
Research Article | DOI: https://doi.org/10.31579/2642-973X/012
1 Tingandogo University Hospital, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
2 Yalgado Ouédraogo University Hospital of Ouagadougou, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
3 Ouagadougou Health Sciences Research Institute, Department of Medical Biology and Public Health, Ouagadougou, Burkina Faso.
*Corresponding Author: Lompo Djingri Labodi, Tingandogo University Hospital, Health Sciences Training and Research Unit, Joseph Ki-Zerbo University, Ouagadougou, Burkina Faso.
Citation: Lompo D Labodi, Somé N Eric, Ouédraogo A Mariam, D Ousséni, N Christian, K Jean. (2021). Predictors of Functional Outcome at Three Months Post Stroke in a Third Level Hospital in Ouagadougou Burkina Faso. Brain and Neurological Disorders. 4(1); DOI:10.31579/2642-9730/012
Copyright: © 2021, Lompo Djingri Labodi, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 20 September 2021 | Accepted: 05 October 2021 | Published: 12 October 2021
Keywords: stroke; functional outcome; physiotherapy ; predictive factors
Aim/Background: The aim of our study was to identify the predictive factors of functional outcome at 3 months post stroke, at Tingandogo University Hospital, in Ouagadougou, Burkina Faso, in order to contribute to the improvement of the functional prognosis of patients suffering from stroke.
Materials and methods: This involved a hospital study, longitudinal prospective and anaytical, of patients hospitalized for stroke, from March 2015 to February 2016, at the Tingandogo University Hospital, in Ouagadougou, then followed in outpatient neurology, for at least 3 months, after discharge from hospital. The sociodemographic, clinical and CT characteristics of the patients on admission, the mortality at 3 months, and the evaluation of the functional outcome of the survivors at 3 months by the modified Rankin score (mRS) were analyzed. Motor functional outcome was considered favorable if mRS ≤ 2 and unfavorable if mRS ≥ 3. Multivariate analysis with logistic regression made it possible to identify independent predictors of functional outcome at 3 months post-stroke.
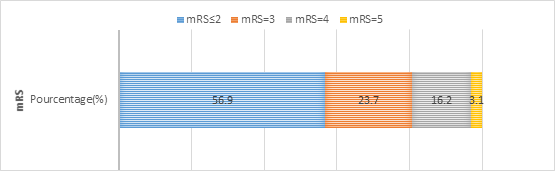
Results: A total of 232 patients were collected, i.e. 62.9% of cerebral infarction and 37.1% of intracerebral hemorrhage, with a male predominance (62.93%), an average age of 60.9 years +/- 14.5 years. On admission, 6% of patients were in a coma and 35.8% had severe to very severe neurological impairment. Motor physiotherapy indicated in 77.3% of patients was but only performed in 47.4% At 3 months post stroke, 27 patients had died (31%). Among the 160 surviving patients, 91 patients (56.9%) were autonomous or independent (mRS≤2) and 69 patients (43.1%) were still dependent (mRS≥3). The independent predictors of unfavorable functional outcome (mRS≥3) at 3 months post-stroke were: age ≥ 60 years (p = 0.007), pre-stroke disability (p = 0.032), severe neurological deficit at admission (p = 0.018), impaired alertness on admission (p = 0.005) and large infarcts (p=0.004).
Conclusion: Advanced age, pre-stroke disability, clinical and CT markers of the extent of brain damage, influence functional outcome at 3 months post-stroke in our context. Improving the quality of care for all patients, even the oldest, and better access to quality functional rehabilitation will help improve the functional prognosis of stroke patients.
Stroke is emerging as one of the leading causes of preventable adult death and disability worldwide [1, 2]. Stroke occurs about 15 years earlier in developing countries than in developed countries, suggesting a younger age of stroke patients in developing countries [3], and therefore, a larger expected number of patients survivors of young age, in full socio-professional activity. This finding underlines the interest of medical interventions that have demonstrated their effectiveness in reducing the frequency and severity of functional disability after stroke, such as primary prevention, early admission of patients to stroke units (SU), the early use of thrombolysis and / or thrombectomy and the importance of continuing functional readaptation and rehabilitation, in this context [4]. Unfortunately in underdeveloped countries in general and in sub-Saharan Africa (SSA) in particular, the delays in patient care, the weakness of health systems, marked in particular by the absence of SU, the unavailability of fibrinolysis and / or thrombectomy and the inaccessibility of patients to quality functional rehabilitation limit the chances of survival or functional recovery after stroke of patients in this region [4]. Thus in SSA, approximately 40 to 51.5% of stroke survivors recover their autonomy or independence, 3 months after the stroke [3, 5-7]. In contrast, in developed countries, only 12 to 20% of patients were still dependent at 3 months post-stroke [8].
