
Research Article | DOI: https://doi.org/10.31579/2690-8808/243
A.T. Still University School of Osteopathic Medicine in Arizona, Mesa, AZ, USA.
*Corresponding Author: Leonard B. Goldstein, A.T. Still University School of Osteopathic Medicine in Arizona, Mesa, AZ, USA.
Citation: Joshua Elmore, James Keane, Leonard B. Goldstein, (2025), Pregnancy and Lactation: A Lifespan Perspective on Maternal Cardiovascular Health and Risk, J, Clinical Case Reports and Studies, 6(1); DOI: 10.31579/2690-8808/243
Copyright: ©, 2025, Leonard B. Goldstein. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 08 January 2025 | Accepted: 15 January 2025 | Published: 24 January 2025
Keywords: cardiovascular disease; cardiovascular stress test; cardiovascular risk
Cardiovascular disease (CVD) remains the leading cause of mortality worldwide, responsible for 18.6 million deaths annually due to heart attacks and strokes. The economic impact is staggering, with the United States alone incurring $363 billion annually in direct and indirect costs. Primary risk factors such as an unhealthy diet, physical inactivity, smoking, and excessive alcohol consumption are further compounded by the rising prevalence of obesity and diabetes in urbanized areas, creating a significant global public health burden [3]
Cardiovascular disease (CVD) remains the leading cause of mortality worldwide, responsible for 18.6 million deaths annually due to heart attacks and strokes [1]. The economic impact is staggering, with the United States alone incurring $363 billion annually in direct and indirect costs [2]. Primary risk factors such as an unhealthy diet, physical inactivity, smoking, and excessive alcohol consumption are further compounded by the rising prevalence of obesity and diabetes in urbanized areas, creating a significant global public health burden [3]
Sex- and gender-specific differences in CVD play a pivotal role in its manifestation, management, and outcomes. Women often present with atypical symptoms, such as fatigue, nausea, and back pain, which delay diagnosis and treatment [4]. Premenopausal women benefit from estrogen’s protective cardiovascular effects, such as improved lipid profiles and enhanced vascular health, but these benefits diminish after menopause, increasing cardiovascular risk [5].
Pregnancy and lactation represent unique phases of the female lifespan, acting as critical "stress tests" that can unmask latent cardiovascular conditions [6]. These physiological transitions provide a window into maternal cardiovascular health, with pregnancy complications such as preeclampsia and gestational diabetes revealing potential future risks [7]. Similarly, lactation confers long-term cardiovascular benefits, offering unique opportunities for intervention and prevention. This paper aims to synthesize existing evidence and analyze cohort data to understand how pregnancy and lactation impact maternal cardiovascular health.
A systematic literature review was conducted using PubMed and Scopus to identify studies published between 2000 and 2023 on the relationship between pregnancy, lactation, and maternal cardiovascular health. Search terms included "adverse pregnancy outcomes," "lactation," and "biomarkers," with inclusion criteria focusing on peer-reviewed articles reporting cardiovascular outcomes related to pregnancy complications or lactation. Exclusion criteria eliminated studies without maternal outcomes or lacking robust methodologies. Following PRISMA guidelines, 120 studies were selected for synthesis from an initial pool of 3,500 articles.
A retrospective cohort analysis was performed using anonymized electronic health records (EHRs) from women aged 18–50 with documented pregnancies between 2010 and 2020. Inclusion criteria required records with at least five years of postpartum follow-up, while exclusions included incomplete records and pre-existing cardiovascular conditions. Key variables included demographic data, pregnancy outcomes, lactation duration, and cardiovascular events. Statistical methods included logistic regression for categorical outcomes and Kaplan-Meier survival analysis for time-to-event data, with significance set at p < 0.05. Data were stored securely following HIPAA guidelines, anonymized to protect participant confidentiality, and curated to ensure accuracy.
Pregnancy as a Cardiovascular Stress Test
Pregnancy induces profound hemodynamic changes, including increased blood volume, cardiac output, and hormonal fluctuations. These changes, while necessary for fetal development, stress the cardiovascular system, unmasking latent conditions such as heart failure or arrhythmias [8]. Labor and delivery further amplify these stressors, with postpartum hemodynamic shifts linked to conditions like peripartum cardiomyopathy (August et al., 2022).
