
Research Article | DOI: https://doi.org/10.31579/2768-0487/168
1Department of Haematology and Blood Transfusion, Federal Medical Centre, Umuahia, Abia State, Nigeria.
2Department of Haematology and Blood Transfusion, Abia State University, Uturu, Nigeria.
3Department of Haematology and Immunology, College of Medicine, University of Nigeria, Ituku-Ozalla Campus, Enugu State, Nigeria.
4Department of Haematology and Blood Transfusion, University of Abuja, Gwagwalada, Nigeria.
5Department of Biochemistry, Lead City University, Ibadan, Oyo State, Nigeria.
*Corresponding Author: Chikezie Kelechi, Department of Haematology and Blood Transfusion, Federal Medical Centre, Umuahia, Abia State, Nigeria.
Citation: Chikezie K, Uche CL, Ocheni S, Nwabuko OC, Agwu O et al., (2025), Preeclampsia and its Clinico-Laboratory Markers: A Comparative Study Among Pregnant Women in Enugu State, Nigeria, Journal of Clinical and Laboratory Research, 8(2); DOI:10.31579/2768-0487/168
Copyright: © 2025, Chikezie Kelechi. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 11 February 2025 | Accepted: 18 February 2025 | Published: 26 February 2025
Keywords: preeclampsia; haematological profile; blood pressure; platelet count; proteinuria
Background: Preeclampsia remains a significant cause of maternal and fetal morbidity and mortality globally. This study aimed to assess the clinico-laboratory markers of pregnant women with preeclampsia in Enugu State, Nigeria.
Methods: A cross-sectional descriptive study was conducted among pregnant and 24–48-hour post-delivery women with and without preeclampsia at the University of Nigeria Teaching Hospital (UNTH) and Enugu State University Teaching Hospital (ESUTH). Participants were recruited based on inclusion and exclusion criteria, and socio-demographic data, clinical history, blood pressure, platelet count, and urine protein levels were recorded. Ethical approval was obtained, and informed consent was secured.
Results: The study included 156 participants, equally divided into preeclamptic (n=78) and non-preeclamptic (n=78) groups. The mean age distribution was similar between groups (21–40 years: 89.8%). Preeclamptic women exhibited significantly higher proteinuria levels (+2: 74.4%; +3: 25.6%) compared to non-preeclamptic women (Nil: 98.7%, +1: 1.3%) (p<0.001). Platelet counts were significantly lower in preeclamptic women (<90 x 10⁹/L: 25.6%) compared to non-preeclamptic women (0.0%) (p<0.001). Blood pressure readings indicated that 87% of preeclamptic women had values >150/100 mmHg, while 97.4% of non-preeclamptic women had BP <140/90 mmHg (p<0.001). A family history of preeclampsia was more prevalent among preeclamptic women (2.6% vs. 0.0%) but was not statistically significant (p=0.27).
Conclusion: The study highlights significant haematological and 'serologic' alterations among preeclamptic women, particularly concerning proteinuria, platelet count, and blood pressure. These findings reinforce the need for early detection and monitoring of these parameters to improve maternal and fetal outcomes in Enugu State, Nigeria.
Preeclampsia is a multifaceted hypertensive disorder unique to pregnancy, typically emerging after 20 weeks of gestation [1]. It is clinically characterized by elevated blood pressure and often accompanied by proteinuria. The condition significantly contributes to maternal and perinatal morbidity and mortality worldwide, with a pronounced impact in low- and middle-income countries. In Nigeria, the prevalence of preeclampsia varies widely, ranging from 2% to 16.7%, depending on the population studied [2].
The pathogenesis of preeclampsia is complex and not fully elucidated. It is believed to involve abnormal placentation, leading to systemic endothelial dysfunction and a cascade of clinical manifestations affecting multiple organ systems. Risk factors include primigravidity, advanced maternal age, obesity, multiple gestations, and a history of certain medical conditions such as chronic hypertension and diabetes mellitus [3].
In Enugu State, Nigeria, studies have reported varying prevalence rates of preeclampsia. For instance, a study conducted at the University of Nigeria Teaching Hospital (UNTH) in Enugu observed a prevalence rate of 3.3% over a four-year period [4]. This variability underscores the need for localized research to understand the burden of the disease better and to develop targeted interventions.