Various studies on the functional outcome after stroke have revealed that most of the recovery (95%) takes place in the first three months after the stroke [1], then recovery continues, to a lesser extent, for several months, and up to 18 months afterwards [2]. This explains why most post-stroke clinical evaluations are usually done within three months, sometimes six months, rarely one year and beyond.
The identification of predictive factors of functional outcome after stroke in our context of countries with limited resources, would make it possible to develop pragmatic strategies for reducing the frequency and severity of functional sequelae and improving the socio-professional reintegration of patients stroke victims.
Among the predictive factors of functional outcome after stroke identified from the acute phase through the literature, the most robust and reproducible are advanced age, history of stroke, existence of a pre-existing disability, initial clinical severity, impaired alertness, the initial large volume of stroke [3, 9].
The aim of our study was to identify the predictive factors of functional outcome at 3 months post stroke, at Tingandogo University Hospital (TUH), in Ouagadougou, Burkina Faso.
This was an observational, prospective cohort, descriptive and analytical study, which took place from December 1, 2016 to May 30, 2018, at TUH, in Ouagadougou, Burkina Faso.
Inclusion criteria : The study concerned all patients aged ≥18 years, hospitalized in said Univesity Hospital for cerebral infarction or intracerebral hemorrhage (ICH) during the study period, confirmed by cerebral CT scan or encephalic MRI, then followed up in outpatient for at least 3 months after the stroke, as part of the neurological consultation for post-stroke follow-up. Patients in whom functional motor rehabilitation was indicated should also be treated in the various functional rehabilitation centers and / or physiotherapy or speech therapy practices in the city of Ouagadougou, for a period of at least 3 months after stroke. Each patient participating in the study had to give informed consent to participate in the study or, failing that, the consent of family member had to be obtained.
Non inclusion criteria : Were not included in our study all the patients whose diagnosis of stroke was not documented by neuroimaging (CT and / or encephalic MRI), those who had a diagnosis of cerebral venous thrombosis, TIA, or neurological pathologies other than stroke, those lost to follow-up before completing the 3-month post-stroke follow-up period, those who had not given their consent to participate in the study and patients who had important cognitive skills (Mini Mental State Examination <26>
Patient data was collected on individual files established for this purpose, upon admission to the emergency department, then completed during their hospital stay and continued throughout outpatient neurological follow-up and functional rehabilitation sessions in the post-hospital phase.
Study variables : Patients were collected consecutively during the study period. Upon admission of patients, their socio-demographic characteristics such as age, sex, socio-professional category; vascular risk factors, comorbidities, clinical data such as Glasgow score, NIHSS score, clinical neurological signs; biological data (glycemia, glomerular filtration rate, natremia, serum potassium, hemoglobin level, white blood cell count); the neuroradiological characteristics of stroke such as old scar lesions, early signs of cerebral ischemia, the nature and location of the stroke, associated neuroradiological complications (cerebral edema, mass effect, cerebral involvement, hemorrhagic rearrangement of the cerebral infarction, acute hydrocephalus, ventricular contamination of intracerebral hemorrhage), as well as the etiological diagnosis of the stroke, were informed. On discharge from hospitalization, the clinical course was assessed with survival or death as the primary endpoint, at the end of hospitalization, then at one month and finally at 3 months after stroke. In surviving patients, the modified Rankin score (mRS) was evaluated, at the end of hospitalization, at one month and at three months pst stroke, by a neurologist in collaboration with physiotherapists. It should be remembered that during the study period, Burkina Faso did not yet have a functional rehabilitation service coordinated by an physical medicine and rehabilitation doctor with physiotherapists, occupational therapists, speech therapists, neuropsychologists, etc. working in interdisciplinary teams).
Among the different modalities of functional rehabilitation, only physiotherapy was available and easily accessible throughout the city of Ouagadougou; it is practiced in the four university hospitals and in several physiotherapy practices and private clinics in the city of Ouagadougou. For these various reasons, only motor functional outcome was evaluated in the present study.