Adverse Pregnancy Outcomes Linked to Future Cardiovascular Risk
Complications such as preeclampsia and gestational diabetes significantly elevate long-term cardiovascular risks. A meta-analysis found that women with preeclampsia face a four-fold higher risk of chronic hypertension and a two-fold increased risk of coronary heart disease [9,10]. Gestational diabetes is strongly predictive of type 2 diabetes, which predisposes women to atherosclerotic CVD (18, Bellamy et al., 2009).
Preeclampsia and Cardiovascular Risk
The probability of developing chronic hypertension, ischemic heart disease, or stroke later in life is strongly correlated with preeclampsia. A systematic review and meta-analysis demonstrated that women with a history of preeclampsia face a four-fold increased risk of developing chronic hypertension and a two-fold higher risk of coronary heart disease and stroke paralleled to women with normotensive pregnancies [9]. Similarly, data from a UK-based cohort study of 1.3 million women revealed that preeclampsia considerably increases the risk of chronic hypertension (hazard ratio [HR] 4.47), cardiac atherosclerotic events (HR 1.67), and stroke (HR 1.9), with these risks evident within a year of the index pregnancy [11]. Additionally, other than the immediate risks, preeclampsia also has long-term implications for cardiovascular health which can be compounded by structural and functional cardiac changes observed postpartum. It has been established that women with preeclampsia often exhibit left ventricular hypertrophy and reduced diastolic function, which can precede the development of chronic hypertension and other cardiovascular complications [12]. These findings highlight the need for lifelong monitoring and enhanced preventive strategies to address the amplified cardiovascular risk in women with a history of preeclampsia.

Source: Benschop et al. "Early Onset of Coronary Artery Calcification in Women With Previous Preeclampsia." Circulation: Cardiovascular Imaging, 2020;13:e010340. DOI: 10.1161/CIRCIMAGING.120.010340.
Chart Summary: This study highlights that women with a history of preeclampsia are at an increased risk of early onset coronary artery calcification (CAC), with notable differences observed in younger age groups.
Several studies have revealed a robust connection between lactation duration and reduced maternal hypertension risk. A meta-analysis of over 55,000 women found that exclusive breastfeeding for six months reduced hypertension risk by 29%, with additional reductions observed with longer lactation durations (Stuebe et al., 2011). Similarly, women who breastfed for 24 months or more were 88% less likely to develop hypertension compared to non-lactating women [15]. The protective effects of lactation on blood pressure are evident even decades after breastfeeding, highlighting the enduring cardiovascular benefits. Encouraging breastfeeding as a lifestyle intervention can help mitigate hypertension risk across the maternal lifespan.
Lactation is linked to a lower risk of stroke in women, with data showing significant reductions in ischemic stroke, intracerebral hemorrhage, and subarachnoid hemorrhage among postmenopausal women who breastfed (Ren et al., 2022). These protective effects appear to strengthen with longer breastfeeding durations, suggesting a dose-response relationship. Additionally, the metabolic and vascular benefits of lactation, such as reduced hypertension and diabetes risks, indirectly contribute to a lower stroke risk later in life (Schwarz et al., 2009; 15]. These findings underscore the role of breastfeeding as a modifiable behavior with lasting effects on maternal health.
Gestational Diabetes and Cardiovascular Risk
Observations show an apparent connection between cardiovascular disease (CVD), gestational diabetes mellitus (GDM), and the associated increased risk of developing type 2 diabetes mellitus (T2DM). In fact, women with GDM face a 9.6-fold greater risk of T2DM compared to those without GDM, with a cumulative risk of 25.8% within 15 years of diagnosis (Lee et al., 2007). A meta-analysis further demonstrated a 7.43-fold increased risk of T2DM among women with GDM, with some cohorts reporting relative risks exceeding 12.6 depending on follow-up duration and additional risk factors [17]. The progression to T2DM is most pronounced in the postpartum period, with approximately 20% of women developing T2DM within nine years after pregnancy, and the highest risk observed within the first nine months postpartum (Spurgeon, 2008). The absolute risk of T2DM after GDM is estimated at 17%, with an 8.3-fold higher risk compared to women without GDM (Dennison et al., 2020). Key predictive factors for T2DM progression include higher pre-pregnancy BMI, insulin use during pregnancy, and elevated fasting glucose levels during gestation (Rayanagoudar et al., 2016). Given the vigorous relationship between GDM and T2DM, postpartum care should emphasize glucose monitoring and metabolic health interventions to mitigate future cardiovascular risks. Early lifestyle modifications and targeted therapies may reduce the risk of progression to T2DM and subsequent CVD in this high-risk population and those with limited access to healthcare.