The clinical presentation of preeclampsia can range from mild to severe forms, with potential progression to eclampsia, characterized by the onset of seizures. Laboratory investigations play a crucial role in the diagnosis and management of preeclampsia. Common laboratory markers include elevated liver enzymes, thrombocytopenia, and indicators of renal impairment such as increased serum creatinine levels. Recent studies have explored the utility of various biomarkers in predicting and diagnosing preeclampsia. For example, angiogenic factors like soluble fms-like tyrosine kinase-1 (sFlt-1) and placental growth factor (PlGF) have shown promise in early detection [3].
Despite advancements in understanding the pathophysiology and management of preeclampsia, it remains a significant cause of adverse maternal and fetal outcomes in Nigeria. A systematic review and meta-analysis highlighted the substantial burden of preeclampsia and eclampsia in the country, emphasizing the need for improved healthcare strategies to mitigate associated complications and mortality rates [3].
Given the heterogeneity in the clinical presentation and progression of preeclampsia, there is a critical need for comparative studies focusing on clinico-laboratory markers among pregnant women in different regions, including Enugu State. Such research could provide valuable insights into region-specific risk factors, enhance early detection, and inform tailored management protocols to improve maternal and fetal outcomes.
Study Design
The study is a cross-sectional descriptive study involving pregnant and 24-48 hours post-delivery women with preeclampsia and those without the disease receiving antenatal care at UNTH and ESUTH, Enugu.
Study Area
The study was conducted in the Obstetrics and Gynaecology Departments of the University of Nigeria Teaching Hospital (UNTH) Ituku-Ozala, and Enugu State University Teaching Hospital (ESUTH), Park lane, GRA, both in Enugu state. These are the two Teaching Hospitals in Enugu state. The samples were analysed in the Haematology laboratory of UNTH Enugu.
Study Population
Subjects were pregnant women diagnosed with preeclampsia as defined by WHO25 (BP ≥ 140/90mmhg and proteinuria of ≥ 2+ in pregnant women of 20 weeks gestation and above as well as those 24-48 hours post-delivery) and those with normal pregnancy recruited at the antenatal clinics and wards (antenatal, postnatal and labour wards) of UNTH and ESUTH.
Inclusion Criteria
Women who are pregnant or 24-48 hours post-delivery with an established diagnosis of preeclampsia were recruited as the study group, while women who do not have preeclampsia or any other hypertensive and medical diseases who are above 20 weeks of gestation or 24-48 hours post-delivery were recruited as the control group.
Exclusion Criteria
Pregnant women with hypertensive disorders of pregnancy other than preeclampsia or other diagnosed morbidities and pregnant women below 20 weeks of gestation were excluded from the study. Previously transfused pregnant women were also excluded from the study.
The duration of the study was twenty-four months.
Sampling Method
Cases and controls were recruited in a non-randomized fashion after confirming from the participants that they had not been earlier recruited for this study. The preeclamptic group was first recruited, and subsequently, the non-preeclamptic group was recruited. The non-preeclamptic group was matched with the preeclamptic group for age range, parity and total number on both sides.
Sample Size Determination
The sample size was determined using the formula for comparison of two proportions [5]:
n= 2(Zα/2+ Zβ)2 P(1-P)/(P1-P2)2, where:
n= minimum sample size
Zα/2 = critical value of the normal distribution at α/2
Zβ = critical value of the normal distribution at β
P= pooled prevalence (prevalence in case group, P1 + prevalence in control group, P2)
P1-P2= difference in the proportion of events in two groups
To calculate the sample size (using the Z table), Zα/2 = 1.64 at 90% confidence interval and Zβ = 0.84 for a power of 80%. Taking P1 to be 28% (0.28) and P2 to be 12% (0.12) from the findings of Mital et al. [6] on the presence of AB blood group among preeclamptic (case) and non-preeclamptic (control) pregnant women in India, the sample size is calculated thus:
n= 2(1.64 + 0.84)2 0.2(1-0.2)/(0.16)2
n= 12.3 x 0.16/0.0256 =76.88
The calculated minimum sample size was approximately 77 for each group of the study.
Detailed clinical, pertinent personal history and other relevant information were collected by the researcher/assistant from clinical/ward records and the patients or their caregivers using a well-structured questionnaire specifically designed for this study. The blood pressure of all participants was tested and reported. Whole blood samples were collected from the study and control groups at recruitment and used for the determination of platelet counts. Urine was also collected for analysis.