Data entry and analysis were performed using epi info 7.2 software, then STATA 15. Student's test was used to compare data means and Pearson's Chi² test to compare data percentages. The p-value ≤ 0.05 was considered to be the threshold of statistical significance. To determine the predictors of functional outcome, an univariate analysis was first performed to look for an association between socio-demographic, clinical, biological and neuroradiological characteristics present at admission and motor functional outcome at three months. Then, a multivariate analysis with the use of the step-by-step logistic regression model made it possible to identify the independent predictors of motor functional outcome at 3 months. Only variables with a p ≤ 0.20 during the univariate analysis were taken into account in the multivariate analysis.
The consent of the patients or that of their legal representatives, as well as the anonymous nature of the survey, were guaranteed before recruitment. The study protocol had been approved by the national ethics committee of Burkina Faso, then authorized by the General Management of the TUH.
Operational definitions:
The socio-professional categories have been classified as follows: farmers / workers / housewives ; craftsmen, traders, business leaders ; executives, higher intellectual professions ; intermediate professions / employees ; students ; retirees ; people who have never worked / disabled.
The National Institute of Health Stroke Scale (NIHSS) was used for the clinical assessment of patients.
The Glasgow score was used to assess the alertness of patients upon admission.
The Modified Rankin Score (mRS) was used for the assessment of functional outcome. It was rated from 0 to 6.
Motor functional outcome was considered favorable if mRS ≤ 2 and the patient considered independent or autonomous in activities of daily living.
Motor functional outcome was considered unfavorable if mRS ≥ 3 and the patient considered to be dependent in activities of daily living. In the event of death, the mRS = 6.
The cerebral infarction was judged to be large when it occupied at least 2/3 of the area of the Midle Cerebral Artery or the entire area of the Posterior Cerebal Artery (PCA) or the entire brainstem or the entire cerebellar hemisphere. It was judged to be moderate in size or small in all other cases.
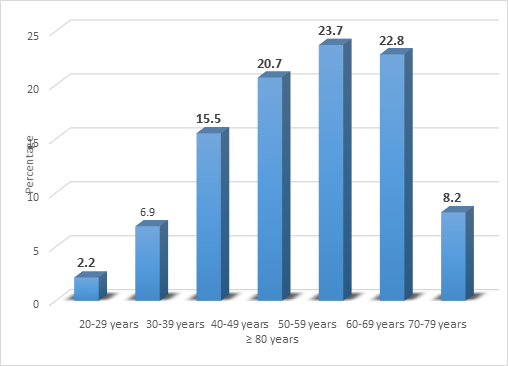
During the study period, 232 patients were collected; the average age was 60.9 +/- 14.5 years (range 26 and 99 years); the age group of 60 to 70 years, with 55 patients (23.7%) was the most represented (Figure 1).
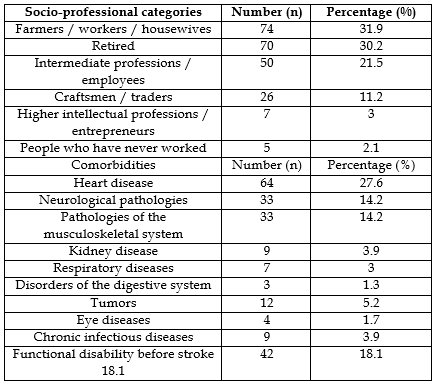
Male patients with 146 cases (62.9%), those in school with 128 cases (55.2%), or living with their spouse (married or in cohabitation) with 152 cases (65.5%), farmers / workers / housewives with 74 patients (31.9%), were the most numerous. Co-morbidities were found in 111 patients (47.8%), including heart disease with 64 cases (27.6%), pathologies of the musculoskeletal system and neurological pathologies with respectively 33 cases each (14.2%), were the most frequently encountered. Functional dependence before stroke was present in 42 patients (18.1%) (Table I).
