
Research | DOI: https://doi.org/10.31579/2642-973X/024
1 Internal Medicine II and Stroke Unit, San Giuseppe Hospital, Empoli, Italy.
2 Neurology, San Giuseppe Hospital, Empoli, Italy.
3 Emergency Department, San Giuseppe Hospital, Empoli, Italy.
4 Radiology, San Giuseppe Hospital, Empoli, Italy.
*Corresponding Author: Luca Masotti, MD, Head, Internal Medicine II and Stroke Unit, San Giuseppe Hospital, Viale Boccaccio 20, 50053, Empoli, Florence, Italy.
Citation: Stefania D Martino, Sisti E, Cozzi A, Francolini V and Masotti L. (2022). Predictive Power of Hemorrhagic Transformation Scores in Real Life Stroke Patients Undergone to Urgent Reperfusion: A Brief Report. Brain and Neurological Disorders. 5(3); DOI:10.31579/2642-973X/024
Copyright: © 2022, Luca Masotti, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 March 2022 | Accepted: 17 June 2022 | Published: 25 June 2022
Keywords: stroke; thrombolysis; mechanical thrombectomy; hemorrhagic transformation; outcome
Introduction and aim: Hemorrhagic transformation (HT) is the most feared complication in acute phase of ischemic stroke. Predicting HT is of utmost importance in clinical practice. In the latest years a lot of HT prediction scores have been proposed, but their comparison in real life lack. Therefore, the aim of our study was to provide information about this topic. Materials and Methods: We retrospectively calculated THRIVE, SPAN-100, MSS score, SITS-ICH and GRASPS scores in patients consecutively admitted in our Stroke Unit along two years. To evaluate their predictive power, the area under the curve (AUC) of the Receiver Operating Characteristic (ROC) curve was calculated. Results: Study population was composed by ninety-one patients (51.6% females) with mean age 80.1 ± 11.3 years. Seventy-four (81.3%) patients undergone to systemic intravenous alteplase, seven (7.7%) to mechanical thrombectomy, ten (11%) to systemic intravenous alteplase plus mechanical thrombectomy. Eighteen patients (19.7%) presented HT. MSS score was the best prognosticator of HT, however the predictive power of the five analyzed score was low, ranging from and none of the score resulted significantly superior to the others. Conclusion: Our real-life study showed a low predictive power of a lot of HT prediction scores. Further prospective studies are warranted.
Predicting hemorrhagic transformation (HT) in stroke patients undergone to urgent reperfusion by intravenous thrombolysis and/or mechanical thrombectomy is of utmost importance in clinical practice. In 2017, a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association identified seven validated scores for predicting HT in clinical practice [1-8]. All these seem to have a similar predictive power, C statistic ranging from about 0.50 to 0.86. National Institute of Health Stroke Scale (NIHSS) score is the only one variable present in all seven scores, while age is present in six of seven scores. Other variables present in the majority of scores are high glucose levels and blood hypertension [1]. Literature lacks about comparison between these prediction score in real life patients, therefore the aim of our study was to compare the power of HT prediction scores.
We retrospectively analyzed clinical, instrumental and laboratory data of patients with acute ischemic stroke consecutively admitted to our Stroke Unit along two years, from November 1st 2017 to November 1st 2019, and undergone to sistemi thrombolysis and/or mechanical thrombectomy. For all patients we calculated five of the seven HT prediction scores proposed by ASA/AHA: THRIVE score [7], SPAN-100 score [8], MSS score [2], SITS-ICH score [5] and GRASPS score [6] (see Table 1 for characteristics of each score). To evaluate their predictive power, the area under the curve (AUC) of the Receiver Operating Characteristic (ROC) curve was calculated. All analyses were performed using MEDCALC statistical software (MedCalc Software Ltd, Acacialaan 22, B-8400 Ostend, Belgium).
Study population was composed by ninety-one patients (51.6?males) with mean age 80.1 ± 11.3 years. Median NIHSS at hospital arrival was 3 (IQR 1-5). Twelve patients (13.2%) had NIHSS score ≥ 8 points. Seventy-four (81.3%) patients undergone to systemic intravenous alteplase, seven (7.7%) to mechanical thrombectomy, ten (11%) to systemic intravenous alteplase plus mechanical thrombectomy. At 24- hour brain CT-scan, eighteen patients (19.7%) presented HT, ten of them (55.5%) symptomatic according to the statement criteria (increase in NIHSS score of ≥4 points) (1). Median NIHSS score after 24 hours from urgent reperfusion was 9.5 (IQR 5-13.5) in patients with HT and 3 in patients without HT (IQR 2-8) (p less than 0.001). In-hospital mortality was 27.7% in patients with HT versus 2.7% in patients without HT (p less than0.001). Median 90-day modified Rankin scale was 4 (IQR 3-4) in patients with HT versus 2 (IQR (0.5-3) in patients without HT (p less than 0.001). MSS score was the best prognosticator of HT (Figure 1), however the predictive power of the five analyzed score was low (Table 2) both for overall HT than for symptomatic HT and none of them resulted significantly superior to the others at pairwise comparison (Table 3).