Source: Sheiner, E. (2020). Gestational Diabetes Mellitus: Long-Term Consequences for the Mother and Child. Frontiers in Clinical Diabetes and Healthcare, 1, 546256. DOI: 10.3389/fcdhc.2020.546256
Chart Summary: Women with a history of gestational diabetes mellitus (GDM) face a 7-fold risk of type 2 diabetes, with 18.9 % developing it within 9 years. They also have a 9% risk of cardiovascular disease and a 10% risk of renal complications, including chronic renal failure. These findings highlight the need for postpartum monitoring and preventive care.
Breastfeeding facilitates cardiovascular recovery through metabolic regulation, blood pressure reduction, and lipid profile improvement. Women breastfeeding for at least six months have a 24% lower risk of hypertension and a 21% reduced risk of type 2 diabetes (Rameez et al., 2019; Aune et al., 2014). Hormonal mediators like oxytocin enhance vasodilation and stress resilience, further supporting maternal health (Grewen & Light, 2011; Engert et al., 2016). Highlighting and integrating these protective factors into postpartum counseling can play a pivotal role in reducing long-term cardiovascular risk and promoting overall maternal health.
The Importance of Breastfeeding Duration
Research consistently demonstrates that the duration of breastfeeding significantly influences cardiovascular outcomes. Women who breastfeed for at least six months experience a 21% lower risk of hypertension and a 24% reduced risk of type 2 diabetes compared to those who do not breastfeed (Rameez et al., 2019). Prolonged breastfeeding has also been linked to improved glucose metabolism and reductions in maternal blood pressure and cholesterol levels (Aune et al., 2014; Tschiderer et al., 2022).
These findings emphasize the long-term health benefits of breastfeeding not only for infants but also for mothers. Promoting extended breastfeeding as part of postpartum care can serve as a critical strategy in reducing chronic disease risks through improved metabolic and cardiovascular health.
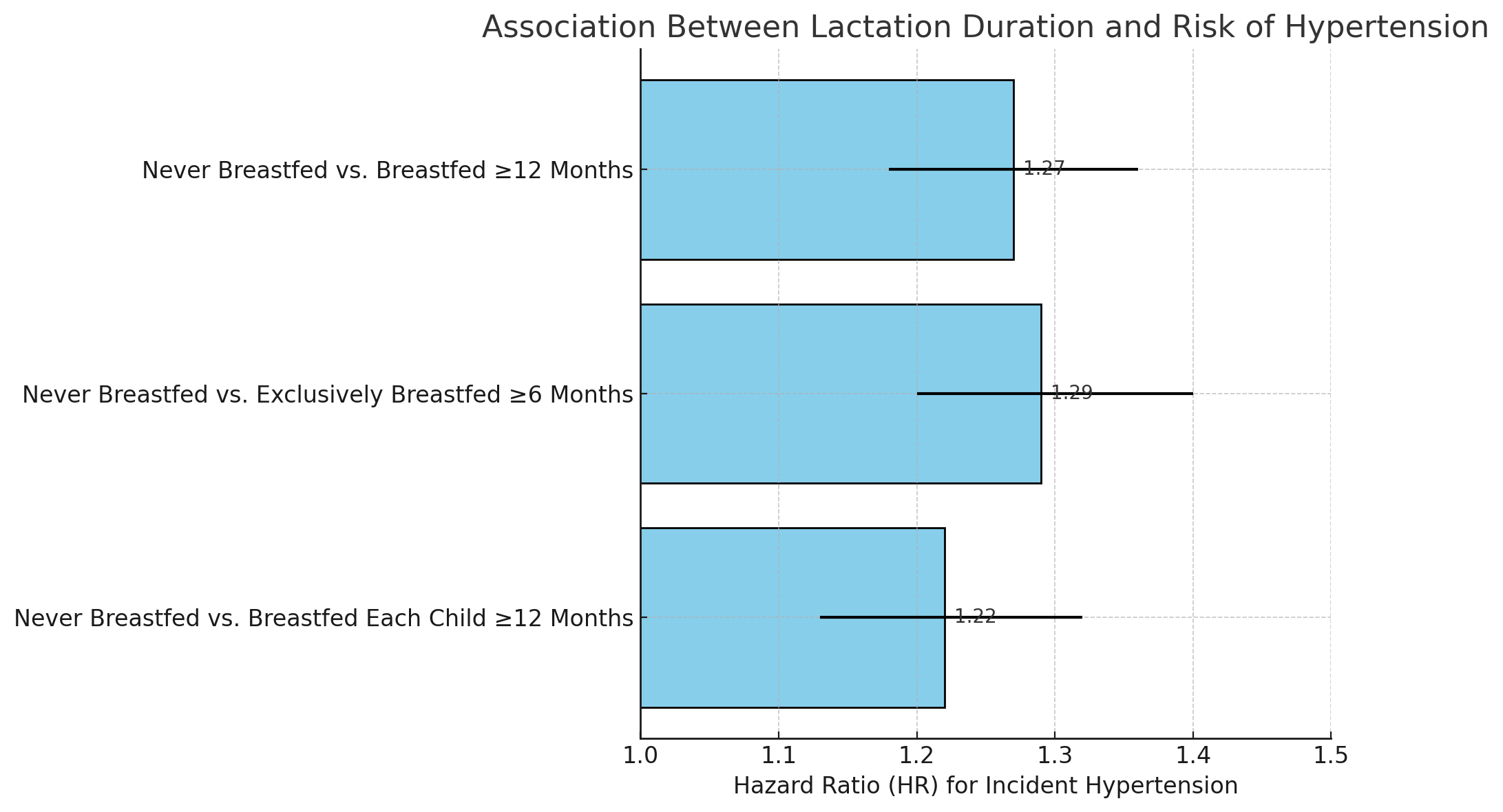
Source: Stuebe AM, Rich-Edwards JW, Willett WC, et al. Duration of lactation and incidence of maternal hypertension: A prospective cohort study. Obstet Gynecol. 2021;137(3):508–516.
Chart Summary: Women who never breastfed had a 1.27-fold increased risk of hypertension compared to those breastfeeding their first child for ≥12 months, 1.29-fold compared to those exclusively breastfeeding ≥6 months, and 1.22-fold compared to those breastfeeding each child for ≥12 months. Error bars indicate 95% confidence intervals, highlighting breastfeeding's protective effect against hypertension.

Chart Sources:
Ren X, Wang H, Hao J, et al. Lactation and stroke risk in women. JAMA Network Open. 2022;5(4):e221569.