Upon admission to the acute phase of stroke : 59 patients (25.4%) had impaired alertness [Glasgow coma scale (GCS) ≤ 14)], including 14 patients (6%) in a coma; 83 patients (35.8%) had a severe to very severe neurological deficit (NIHSS ≥ 17); 150 patients (64.9%) had an hemicorporeal motor deficit, dominated by hemiplegia, 89 cases (38.6%) and hemiparesis, 34 cases (14.8%); the right laterality of the motor deficit with 46 cases (47.4%) was more frequently reported. Dyshagia in 93 patients (70.2%), aphasia in 89 patients (38.5%), hemihypoesthesia in 85 patients (36.7%), were the main other clinical neurological signs present on admission (table II).

Hyperglycemia with 87 cases (37.5%), hyperleukocytosis with 58 cases (25%) and renal failure with 47 cases (20.3%), were the laboratory abnormalities most frequently found on admission. On cerebral CT, a cerebral infarction and an intracerebral hemorrhage (ICH) were found respectively in 146 patients (62.9%); infarctions of the middle cerebral artery (MCA) with 121 cases (82.9%) and deep ICH with 55 cases (64%), were the most frequent locations; large-volume infarctions with 52 cases (35.6%) and medium-volume ICHs (30-60 cc), with 38 cases (44.2%), were the most frequent; cerebral edema with 130 cases (56%) and mass effect with 136 cases (58.6%) were neuroradiolgic complications present at the outset on admission.
Embologenic heart disease and atheromatous stenosis of the supraortic trunks, found respectively in 40 patients (27.4%) and 37 patients (25.3%), were the most frequent etiologies of cerebral infarction. Cerebral microangiopathy due to chronic hypertension found in 62 patients (72.1%) was the main cause of ICH (Table III).
Laboratories abnormalities | Number (n) | Percentage (%) |
Hyperglycemia | 87 | 37.5 |
Hypoglycemia | 9 | 3.9 |
Hyperleukocytosis | 58 | 25 |
Leukopenia | 5 | 2.2 |
Anemia | 39 | 16.8 |
Renal failure | 47 | 20.3 |
Vascular territory of the infarction | number (n) | Percentage(%) |
MCA | 121 | 82.9 |
ACA | 12 | 8.2 |
Anterior choroid artery | 5 | 3.4 |
Junctional | 1 | 0.7 |
PCA | 12 | 8.2 |
Cerebral trunck | 10 | 6.8 |
Cerebellum | 4 | 2,74 |
Internal carotid | 124 | 84.9 |
Internal carotid and vertebrobasilar territory | 6 | 4.1 |
Vertebrobasilar territory | 16 | 11 |
Location of ICH | Number (n) | Percentage(%) |
Deep hemispherical | 55 | 64 |
Lobe hemispherical | 21 | 24.4 |
Brainstem | 2 | 2,32 |
Cerebellar | 6 | 6,98 |
Intraventricular | 2 | 2,32 |
Total | 86 | 100,00 |
Volume of infarction | Number (n) | Percentage(%) |
Large volume | 52 | 35.6 |
Moderate volume | 48 | 32.9 |
Small volume | 46 | 31.5 |
Total | 146 | 100.00 |
Initial volume of ICH (cm3) | Number (n) | Percentage (%) |
< 30> | 30 | 34.9 |
[30-60] | 38 | 44.2 |
> 60 | 18 | 20.9 |
Total | 86 | 100.00 |
Associated neuroradiological signs | Number (n) | Percentage(%) |
Brain edema | 130 | 56 |
Mass effect | 136 | 58.6 |
Brain engagement | 49 | 21.1 |
Ventricular flooding | 39 | 16.8 |
Acute hydrocephalus | 15 | 6.5 |
etiologies of cerebral infarction | Number (n) | Percentage (%) |
Cervicocephalic atherosclerosis | 37 | 25.3 |
Embologenic heart disease | 40 | 27.4 |
Cerebral microangiopathy | 13 | 8.9 |
Dissection of cervicocephalic arteries | 2 | 1.4 |
Associated causes | 12 | 8.2 |
Undetermined causes | 66 | 45.2 |
Etiologies | Number (n) | Percentage(%) |
Hypertensive microangiopathy | 62 | 72.1 |
Undetermined causes | 12 | 13.9 |
Toxic causes | 3 | 3,49 |
Cerebrovascular malformations | 4 | 4.7 |
Anticoagulants/antiplatelet agents | 2 | 2.3 |
Cerebral amyloid angiopathy | 1 | 1.2 |
Tumor causes | 2 | 2.3 |
Total | 86 | 100 |
Table III: Distribution of patients according to laboratory data, cerebral CT scan on admission and etiologies of stroke.