All data collected from the study were cleaned, coded, entered into the computer on a pre-designed Excel spreadsheet and analysed using the statistical package for Social Sciences (SPSS) computer software version 21. Also, quantitative data were summarized using mean ± standard deviation (SD), median, mode and range; and outcomes were presented in tables and figures. Qualitative data were presented in proportions. Differences in mean between the cases and the control were analysed using the student t-test, while differences in proportions and test of association were done using the chi-squared test. All tests were two-sided and the statistical significance was considered to be at a probability (p) value of <0.05.
The socio-demographic characteristics of pre-eclamptic and non-pre-eclamptic women were compared in Table 1. Age distribution showed no significant difference between the two groups, as 43.6% of both groups were aged 21-30 years, and 46.2% were aged 31-40 years, with a p-value of 1.00. Education levels revealed that 60.3% of all women had tertiary education, with no significant differences between the groups (p = 0.82). Occupational differences were also insignificant (p = 0.55), with most women in both groups being civil servants (35.9%) and traders (23.1%). Religious affiliation showed a similar trend, with 93.6% of all women being Christian and no significant difference between the groups (p = 0.51). Ethnicity was predominantly Igbo (96.2%) across both groups.
Regarding the history of preeclampsia, Figure 1 shows that none of the non-preeclamptic women had a previous history of preeclampsia, while 15.4% of the preeclamptic women reported a previous occurrence, a statistically significant difference (p < 0.001). Figure 2 highlights family history findings, showing that 25.6% of preeclamptic women had a family history of preeclampsia, compared to 25.0% in the non-preeclamptic group, with no significant difference (p = 0.27).
Clinico-laboratory parameters are presented in Figures 3-5. Urine protein findings (Figure 3) were significantly different, with 98.7% of non-preeclamptic women showing no proteinuria, compared to 74.4% of preeclamptic women showing +2 proteinuria, and 25.6% showing +3 proteinuria (p <0.001). Platelet count findings in Figure 4 also showed significant differences, with 49.0% of non-preeclamptic women falling within the 151-300 x 109 range, while preeclamptic women were more likely to be in the 90-150 x 109 range (43.8%) (p < 0.001). Blood pressure findings (Figure 5) revealed that all non-preeclamptic women had normal blood pressure (<140/90), while 33.0% of preeclamptic women had blood pressure >160/100, a statistically significant difference (p< 0.001).
| Characteristic | Pre-eclamptic women n=78 (%) | Non pre-eclamptic women n=78 (%) | All Women n=156 | χ2 | p-value |
| Age (in years) | |||||
| 21-30 | 34 (43.6) | 34 (43.6) | 68 (43.6) | ||
| 31-40 | 36 (46.2) | 36 (46.2) | 72 (46.2) | 0.00 | 1.00 |
| >40 | 8 (10.3) | 8 (10.3) | 16 (10.3) | ||
| Educational Status | |||||
| None | 2 (2.6) | 1 (1.3) | 3 (1.9) | ||
| Primary | 5 (6.4) | 6 (7.7) | 11 (7.1) | 0.93 | 0.82 |
| Secondary | 26 (33.3) | 22 (28.2) | 48 (30.8) | ||
| Tertiary | 45 (57.7) | 49 (62.8) | 94 (60.3) | ||
| Occupation | |||||
| Civil Servant | 30 (38.5) | 26 (33.3) | 56 (35.9) | ||
| Trader | 16 (20.5) | 20 (25.6) | 36 (23.1) | ||
| Work in private firm | 10 (12.8) | 6 (7.7) | 16 (10.3) | ||
| Farmer | 6 (7.7) | 4 (5.1) | 10 (6.4) | 3.08 | 0.55 |
| Others | 16 (20.5) | 22 (28.2) | 38 (24.4) | ||
| Religion | |||||
| Christian | 72 (92.3) | 74 (94.9) | 146 (93.6) | ||
| Muslim | 6 (7.7) | 4(5.1) | 10 ((6.4) | 0.43 | 0.51 |
| Tribe/ethnicity | |||||
| Igbo | 75 (96.2) | 75 (96.2) | 150 (96.2) | ||
| Hausa | 2 (2.6) | 3 (3.8) | 5 (3.2) | 1.58 | 0.45 |
| Yoruba | 1 (1.3) | 0 (0.0) | 1 (0.6) | df=1 |
Table 1: Socio-Demographic Characteristics

Figure 1: Data on the previous history of preeclampsia
Key: NPE- Non-preeclamptic; PE- Preeclamptic, p<0.001.