Schwarz EB, Ray RM, Stuebe AM, et al. Duration of lactation and risk factors for maternal cardiovascular disease. Obstet Gynecol. 2009;113(5):974–982.
Stuebe AM, Rich-Edwards JW, Willett WC, et al. Duration of lactation and incidence of maternal hypertension: A prospective cohort study. Obstet Gynecol. 2021;137(3):508–516.
Natland ST, Nilsen TI, Midthjell K, et al. Duration of lactation and risk of maternal hypertension: A population-based study. Am J Epidemiol. 2012;175(9):957–965.
Lactation and Cardiovascular Recovery
Lactation offers significant cardiovascular benefits, extending the adaptations initiated during pregnancy and promoting long-term metabolic recovery. Breastfeeding has been shown to lower blood pressure, improve lipid profiles, and regulate inflammatory markers, all of which contribute to reduced cardiovascular disease (CVD) risk (Christensen et al., 2023). Notably, the presence of n-3 long-chain polyunsaturated fatty acids in breast milk has been linked to lower systolic and diastolic blood pressure in boys and improved lipid profiles in girls, highlighting potential sex-specific benefits (Bruun et al., 2019).
Postpartum studies indicate that breastfeeding for at least six months significantly reduces indicators of metabolic syndrome, including lower triglyceride levels, improved HDL cholesterol, and decreased blood pressure, particularly in women with prior pregnancy complications (Yu et al., 2021). Furthermore, long-term research suggests that breastfeeding is associated with improved cardiometabolic markers, such as reduced C-reactive protein levels and lower LDL cholesterol. These benefits are especially pronounced in women with a history of hypertensive disorders during pregnancy, underscoring lactation’s restorative effects on cardiovascular health (Magnus et al., 2023).
Promoting breastfeeding not only benefits infant health but also aligns with public health objectives to reduce maternal cardiovascular risks. Incorporating lactation support into postpartum care may serve as a cost-effective intervention to improve long-term outcomes for women, particularly those with a history of adverse pregnancy outcomes.
Hormonal Mechanisms in Cardiovascular Recovery
Hormones such as prolactin and oxytocin play pivotal roles in reducing cardiovascular stress and promoting vasodilation during and after pregnancy. Oxytocin, a well-established cardiovascular hormone, enhances vasodilation and mitigates stress reactivity by lowering norepinephrine levels and accelerating vagal recovery (Grewen & Light, 2011; Engert et al., 2016). Elevated plasma oxytocin levels are associated with improved cardiac function and reduced cortisol levels, contributing to faster recovery from physiological and emotional stress.