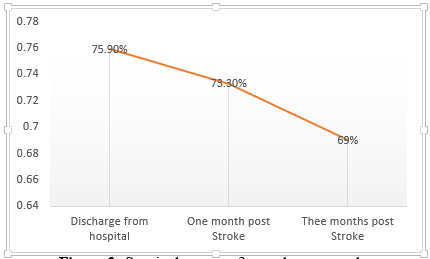
The mean length of hospital stay was 12.6 days ± 8.5 (range 2 to 57 days). At the end of hospitalization, 1 month after stroke and 3 months after stroke, 56 patients (24.1%), 62 patients (26.7%) and 72 patients (31%) respectively died (Figure 2).
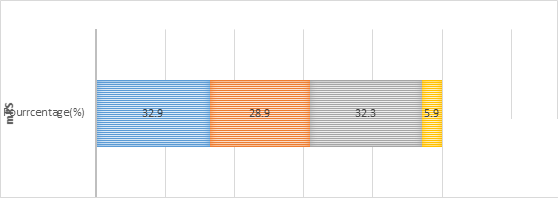
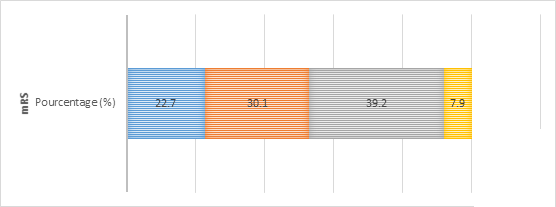
At the end of hospitalization, there were 176 survivors, of whom 136 patients (77.3%) were still dependent. At 1 month post-stroke, there were 170 survivors, of whom 114 patients (67.1%) were still dependent. At 3 months post-stroke, there were 160 survivors, among whom, 69 patients (43.1%) were dependent. The gain in autonomy of patients concerned 17.2% of patients at the end of hospitalization, 24.1% of patients at 1 month after stroke and finally 39.2% of patients at 3 months after stroke; while the functional dependence of patients gradually decreased from 58.6% of patients at the end of hospitalization to 49.1% of patients at one month after stroke and to 29.7% of patients at 3 months after stroke (Figure 3).
Functional motor rehabilitation by physiotherapy was indicated in 136 patients (77.3%) during and after hospitalization in all patients; however, only 110 patients (80.8%) of them benefited from it.
Cumulative mortality rates at the end of hospitalization, at 1 month and 3 months post stroke, increased from 24.1% to 26.7% and 31% respectively.
After a univariate analysis between the socio-demographic, clinical and paraclinical characteristics of patients present on admission to the acute phase of stroke (independent variables) and functional outcome (dependent variable), the variables significantly associated with unfavorable functional outcome at 3 months after stroke were: age ≥60 years (p = 0.001), low level of education (p = 0.004), previous stroke (p = 0.000), rheumatologic comorbidities (p = 0.034), Glasgow score ≤12 (p = 0.000), NIHSS score ≥17 (p = 0.000) cognitive impairment (p = 0.005); anemia (p = 0.012), hyperleukocytosis (p = 0.006), renal failure (p = 0.005); old scarring lesions on neuroimaging (p = 0.023), bilateral localization of the lesions (p = 0.043), HICs of volume> 30 cc (p = 0.013), large infarcts (p = 0.023) and the presence of cerebral edema (p = 0.002).