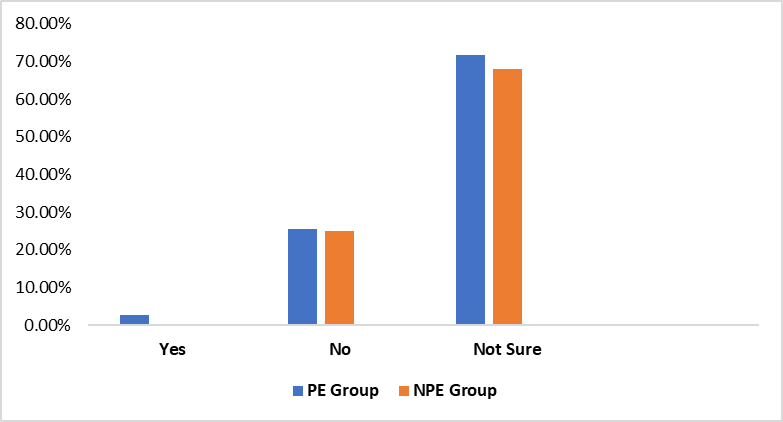
Figure 2: Family history of preeclampsia
Key: PE- Preeclamptic; NPE- Non preeclamptic; p=0.27
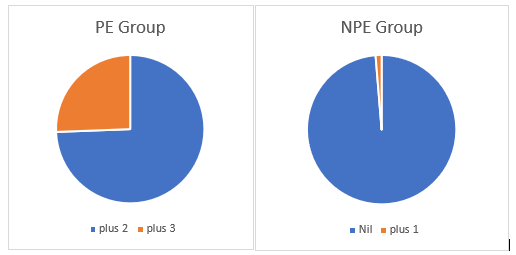
Figure 3: Urine protein findings in both groups
Key: PE- Preeclamptic (+2=74.4%; +3=25.6%); NPE- Non preeclamptic (Nil=98.7%; +1=1.3%) p<0.001
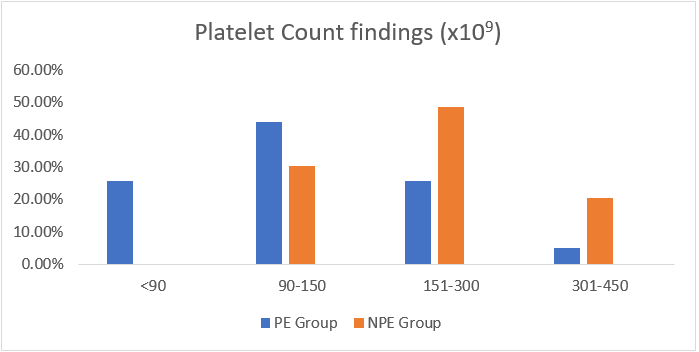
Figure 4: Platelet count findings in both groups
Key: PE- Preeclamptic; NPE- Non preeclamptic; p<0.001
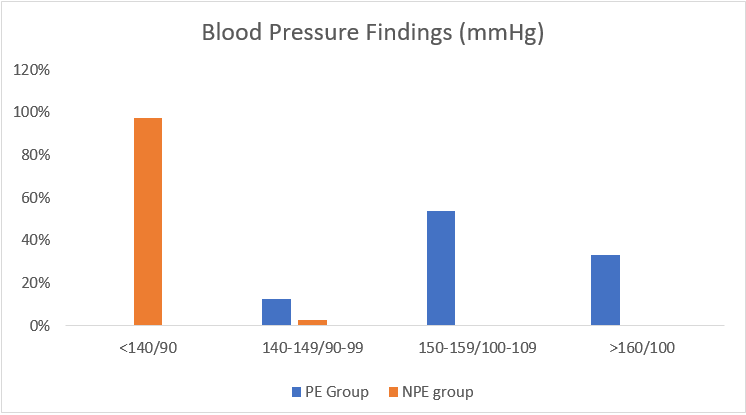
Figure 5: Blood pressure findings in both groups
Key: PE- Preeclampsia; NPE- Non preeclampsia; p<0.001
The socio-demographic characteristics of pre-eclamptic and non-pre-eclamptic women were compared in Table 1. Age distribution showed no significant difference between the two groups, as 43.6% of both groups were aged 21-30 years, and 46.2% were aged 31-40 years, with a p-value of 1.00. Education levels revealed that 60.3% of all women had tertiary education, with no significant differences between the groups (p = 0.82). Occupational differences were also insignificant (p = 0.55), with most women in both groups being civil servants (35.9%) and traders (23.1%). Religious affiliation showed a similar trend, with 93.6% of all women being Christian and no significant difference between the groups (p = 0.51). Ethnicity was predominantly Igbo (96.2%) across both groups.
