
Research Article | DOI: https://doi.org/10.31579/2578-8965/182
1 Reproductive Genetics Innovations, Northbrook, Illinois.
*Corresponding Author: Anver Kuliev, Reproductive Genetics Innovations, Northbrook, Illinois.
Citation: Svetlana Rechitsky, Tatiana Pakhalchuk, Maria Prokopovich, Agnes Machaj, Anver Kuliev (2023), Preimplantation Genetic Testing (PGT) for Non-Lethal Correctable Conditions Through Population Carrier Screening, J. Obstetrics Gynecology and Reproductive Sciences, 7(6) DOI:10.31579/2578-8965/182
Copyright: © 2023, Anver Kuliev. This is an open-access article distributed under the terms of The Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 August 2023 | Accepted: 29 August 2023 | Published: 07 September 2023
Keywords: preimplantation genetic testing for monogenic disorders (pgt-m); phenylketonuria (pku); hereditary hearing loss (hhl); prospective application of pgt-m, expanded carrier screening (ecs), non-lethal correctable conditions
An increasing number of patients without family history of genetic disease are referred for preimplantation genetic testing of monogenic disorders (PGT-M) after ascertainment through population (expanded) carrier screening (ECS), increasing the proportion of non-lethal correctable genetic conditions in PGT-M indication profile. The aim of this paper is to analyze the current dynamics of these changes in our PGT-M series, which is the world’s largest PGT-M experience. This was analyzed using our PGT-M for two prevalent examples of non-lethal correctable genetic conditions, phenylketonuria (PKU) and hereditary hearing loss (HHL) during the period of 2005-2022. During this period, 91 PGT-M cycles were performed for PKU, involving testing for 108 mutant alleles in PAH gene, and 262 PGT-M cycles for HHL, involving testing for up to 300 mutations in 13 different genes causing hearing loss. PGT-M for these non-lethal correctable conditions resulted in the birth of 54 babies free of PKU and 134 children free of HHL. Dynamics of PGT-M referrals during this period of 17 years demonstrated the shift from retrospective to prospective application of PGT-M for both conditions, with 87% of prospective PGT-M performed for PKU, and 82% for HHL, performed for couples who had no affected relatives with PKU or HHL. These at-risk couples were ascertained through ECS in the last decade, making it possible to provide the option of prospective PGT-M for these non-lethal correctable conditions.
Although phenylketonuria (PKU) and hereditary hearing loss (HHL) (https://hereditaryhearingloss.org/) are non-lethal conditions, they still require lifelong care, representing a real financial burden. Prenatal diagnosis of these conditions is also possible but leads to a difficult decision of a possible termination of affected pregnancy, which is the problem for any non-lethal condition. Preimplantation genetic testing (PGT), based on pre-selection and transfer of unaffected embryos avoids the risk for pregnancy termination, and most importantly, allows having children free of these conditions.
Since the introduction of PGT for monogenic disorders (PGT-M) [1,2], it has been applied for more than 600 different conditions, resulting in birth of thousands of children free of genetic disease [3]. Initially applied for avoiding a recurrence risk of having severe genetic conditions, PGT-M has
then been applied also for diseases with genetic predisposition, such as breast cancer and coronary disease [4-7]. It has been usually applied retrospectively for those at-risk couples who have already had an affected offspring with monogenic disorder, until introduction of different screening programs, including expanded (population) carrier screening (ECS), which made it possible to apply PGT-M for patients without an affected family member, with a chance of avoiding any possibility of having an affected child in the family. Accordingly, an increasing number of patients without family history of genetic disease are referred for PGT-M after ascertainment through ECS, also significantly increasing the proportion of non-lethal correctable genetic conditions in the indication profile. The aim of this paper is to analyze the current dynamics of these changes, based on our PGT-M series, which is the world’s largest PGT-M experience. As will be presented, using PGT-M for PKU and HHL, the examples of non-lethal correctable conditions, there is an ongoing shift of PGT-M from retrospective to prospective application, as a practical tool for primary prevention of genetic disorders.
Dynamics of referrals for PGT-M of PKU and HL were analyzed during the period of 2005-2022. These included 91 PGT-M cycles for PKU, performed for 53 at risk carriers of 108 mutant alleles in PAH gene, including 98 missence and 12 spicing mutations, and 1 deletion. For ten of these carries, a combined PGT-M was performed for additional conditions, including cystic fibrosis, fragile-X mental retardation, BRCA-1, myotonic dystrophy, adrenal hypoplasia, Wilson’s disease, propionic acidemia and translocation.
