plasty
The LV was non-dilated in 51.6% with a mean DTD of 49.61 ± 8.85 mm and a mean DTS of 36.14 ± 8.49 mm and extremes of 31-72 mm for diastole, 24-60 mm for systole.
LVEF was reduced in 12.9%, intermediate in 45.2% and preserved in 41.9%, with a mean of 47.94% and extremes of 30 and 63%.
The mean postoperative PAPS was 37.45 ± 14.18 mmHg, ranging from 21 to 72 mmHg.
PAH was absent in 64.5% of patients. At 3 months post-op, NYHA stage 2 was the most common at 51.6%, followed by stage 1 at 45.2% and stage 3 at 3.2%. Morbidity at 3 months was marked by a cumulative endocarditis rate of 3% (1 patient) and INR instability of 3% (1 patient) (mitral plasty associated with AVR on VKA).There were no deaths at 3 months after mitral plasty. All patients had a residual leak.
Grade 1 leakage predominated, with 19 cases (61.3%).

Table IV: Residual leakage on mitral plasty
The mean mitral valve gradient was between 6 and 10 mmHg was predominant in 51.6% of cases. The mean was 6.96 ± 2.79 with extremesof 3 and 13 mmHg. The mean mitral valve gradient between 6 and 10 mm Hgwas predominant, accounting for 51.6% of cases. The mean was 6.96 ± 2.79, with extremes of extremes of 3 and 13 mmHg.
Morbi-mortality at M6:
There was no morbidity or mortality at 6 months. Seventeen patients (56.7%) had a grade 1 residual leak. One patient (3.3%) had a major grade 3 leak. Seventeen patients (56.7%) had Grade 1 residual leakage. One patient (3.3%) had a significant grade 3 leak.

Table V: Residual leak on mitral plasty:
The mean gradient on mitral plasty was predominantly between 6 and 10 mmHg, with a mean of 7.06 ± 2.57 mmHg and extremes of 3 and 12 mmHg.
At M6, the LV was predominantly undilated in 76.7% of cases, with a mean diameter of 49.11 ± 8.47 mm in diastole and 33.96 ± 7.61 in systole, and extremes of 38 and 82 mm for DTD 25 and 64 mm for DTS.
The mean gradient on mitral plasty was predominantly between 6 and 10 mmHg, with a mean of 7.06 ± 2.57 mmHg and extremes of 3 and 12 mmHg.
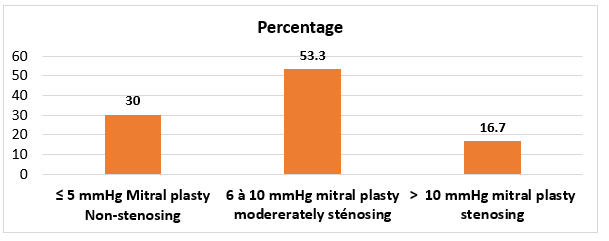
Figure 10: Distribution according to mean gradient mitral plasty at M6
1-Epidemiological:
Rheumatic heart disease is the most common valvular pathology in Third World countries, with a high prevalence in young school-age subjects, and constitutes a public health problem in these countries. [4-5].
Mitral valve replacement is generally preferred for rheumatic mitral disease. However, the limited lifespan of bioprostheses and the thromboembolic risk associated with mechanical valves, as well as the complications and cost of anticoagulant treatment, argue in favor of mitral plasty whenever possible [5].
Conservative mitral surgery enables the patient to retain his own valve, preserve the subvalvular tensor apparatus and the geometry of the left ventricle, and consequently conservation of left ventricular function and improved survival as well as remote functional status [6].
In our series, the mean age was 12.9 ±3.9 years, with extremes of 5 and 25 years. This result is similar to that of CISS AG in Senegal [7], who reported a mean age of 12 ±5 years, and close to those of SOUAGA K. A. in Abidjan [8] and SKOULARIGIS. J [9] who found 19 ± 9 and 18 ± 9 years respectively.
These results confirm that rheumatic valvulopathy is more common in young, active subjects.
In our study, as in the literature, the female sex is more concerned. In our study, the sex ratio was 0.4. In CISS [7] study it was 0.6 and in DIOP [14] study in Senegal the ratio was 0.62.
Recurrent sore throat was the most frequent antecedent with 51.5%.
This result was similar to those found by Diop [14] in Senegal, who reported 51% respectively.
2- Clinical:
Exertional dyspnoea was the main symptom in all our patients, with a predominance of NYHA stage III (66.7%), followed by stage II (24.2%) and stage IV (9.1%).
These results are similar to those of KUMAR in India [11] and DIOP [14] in Senegal.
This would indicate that they have reached an advanced stage of valvulopathy.
2- Paraclinical :
The electrocardiogram plays a key role in the evaluation of patients with valvular heart disease, where rhythm or conduction disorders are sometimes noted.
Atrial fibrillation is the most frequently observed rhythm disturbance in mitral valve disease.
The onset of AF in mitral valve disease marks a turning point in the progression of the disease, and exposes the patient to the risk of thromboembolic events and heart failure. Its onset also poses a major prognostic problem [11].
In our study, AF occurred in 3% of cases, a low rate compared with 62.9% in the series by KUMAR [11] and 21% in that of Diop [14].
However, this rate is close to that of CISS AG. [7], who had 0
Mitral plasty is a preferred alternative to valve replacement in children. The complexity of the lesions involved makes this procedure difficult, and good results can only be achieved through rigorous patient selection and precise lesion analysis. This study reveals the unique aspects of rheumatic valve repair. The short- and medium-term results of mitral plasty in rheumatic valve disease are encouraging, and call for further progress.
Conservative surgery is therefore a non-negligible option in our context, especially for women of childbearing age and children, given the risks associated with anticoagulant treatment in the case of mechanical valve replacement.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