Regarding the history of preeclampsia, Figure 1 shows that none of the non-preeclamptic women had a previous history of preeclampsia, while 15.4% of the preeclamptic women reported a previous occurrence, a statistically significant difference (p < 0.001). Figure 2 highlights family history findings, showing that 25.6% of preeclamptic women had a family history of preeclampsia, compared to 25.0% in the non-preeclamptic group, with no significant difference (p = 0.27).
Clinico-laboratory parameters are presented in Figures 3-5. Urine protein findings (Figure 3) were significantly different, with 98.7% of non-preeclamptic women showing no proteinuria, compared to 74.4% of preeclamptic women showing +2 proteinuria, and 25.6% showing +3 proteinuria (p <0.001). Platelet count findings in Figure 4 also showed significant differences, with 49.0% of non-preeclamptic women falling within the 151-300 x 109 range, while preeclamptic women were more likely to be in the 90-150 x 109 range (43.8%) (p < 0.001). Blood pressure findings (Figure 5) revealed that all non-preeclamptic women had normal blood pressure (<140/90), while 33.0% of preeclamptic women had blood pressure >160/100, a statistically significant difference (p< 0.001).
| Characteristic | Pre-eclamptic women n=78 (%) | Non pre-eclamptic women n=78 (%) | All Women n=156 | χ2 | p-value |
| Age (in years) | |||||
| 21-30 | 34 (43.6) | 34 (43.6) | 68 (43.6) | ||
| 31-40 | 36 (46.2) | 36 (46.2) | 72 (46.2) | 0.00 | 1.00 |
| >40 | 8 (10.3) | 8 (10.3) | 16 (10.3) | ||
| Educational Status | |||||
| None | 2 (2.6) | 1 (1.3) | 3 (1.9) | ||
| Primary | 5 (6.4) | 6 (7.7) | 11 (7.1) | 0.93 | 0.82 |
| Secondary | 26 (33.3) | 22 (28.2) | 48 (30.8) | ||
| Tertiary | 45 (57.7) | 49 (62.8) | 94 (60.3) | ||
| Occupation | |||||
| Civil Servant | 30 (38.5) | 26 (33.3) | 56 (35.9) | ||
| Trader | 16 (20.5) | 20 (25.6) | 36 (23.1) | ||
| Work in private firm | 10 (12.8) | 6 (7.7) | 16 (10.3) | ||
| Farmer | 6 (7.7) | 4 (5.1) | 10 (6.4) | 3.08 | 0.55 |
| Others | 16 (20.5) | 22 (28.2) | 38 (24.4) | ||
| Religion | |||||
| Christian | 72 (92.3) | 74 (94.9) | 146 (93.6) | ||
| Muslim | 6 (7.7) | 4(5.1) | 10 ((6.4) | 0.43 | 0.51 |
| Tribe/ethnicity | |||||
| Igbo | 75 (96.2) | 75 (96.2) | 150 (96.2) | ||
| Hausa | 2 (2.6) | 3 (3.8) | 5 (3.2) | 1.58 | 0.45 |
| Yoruba | 1 (1.3) | 0 (0.0) | 1 (0.6) | df=1 |
Table 1: Socio-Demographic Characteristics
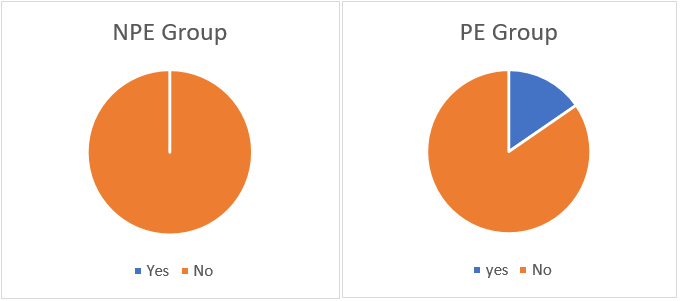
Figure 1: Data on the previous history of preeclampsia
Key: NPE- Non-preeclamptic; PE- Preeclamptic, p<0.001.