PGT-M for HHL was done in 262 PGT-M cycles for 178 patients at risk for producing progeny with syndromic and non-syndromic HHL, caused by up to 300 mutations in 13 different genes (Table 1).
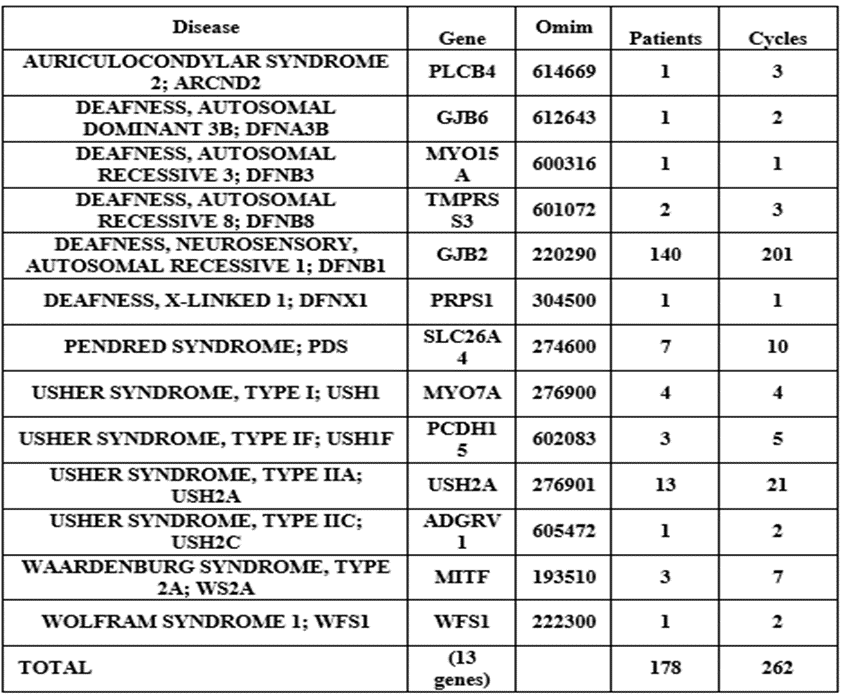
Table 1: List of Syndromic and Non-syndromic HHL for which PGT-Mwas performed during 2005-2022
Initially, most of these patients tested for PKU and HHL were referred for avoiding a recurrence of these conditions after birth of an affected child in the family, but the number of such patients has been decreasing in the last decade, with a corresponding increase of couples with no family history of these conditions, who referred for PGT-M to avoid even the first occurrence of the disease.
PGT-M methods applied during this period have changed from traditional mutation testing with linkage analysis using informative short tandem repeats (STRs), to more sophisticated approaches allowing a combined testing for single gene and chromosomal disorders [8]. In brief, PGT-M was performed using a standard IVF protocol, coupled with embryo biopsy, described in detail elsewhere [9]. Details of PGT guidelines were reported previously [10, 11]. The present standards of the procedure involve a whole genome amplification (WGA) of embryo samples obtained by blastocyst biopsy, followed by multiplex nested PCR analysis of the mutations in question, together with closely linked genetic markers in a multiplex heminested system [8,9]. For each family, heterozygous alleles and haplotypes not shared by parents were selected. This allowed detecting and avoiding misdiagnosis due to preferential amplification and allele dropout (ADO), and a possible aneuploidy or uniparental disomy of chromosomes in which the tested mutations are located, which may affect diagnostic accuracy of PGT-M. In PGT cycles, involving an advanced reproductive age of maternal partner, aneuploidy testing was also performed by next generation technologies (NGS) (Illumina Inc) for 24-chromosome aneuploidy analysis [8].