socio-demographic variables | unfavorable functional outcome Yes No | OR [95% IC] | P | |||
Age | ||||||
< 60> | 22(29.33) | 53(70.6) |
|
| ||
≥ 60 ans | 47(54.65) | 39(45.35) | 2.90 [1.51-5.58] | 0.001 | ||
Sex | ||||||
Femal | 22(36.0) | 39(63.93) | 0.64 [0.33-1.22] | 0.173 | ||
Male | 47(47.00) | 53(53.00) | ||||
Residence | ||||||
Rural | 15(48.39) | 16(51.61) | 1.32 [0,60-2.89] | 0.488 | ||
Urban | 54(41.54) | 76(58.46) |
|
| ||
Schooling |
|
|
|
| ||
Schooled | 38(55.88) | 30(44.12) | 0.39 [0.21-0.75] | 0.004 | ||
Unschooled | 31(33.33) | 62 (66.67) | ||||
Marital status | ||||||
single or widowed | 25(50.00) | 25(50.00) | 1.52 [0.78-2.98] | 0.219 | ||
Married or concubinage | 44(39.64) | 67(60.36) | ||||
Vascular risk factors | ||||||
Yes | 62(43.06) | 82(56.94) | 0.97 [0.34-2.75] | 0.95 | ||
No | 7(43.75) | 9(56.25) | ||||
Hypertension | ||||||
Yes | 53(44.54) | 66(55.46) | 1.25 [0.61-2.59] | 0.53 | ||
No | 16(39.02) | 25(60.98) | ||||
Diabetes | ||||||
Yes | 12(54.55) | 10(45.45) | 1.70 [0.69-4.21] | 0.24 | ||
No | 57(41.30) | 81(58.70) | ||||
Smoking | ||||||
Yes | 7(37.84) | 12(63.16) | 0,74[0.28-2.00] | 0.55 | ||
No | 62(43.97) | 79(56.03) | ||||
Alcohol | ||||||
Yes | 10(34.48) | 19(65.52) | 0.64 [0.28-1.49] | 0.294 | ||
No | 59(45.04) | 72(54.96) | ||||
Obesity | ||||||
Yes | 9(56.25) | 7(43.75) | 1.80 [0.63-5.10] | 0.261 | ||
No | 60(41.67) | 84(58.33) | ||||
Sedentarty | ||||||
Yes | 14(60.87) | 9(39.13) | 2.32 [0.94-5.73] | 0.063 | ||
No | 55(40.15) | 82(59.85) | ||||
Previous stroke | ||||||
Yes | 24(75.00) | 8(25.00) | 5.53 [2.30-13.32] | 0.005 | ||
No | 45(35.16) | 83(64.84) | ||||
Cardiac arrhythmia by atrial fibrillation | ||||||
Yes | 5(41.67) | 7(58.33) | 0,94[0,28-3,09] | 0.912 | ||
No | 64(43.24) | 84(56.76) | ||||
Atherosclerosis | ||||||
Yes | 2(66.67) | 1(33.33) | 2.69 [0.24-30.25] | 0.404 | ||
No | 67(42.68) | 90(57.32) | ||||
|
|
|
|
| ||
Comorbidities | ||||||
Oui | 39(48.15) | 42(51.85) | 1.51 [0.81-2.85] | 0.194 | ||
Non | 0 | 49(62.03) | ||||
Cardiac comorbidities | ||||||
Yes | 18(39.13) | 28(60.87) | 0.79 [0.39-1.59] | 0.517 | ||
No | 51(44.74) | 63(55.26) | ||||
Respiratory comorbidities | ||||||
Yes | 3(75.00) | 1(25.00) | 4.09 [0.42-40.21] | 0.192 | ||
No | 66(42.31) | 90(57.69) | ||||
Renal comorbidities | ||||||
Yes | 1(50.00) | 1(50.00) | 1.32 [0.08-21.54] | 0.843 | ||
No | 68(43.04) | 90(56.96) | ||||
Neurological comorbidities | ||||||
Yes | 9(64.29) | 5(35.71) | 2.58 [0.82-8.08] | 0.094 | ||
No | 60(41.10) | 86(58.90) | ||||
Rheumatological comorbidities | ||||||
Yes | 13(65.00) | 7(35.00) | 2.78 [1.04-7.41] | 0.034 | ||
No | 56(40.00) | 84(60.00) | ||||
Tumor comorbidities |
|
|
|
| ||
Yes | 5(62.50) | 3(37.50) | 2.29 [0.53-9.94] | 0.256 | ||
No | 64(42.11) | 88(57.89) |
|
| ||
mRS preceding stroke |
|
|
|
| ||
mRS = [3-5] | 22(70.97) | 9(29.03) | 4.26 [1.81-10.02] | 0.000 | ||
mRS = [0-2] | 47(36.43) | 82(63.57) |
|
| ||
Stroke | ||||||
Cerebral infarction | 52(47.27) | 58(52.73) | 0.57 [0.29-1.15] | 0.120 | ||
intra-cerebral hemorrhage | 17(34.00) | 33(66.00) | ||||
Ancient cicatricular lesions | ||||||
Yes | 19(61,29) | 12(38,71) | 2,50[1,12-5,59] | 0,023 | ||
No | 50(38,76) | 79(61,24) | ||||
The laterality of the lesion | ||||||
Bilateral | 5(83,33) | 1(16,67) | 7,03[0,80-61,63] | 0,043 | ||
Unilateral | 64(41,56) | 90(58,44) | ||||
Side of the lesion | ||||||