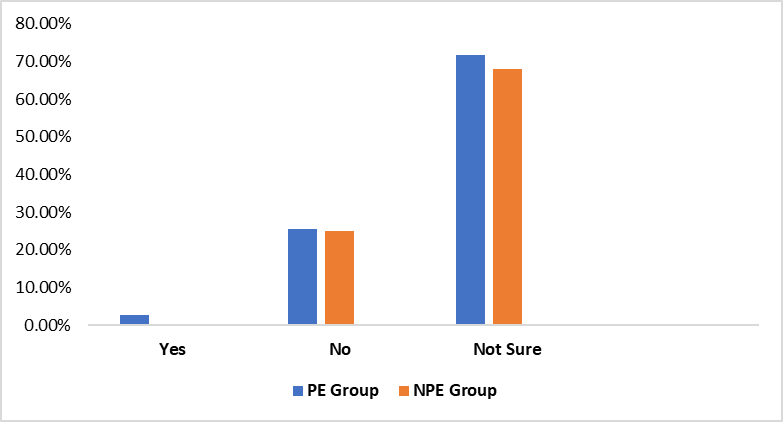
Figure 2: Family history of preeclampsia
Key: PE- Preeclamptic; NPE- Non preeclamptic; p=0.27
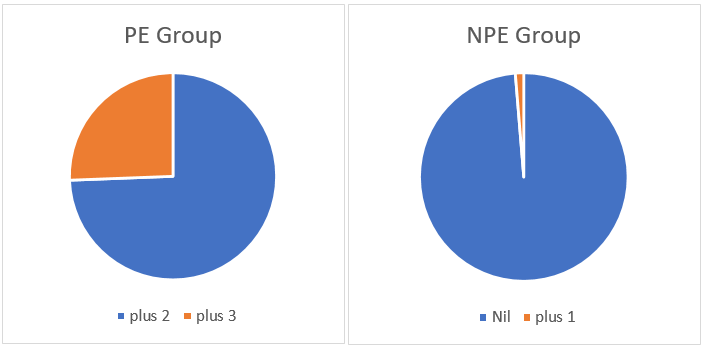
Figure 3: Urine protein findings in both groups
Key: PE- Preeclamptic (+2=74.4%; +3=25.6%); NPE- Non preeclamptic (Nil=98.7%; +1=1.3%) p<0.001
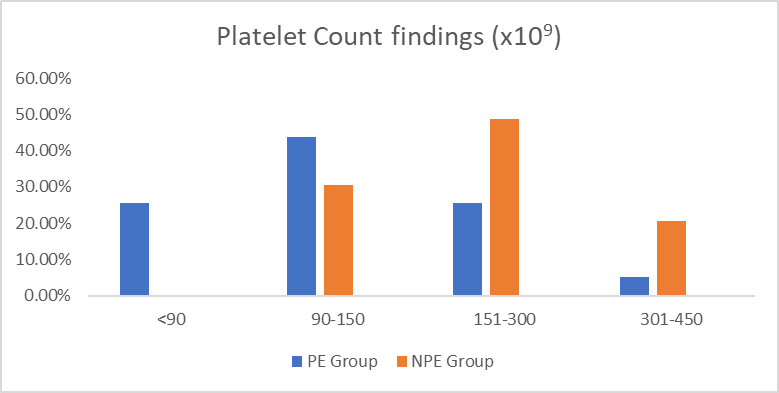
Figure 4: Platelet count findings in both groups
Key: PE- Preeclamptic; NPE- Non preeclamptic; p<0.001
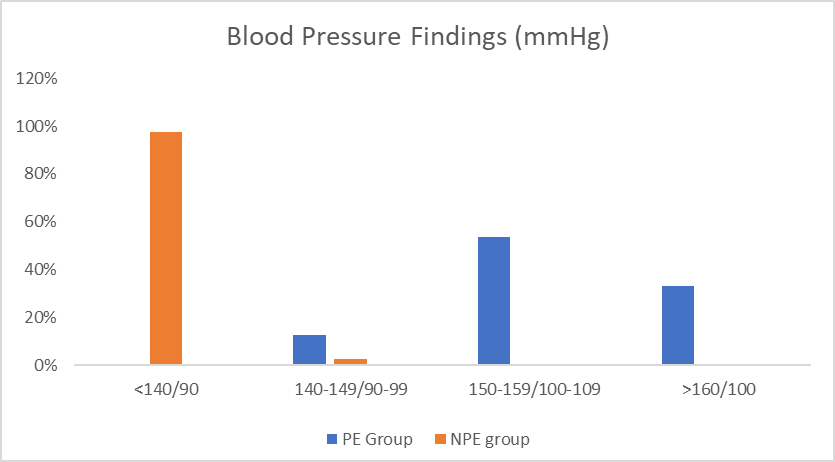
Figure 5: Blood pressure findings in both groups
Key: PE- Preeclampsia; NPE- Non preeclampsia; p<0.001
Preeclampsia is a hypertensive disorder of pregnancy characterized by elevated blood pressure and often proteinuria, posing significant risks to both maternal and fetal health. Understanding the socio-demographic, haematological, and serologic profiles of affected individuals is crucial for effective management and intervention strategies. The socio-demographic characteristics of the 'study participants'. indicate no statistically significant differences between pre-eclamptic and non-pre-eclamptic pregnant women across various parameters, including age, educational status, occupation, religion, and ethnicity. This suggests that socio-demographic variables may not be independent predictors of preeclampsia in this cohort. The majority of the participants in both groups were between 31-40 years old (46.2%), followed by those aged 21-30 years (43.6%). This aligns with studies conducted in Nigeria and other African countries, where preeclampsia is more prevalent among women in their reproductive prime [7]. However, other studies have reported a higher prevalence among women younger than 30 years, particularly primigravida [8]. The lack of statistical significance (P=1.00) in this study may suggest that age alone is not a strong independent risk factor, but rather interacts with other physiological and genetic predispositions. The majority of the participants had tertiary education (60.3%), with a slightly lower proportion in the pre-eclamptic group (57.7%) compared to the non-pre-eclamptic group (62.8%). This finding corroborates reports by Adewunmi et al. [9], who found that preeclampsia occurs across all educational levels, though lower education has been associated with increased risk due to limited health literacy and healthcare access [10]. Despite the variation in numbers, the difference was not statistically significant (P=0.82), indicating that education alone may not be a determinant of preeclampsia but may interact with other socio-economic factors. Occupational status varied among participants, with civil servants (35.9%) being the most represented. While more pre-eclamptic women were civil servants (38.5%) compared to non-pre-eclamptic women (33.3%), the difference was not statistically significant (P=0.55). This contrasts with findings from Spadarella et al. [11], who suggested that physically demanding jobs might contribute to increased stress levels, a known risk factor for preeclampsia. However, the relatively even distribution across occupational categories in this study suggests that occupation alone may not be a primary determinant. Christianity was the predominant religion (93.6%), consistent with the religious demographics of Enugu State. The slight difference in the proportion of Muslims between groups was not statistically significant (P=0.51). Similarly, ethnicity was predominantly Igbo (96.2%), reflecting the study’s location. Prior studies [12] have suggested a potential genetic predisposition to preeclampsia among certain ethnic groups, but the