Results of 91 PGT-M cycles for PKU are presented in Table 2,
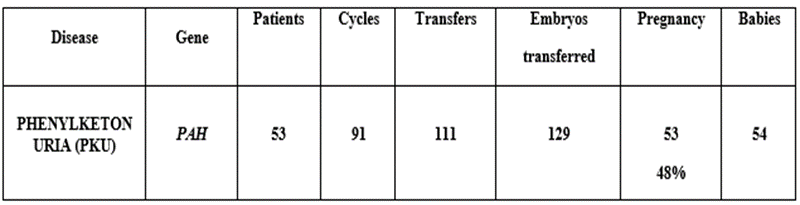
Table 2: PGT-M for Phenylketonuria (PKU)
showing the detection of 129 of PKU free embryos for transfer in 111 cycles, yielding 53 (48%) clinical pregnancies and birth of 54 unaffected babies. PGT-M referrals during the period of 2005-2015 were mainly (75%) after the birth of affected child, while after 2016 only a few (13%) PGT-M referral were due to an affected progeny in the family, while the majority (87%) were performed prospectively for couples who had no affected relative but were ascertained through ECS.
Similar results were observed in the dynamics of 262 PGT-M cycles performed for HHL, which resulted in transfer of 282 HHL free embryos in 258 cycles, yielding 164 (63.5%) clinical pregnancies and birth of 134 children free of HHL (Table 3).
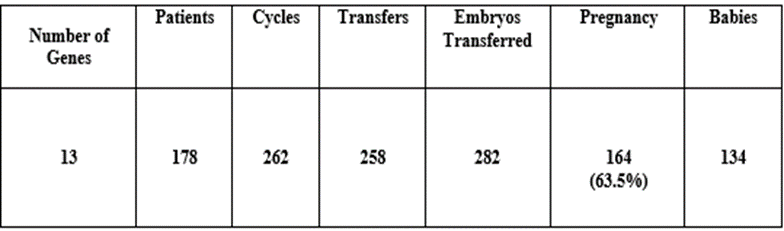
Table 3: PGT-M for Hereditary Hearing Loss (HHL)
PGT-M referrals during the period of 17 years showed the shift from retrospective to prospective application of PGT-M, with 82% -provided for couples with no affected relative, who were ascertained through ECS in the last decade (Table 4).

Table 4: Increase of PGT-M cases for Hereditary Hearing Loss (HHL) with no affected relative in the family, ascertained through expanded carrier screening (ECS)
The data show an increase of referral for PGT-M of PKU and HHL, which originally have not even been an indication for PGT-M. Such an increase may be related to the introduction of ECS, which allows couples at risk avoiding even the first occurrence of disease. Retrospective application of PGT-M was mainly prior-to 2016, performed to prevent a recurrence of PKU or HHL after couples have had an affected offspring or had a relative with these conditions. However, increasing number of patients after 2015 presented with no relative affected with PKU or HHL. Overall, 87% PGT-M cycles for PKU and 82% for HHL were performed prospectively for couples with no affected relative.
With a low treatment efficiency for therapeutic interventions and a high (25% - 50%) risks of recurrence in each pregnancy, PGT-M may be the main tool for the purpose of primary prevention of genetic disease. However, at-risk couples usually do not know about their at-risk status until they have an affected child, so reduction of affected birth prevalence cannot be done in the absence of screening programs, which have been offered for many years exclusively for special ethnic groups or selected genetic conditions. But in contrast to such screening programs applied to special groups of high incidences, ECS is offered in pan-ethnic fashion, extending surveillance to couples of all ethnicities and involving increasing number of genetic conditions [12,13], that appeared having a growing impact on PGT-M application. Targeted gene panels further increase the number of genetic disorders amenable to ECS, leading to PGT-M prospectively, representing a real form of primary prevention, as it allows avoiding affected pregnancies, and establishing unaffected pregnancies from the onset. Several hundred additional genes are becoming considered plausible candidates for inclusion into ECS, with expanded panels now consisting of hundreds of genes, resulting in the increase of detection rate [14]. Thus, presented dynamics of PGT-M during the period of 17 years demonstrated the shift from retrospective to prospective application of PGT -M for PKU and HHL. Overall, 87% and 82% PGT cycles for PKU and HHL, respectively, were performed prospectively for couples with no affected relative. An increase in referrals for PGT-M through ECS was observed also for other genes, with the number of prospective PGT-M cases for the last decade more than doubling through referral from ECS [15]. This may lead to the application PGT-M beyond family level, allowing to offer PGT-M prospectively before the birth of an affected child, as a tool for primary prevention of genetic disorders.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