Prolactin, regulated by oxytocin, further supports emotional resilience and stress adaptation, particularly during the peripartum period. Increased prolactin receptor activity has been linked to reduced neuroendocrine stress responses, highlighting its dual role in cardiovascular and emotional health (Torner & Neumann, 2002). Together, oxytocin and prolactin offer promising therapeutic targets for managing stress-related cardiovascular and emotional disorders, underscoring the interconnected benefits of lactation.
Emerging biomarkers, including placental growth factor (PlGF) and C-reactive protein (CRP), offer promising avenues for early identification of at-risk women. Elevated inflammatory and angiogenic markers during pregnancy are linked to postpartum vascular dysfunction, emphasizing the potential of biomarker-guided care (Zeisler et al., 2016; 27].
Role of Biomarkers in Maternal Cardiovascular Health
Emerging evidence underscores the role of biomarkers in linking pregnancy complications to long-term cardiovascular disease (CVD). Placental growth factor (PlGF) and soluble FMS-like tyrosine kinase-1 (sFlt-1), key markers of angiogenic imbalance, have been associated with endothelial dysfunction and arterial stiffness, both precursors to atherosclerosis (Zeisler et al., 2016). Elevated levels of C-reactive protein (CRP), a marker of chronic inflammation, are predictive of hypertension and coronary artery disease (Vaughn et al., 2020). These biomarkers hold promise for early detection and intervention, enabling personalized approaches to maternal cardiovascular care.
Biomarker studies have further highlighted the risks associated with hypertensive disorders of pregnancy (HDP). Women with HDP often exhibit elevated postpartum levels of CRP, IL-6, and urine microalbumin-to-creatinine ratio, with these changes persisting up to 12 months postpartum [27]. Similarly, angiogenic markers such as sFlt-1 have been linked to adverse cardiovascular profiles, including increased left ventricular hypertrophy and blood pressure, supporting their role in postpartum cardiovascular monitoring (Visser et al., 2014).
Long-term studies also reveal sustained elevations in vascular dysfunction markers, such as SE-selectin and PAPPA, in women with a history of preeclampsia, with these elevations persisting for a decade postpartum (Drost et al., 2014). These findings emphasize the importance of embracing biomarker monitoring in postpartum care, particularly for women with a history of pregnancy complications.
Inflammatory biomarkers play a critical role in understanding maternal health during and after pregnancy. For example, in women with gestational diabetes mellitus (GDM), altered cytokine profiles (e.g., IL-6, IL-10, and IL-18) have been closely associated with postpartum glucose intolerance and other metabolic complications [32]. Elevated levels of CRP and IL-6 also correlate with vascular dysfunction and increased cardiovascular risk, particularly in women with HDP [28].
Environmental factors, such as exposure to endocrine-disrupting chemicals (EDCs) during pregnancy, further exacerbate inflammation. Persistent exposure to chemicals like PBDEs and PFASs has been linked to elevated IL-6 and TNF-α levels, with the impact more pronounced in obese women and during pregnancy compared to postpartum periods [33]. These findings highlight the interplay between environmental and biological factors in maternal cardiovascular health.
In addition to inflammatory markers, cardiac biomarkers like high-sensitivity troponin I (hs-TnI) and B-type natriuretic peptide (BNP) have shown significant postpartum changes. These biomarkers correlate with echocardiographic measures of cardiac morphology, such as increased left ventricular mass and atrial volume, underscoring their potential utility in monitoring postpartum cardiovascular risks [34]. Together, these biomarkers provide actionable insights for early detection and management of pregnancy-related cardiovascular complications.

Summary: Pregnancy complications such as preeclampsia, gestational diabetes, and hypertension significantly increase the risk of cardiovascular disease, with fold changes visualized to highlight these impacts. Breastfeeding duration also plays a protective role, with longer durations (>12 months) associated with substantial reductions in hypertension and stroke risk compared to shorter durations (<6>
Chart Sources:
Zeisler H, Llurba E, Chantraine F, et al. Predictive value of the sFlt-1 ratio in women with suspected preeclampsia. N Engl J Med. 2016;374(1):13–22.
Sukmanee T, Phunthikaphadr U, Phadungkiat N, et al. Cardiovascular biomarkers in women with hypertensive disorders of pregnancy (HDP). Consensus. 2023.
Zieleniak A, Bogacka I, Wsół B, et al. Inflammatory cytokines and metabolic changes postpartum in women with GDM. Front Endocrinol. 2022;13:826537.