lack of significant variation here suggests that ethnicity may not be a major risk factor in this cohort. A history of preeclampsia in previous pregnancies and family history were both more common among pre-eclamptic women. This finding is consistent with studies indicating that a prior history of preeclampsia increases recurrence risk in subsequent pregnancies [13]. Additionally, genetic predisposition has been implicated, with studies suggesting that daughters of women with preeclampsia have a higher likelihood of developing the condition [14]. These findings emphasize the need for early screening and close monitoring of women with a history of preeclampsia. The findings of this study align with global and regional research on the socio-demographic distribution of preeclampsia. For instance, a study by Bello et al. [15] in Northern Nigeria reported similar age and educational distributions but found a slightly higher prevalence of preeclampsia among women with lower educational attainment. In contrast, research conducted in high-income countries, such as that by Magee et al. [16], found a stronger association between low socio-economic status and preeclampsia, highlighting the role of healthcare accessibility and nutritional disparities. Furthermore, previous studies have indicated that factors such as obesity, hypertension, and gestational diabetes contribute significantly to the pathogenesis of preeclampsia [17]. The lack of significant differences in the socio-demographic characteristics in this study suggests that genetic, immunological, and environmental factors may have a more substantial role in preeclampsia development. The findings from this study indicate that 15.4% of preeclamptic women had a previous history of preeclampsia, whereas none of the non-preeclamptic women had such a history (p<0.001). This suggests a strong association between previous preeclampsia and its recurrence in subsequent pregnancies. Similar results have been documented in other studies. For instance, Smith et al. [18] reported that women with a prior history of preeclampsia had a significantly increased risk of developing the condition again, with recurrence rates ranging between 10% and 65%, depending on severity and management. Regarding family history, 2.6% of preeclamptic women had a known family history of preeclampsia, while 25.6% reported no family history, and 71.8% were unsure. Among non-preeclamptic women, none reported positive family history, 25% had no history, and 68% were unsure (p=0.27). These findings suggest a possible genetic predisposition to preeclampsia, though the high proportion of uncertainty highlights a gap in awareness. Consistent with our results, studies by Gray et al. [19] and McGinnis et al. [20] reported that a positive family history significantly increases preeclampsia risk, with heritability estimates ranging from 35% to 65%. Proteinuria is a hallmark of preeclampsia. Our study found that 74.4% of preeclamptic women had +2 proteinuria, while 25.6% had +3 proteinuria. In contrast, 98.7% of non-preeclamptic women had no proteinuria, and only 1.3% had +1 proteinuria (p<0.001). These results align with findings by Magee et al. [16], who noted that proteinuria levels of +2 or higher are strongly predictive of severe preeclampsia. Similarly, studies by Roberts et al. [21] and Fishel-Bartal et al. [22] support the role of proteinuria in diagnosing and assessing the severity of preeclampsia. Our study revealed significant thrombocytopenia in preeclamptic women, with 25.6% having platelet counts below 90 x 10⁹/L, 43.8% between 90-150 x 10⁹/L, 