Right | 24(38,10) | 39(61,90) | 0,78[0,41-1,51] | 0,468 | ||
Left | 40(43,96) | 51(56,06) | ||||
Volume of intra cerebral hemorrhage | ||||||
> 30cc | 3(13,64) | 19(85,36) | 0,17[0,04-0,71] | 0,010 | ||
≤30 cc | 13(48,15) | 14(51,85) | ||||
Volume of cerebral infarction | ||||||
Large volume | 23(60,42) | 19(39,59) | 2,37[1,12-5,05] | 0,023 | ||
Small volume | 27(39,13) | 42(60,87) | ||||
Associated neuroradiological lesions | ||||||
Yes | 49(52,69) | 44(47,31) | 2,61[1,35-5,08] | 0,004 | ||
No | 20(29,85) | 47(70,15) | ||||
Brain swelling | ||||||
Yes | 45(54,88) | 37(69,23) | 2,74[1,43-5,23] | 0,002 | ||
No | 24(30,77) | 54(59,34) | ||||
Mass effect | ||||||
Yes | 45(53,57) | 39(46,43) | 2,50[1,30-4,77] | 0,005 | ||
No | 24(31,58) | 52 (68,42) | ||||
Cerebral engagement | ||||||
Yes | 15 (71,43)) | 6(28,57) | 3,93 [1,44-10,76] | 0,005 | ||
No | 54 (38,85) | 85(61,15) | ||||
hemorrhagic rearrangement of cerebral infarction | ||||||
Yes | 7(58,33) | 5(41,67) | 1,94 [0,53-6,40] | 0,269 | ||
No | 62(41,89) | 86(58,11) | ||||
acute hydrocephalus | ||||||
Yes | 2(100) | 0(0,00) | Indéfini | 0,102 | ||
No | 67(42,41) | 91(57,59) | ||||
ventricular flood | ||||||
Yes | 6(33,33) | 12(66,67) | 0,63 [0,22-1,76] | 0,373 | ||
No | 63(44,37) | 79(55,63) | ||||
Table IV : univariate analysis results
After multivariate analysis with logistics regression step by step, the independent predictive factors of the unfavorable functional outcome to 3 months post-stroke identified were: age ≥ 60 years (OR 2.84; 95% IC [1,48- 5,48], p = 0.007), pre-stroke disability (mRS pre-stroke ≥3) (OR 3,51, 95% IC [1,18-7,80] ; p = 0.032), Glasgow score ≤ 12 (OR 3.97; 95% IC [1.91-8.04]; p = 0.005), NiHSS score ≥ 17 (gold 4,18; 95% IC [1,28-13,70] p= 0.018) and large cerebral infarction (OR 3.78, 95% IC [1,93-9,62]; p = 0.004) (Table V).

The 3-month post stroke functional outcome seems better in developed or midddle-income countries, than in low-income countries such as Sub-Saharan Africa countries [8-11]. The thrombolysis and the stroke units widely implemented in developed countries contributed to the reduction of the mortality and frequency and the severity of the post-stroke functional sequelae [12, 13]. In African Sub Saharan, on the other hand, the high lethality, the post stroke high frequency and the severity of functional sequelae, were blamed on limited access to health care, including the near absence of stroke units, late hospital management and insufficient human resources adequately trained to provide acute care and functional rehabilitation to stroke victims [4, 14].
Indeed, in most sub-Saharan African countries, such as ours, we see, (i) a low availability of physical medicine and rehabilitation services equipped, specialized and organized into coordinated multidisciplinary care teams [15, 16]; (ii) insufficiency or even lack of qualified functional rehabilitation professionals, including physicians of physical medicine and rehabilitation, occupational therapists, speech therapists, neuropsychologists, psychomotricians [15]; (iii) a low quality of rehabilitation, due to late access, low compliance and accession and lack of attendance of patients by even ignorance of the interest of population rehabilitation [6 , 15, 16] and the problems of poverty of the populations [4]. Thus, in our study, only 80.8% of patients who had a physiotherapy indication benefited.