Drost JT, van Eyck J, Schalij MJ, et al. Novel biomarkers in women with a history of preeclampsia. Consensus. 2014.
Integration of Findings into Clinical Practice
The findings emphasize the need for integrating pregnancy and lactation history into standard cardiovascular risk assessments. Adverse pregnancy outcomes (APOs), such as preeclampsia and gestational diabetes, are strongly associated with long-term risks of chronic hypertension, ischemic heart disease, and stroke. These conditions should prompt clinicians to consider postpartum women as high-risk individuals who require targeted monitoring and early intervention. Biomarker screening, particularly for elevated CRP and PlGF, could be included as part of routine postpartum care to detect cardiovascular risks early.
Postpartum follow-ups could be expanded to include comprehensive cardiovascular evaluations, particularly for women with APOs. Current postpartum care often focuses on immediate physical recovery and infant health, neglecting long-term maternal risks. Implementing these evaluations could significantly reduce morbidity and mortality associated with undiagnosed cardiovascular conditions. Clinicians should integrate pregnancy and lactation history into cardiovascular risk assessments and consider long-term follow-up for women with adverse pregnancy outcomes.
Recommendations for Public Health Interventions
To address disparities in maternal health outcomes, public health strategies should focus on expanding access to postpartum care for underserved populations. Research has shown that socioeconomic factors, such as income and education, significantly influence access to care and subsequent health outcomes. Policies aimed at extending Medicaid coverage and providing affordable access to postpartum clinics could help bridge these gaps and improve access for underserved populations.
Educational campaigns targeting at-risk populations can also play a crucial role. For example, promoting the cardiovascular benefits of breastfeeding among women with hypertensive disorders could encourage higher rates of lactation, thereby reducing long-term risks. Similarly, healthcare providers could receive training to recognize APOs as critical risk factors and incorporate them into cardiovascular health discussions with patients.
Addressing Demographic and Socioeconomic Disparities
There is a pressing need to address the disproportionate impact of cardiovascular risks on women from marginalized groups. Studies have shown that Black and Hispanic women are more likely to experience APOs and less likely to receive adequate postpartum care. Tailored interventions, such as community-based health programs and telemedicine options, could help reduce these disparities. Furthermore, efforts to improve diversity in clinical research would ensure that findings are generalizable to broader populations.
Limitations and Future Research
This study has several limitations, including potential selection bias from reliance on electronic health records, publication bias in the systematic review, and the absence of longitudinal data spanning decades. Biomarkers discussed require further validation in larger, diverse cohorts, and self-reported lactation data may introduce recall bias. Additionally, genetic, lifestyle, and environmental factors were not fully explored.
Future research should focus on long-term, multi-ethnic studies to validate biomarkers like CRP and PlGF, investigate epigenetic changes during pregnancy, and assess interactions between genetic predispositions and environmental factors. Expanding biomarker-guided care into clinical practice and evaluating its cost-effectiveness will also be critical for advancing maternal cardiovascular health.
Pregnancy and lactation are critical, yet underutilized, windows for understanding and addressing maternal cardiovascular health. Adverse pregnancy outcomes, such as preeclampsia and gestational diabetes, serve as important predictors of long-term cardiovascular risks, while lactation offers unique protective benefits that extend beyond the postpartum period. These reproductive milestones underscore the need for a paradigm shift in how maternal cardiovascular health is assessed and managed.
The integration of pregnancy and lactation history into routine cardiovascular risk assessments, coupled with biomarker-guided interventions, has the potential to transform postpartum care. By leveraging these insights, healthcare providers can identify at-risk women early, implement targeted prevention strategies, and address disparities in care that disproportionately affect underserved populations.
Moreover, advancing research into inflammatory and angiogenic biomarkers and their links to long-term cardiovascular outcomes will deepen our understanding of the pathophysiological mechanisms at play, paving the way for personalized medicine approaches. Public health initiatives that prioritize equitable access to postpartum care and promote breastfeeding as a cardiovascular intervention will further amplify these benefits, ensuring better outcomes across diverse populations.
Addressing maternal cardiovascular health is not just a clinical imperative but a public health priority. By focusing on this critical window, we can break the cycle of delayed diagnosis and treatment, improve the quality of life for mothers, and reduce the burden of cardiovascular disease across generations. The time to act is now—transforming pregnancy and lactation from overlooked transitions into pivotal opportunities for lifelong cardiovascular health.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