25.6% between 151-300 x 10⁹/L, and only 5.1% above 301 x 10⁹/L. Among non-preeclamptic women, none had platelet counts below 90 x 10⁹/L, 30% fell within 90-150 x 10⁹/L, 49% were within 151-300 x 10⁹/L, and 21% had platelet counts above 301 x 10⁹/L (p<0.001). Thrombocytopenia in preeclamptic women has been well-documented, with studies by Ananth et al. [23] and Tita et al. [24] reporting that platelet counts below 150 x 10⁹/L are significantly associated with severe preeclampsia and adverse maternal-fetal outcomes. Blood pressure assessment showed that none of the preeclamptic women had BP below 140/90 mmHg, 13% had readings between 140-149/90-99 mmHg, 54% had BP between 150-159/100-109 mmHg, and 33% had BP exceeding 160/100 mmHg. Conversely, 97.4% of non-preeclamptic women had BP below 140/90 mmHg, while 2.6% fell within the 140-149/90-99 mmHg range (p<0.001). These findings are in agreement with a meta-analysis by Lisonkova et al. [25], which showed that BP above 140/90 mmHg is a defining feature of preeclampsia and that BP readings exceeding 160/100 mmHg significantly increase the risk of maternal and fetal complications. The overall findings of this study reinforce existing literature on preeclampsia. The associations between prior history, family history, proteinuria, thrombocytopenia, and hypertension in preeclamptic women mirror findings from extensive research. Studies by Bartsch et al. (2019) and Roberge et al. (2020) further emphasize that early recognition of these factors can improve maternal and fetal outcomes. The significant statistical differences observed (p<0.001) underscore the clinical importance of monitoring these parameters in at-risk pregnant women.
The study highlights significant haematological and clinical alterations among preeclamptic women, particularly concerning proteinuria, platelet count, and blood pressure. These findings reinforce the need for early detection and monitoring of these parameters to improve maternal and fetal outcomes in Enugu, Nigeria.
KC, TN, SO conceptualized and designed the study. KC, OA and CJM were involved in data collection/acquisition and statistical analysis. KC, TN, SO, interpreted the results and together with CLU, AIA, CON were involved in the writing and revising of the manuscript for intellectual content. All authors read and approved the final manuscript and agreed to be accountable for all aspects of the work. All authors have accepted responsibility for the entire content of this manuscript and consented to its submission to the journal reviewed all the results and approved the final version of the manuscript.
Ethical Considerations: Ethical approval was obtained from the Health Research and Ethics committees of UNTH and ESUTH with reference numbers NHREC/05/01/2008B and ESUTHP/C-MAC/RA/034/vol-2163 respectively.
Informed Consent: Informed consent was obtained from all individuals included in this study, or their legal guardians or wards.
Declaration of Helsinki: The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013).
Availability of research data: Authors are available and ready to supply the data upon any request through the corresponding author.
Funding or financial support: The authors did not receive any funding or financial support for this study.
Conflict of Interest Statement: Authors have no conflict of interest to declare.
Acknowledgement: We acknowledge all the subjects who willingly participated in this study. We also acknowledge the efforts of Dr Ugochukwu Onyeonoro and Dr Ehijie Okoigun in the sample collection and data analysis.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