The identification of predictors of functional recovery after stroke Acute is important for the development of stroke management strategies, particularly in limited resources [14]. Functional independence of patients is mainly conditioned by their motor capacities. Nevertheless, cognition including language, visual functions, emotional disorders and pain impact this functional independence [17].
In our study, age ≥ 60 years, disability (mRS ≥ 2) preceding, initial clinical gravity of stroke (NIHSS ≥ 17), initial alteration of vigilance (GCS ≤ 12) and initial large-volume cerebral infarctions, all present in the acute phase, were identified as independent predictors of unfavorable motor functional outcome at 3 months post stroke. This result is in agreement with several studies [3, 9].
Strokes in the elderly are characterized by a darker functional and cognitive outcome, due to an often polypathological context and more frequent comorbidities, in particular a physical and / or cognitive handicap pre-existing to the stroke, which exposes these patients to greater risk of suboptimal care, often referred to under the term "ageism" of the Anglo-Saxons [9, 14, 18, 19].
The pre-existing dependence on stroke is often associated with a pejorative functional outcome according to several studies around the world [9, 20, 21].
The initial severity of stroke, often measured by the NIHSS, is a strong predictor of death and functional outcome after stroke according to numerous studies [11, 22]. In addition, among the symptoms or signs of initial severity of stroke, initial impaired alertness, disorientation, limb motor deficit, trunk ataxia, and dysphagia have been reported as early predictors of unfavorable functional outcome [9]. In our study, only impaired alertness (GCS ≤ 12) was identified as predictors of poor functional outcome after stroke among neurological symptoms.
The initial impairment of alertness, the initial clinical severity of the stroke, and the initial large size of the strokes, are a direct reflection of the severity and extent of the neurological damage due to the stroke, which explains their influence on the possibilities of functional recovery after stroke [23].
The neurobiological basis of post-stroke functional recovery is represented by post-injury neuronal plasticity. It consists of a reorganization of neuronal interactions in order to preserve and / or restore as much as possible the functional capacities of the nervous system [24]. It is specifically dependent on the age, the extent of the lesions and the degree of development of the cerebral structure involved, as well as the functional stimuli that it can receive, taking into account the notion of the critical period during which the stimuli remain operational. This critical period extends up to 3 months after the stroke [25, 26].
It is admitted that advanced age and the extent of cerebral lesions decrease the repair capabilities of neuronal circuits, while the absence or insufficiency of post-lesion functional rehabilitation does not allow the activation of substitution processes. and/or functional compensation, essential for optimal post-injury functional recovery [27, 28].
Early management of all stroke patients in stroke units, including the elderly, the use of specific therapies aimed at reducing the extent of brain damage and the clinical severity of stroke, such as fibrinolysis of infarction and early reduction of hypertension during intracerebral hemorrhages, from the acute phase, associated with quality functional rehabilitation started early, constitute an effective means of reducing the frequency and severity of functional sequelae after stroke.
Limits of our study
In our study, we evaluated the functional outcome of patients according to the mRS which is a global assessment score of functional disability, including motor skills, language, cognitive disability, in a living context. But in our study, our patients have only benefited from functional motor rehabilitation by physiotherapy, some rare patients have benefited from speech therapy. None of our patients benefited from occupational therapy or cognitive revalidation. Motor rehabilitation has been carried out in most cases, in physiotherapy practices; No patients were supported in a physical medicine and rehabilitation service with adequate equipment with a good multidisciplinary team organization.
The data concerning aphasia and intellectual deficits were not specifically taken into account, due to the absence of cognitive rehabilitation and the very low availability of language rehabilitation, in our context.
Despite these shortcomings, our results are comparable to those of the literature.
Functional outcome at 3 months after stroke remains unfavorable in Burkina Faso, marked by a high frequency of often severe functional sequelae. Advanced age, initial impairment of alertness, disability pre-existing to the stroke, initial clinical severity of the stroke, the large size of the cerebral infarction from the initial CT scan, are the predictive factors of unfavorable functional outcome at 3 months post stroke. The early admission of all patients to stroke units, including the elderly, the use of specific therapies aimed at reducing or stabilizing the volume of stroke, from the acute phase, associated with quality functional rehabilitation, will effectively contribute to reducing the frequency and severity of post-stroke functional sequelae and to better socio-professional reintegration of patients suffering from stroke.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