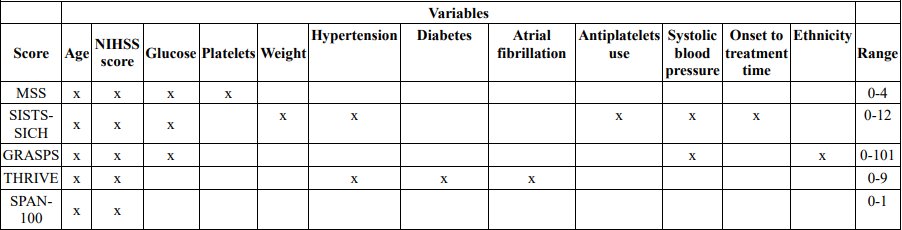
Table 1: Characteristics of analyzed HT prediction scores
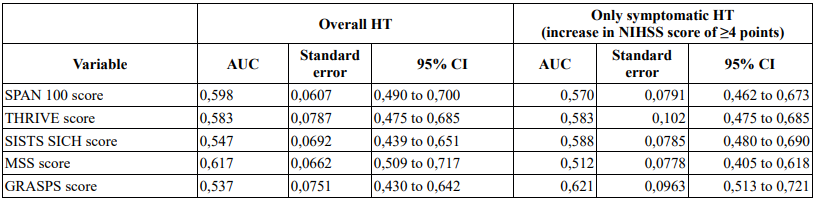
Table 2: Predictive power of analyzed HT scores
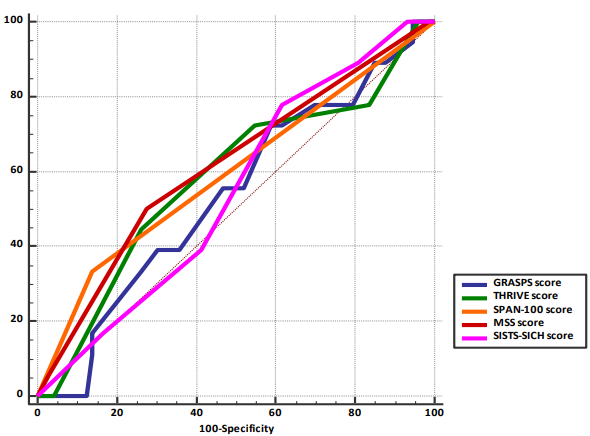
Figure 1: Comparison of areas under the receiver operating curves of HT scores
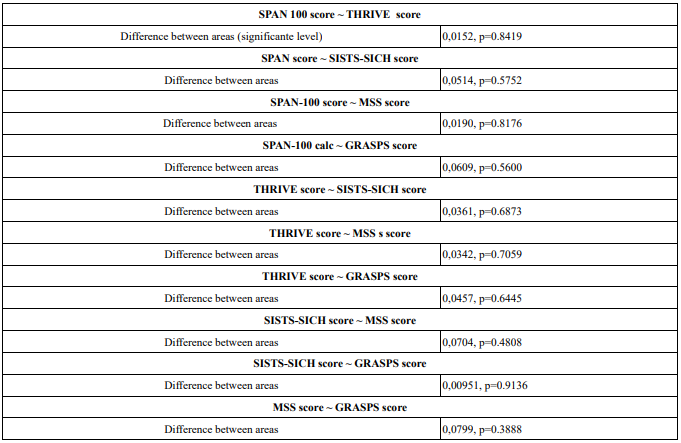
Table 3: Pairwise comparison of score ROC curves
HT represents the most feared complication of urgent reperfusion in acute stroke patients and it is associated to reduced neurological improvement or deterioration [9]. Therefore, predict or prevent HT is fundamental. Despite the prediction scores are effective at estimating the HT risk, in clinical practice it's not justified withholding urgent reperfusion treatment in patients with high HT scoring. Many HT predictions scores have been proposed [2-8] in the past decade and others have been recently proposed [10-12]. These could help to select high HT risk patients requiring a closer monitoring. Despite limitations due to retrospective methodology, single center and limited sample size, our real-life study showed a low predictive power of a lot of HT prediction scores. Further prospective studies are warranted.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
