North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, United Kingdom.
*Corresponding Author:
Anthony Kodzo-Grey Venyo, North Manchester General Hospital, Department of Urology, Delaunays Road, Manchester, United Kingdom.
Citation: Grey Venyo AK, (2024), Prediction of Binding Affinity for some Tetrahydro carbazole Derivatives as Serotonin Receptor Antagonists from their Molecular Structural Descriptors, J. General Medicine and Clinical Practice, 7(3); DOI:10.31579/2639-4162/124
Penile intraepithelial neoplasia (PeIN) is a histopathology terminology that is utilized for precancerous penile lesions. PeIN is important in view of the high morbidity and mortality associated with progression to penile squamous cell carcinoma (PSSC). But PeIN is not commonly encountered and it does contribute to a limited evidence-base for the relative efficacy of available options of treatment. PeIN tends to be classified into HPV-associated and HPV-independent (differentiated) (dPeIN). Even though HPV-associated PeIN had been linked to the oncogenic effect of human papillomavirus (HPV), the HPV-independent pathway is stated to be driven by chronic inflammatory conditions. These two biology pathways had been iterated to be are associated with distinct histopathology examination features. The commonest morphology patterns of HPV-associated PeIN include basaloid, warty, and mixed PeIN. DPeIN is the morphological expression of HPV-independent PeIN. A review of therapy options and outcomes for PeIN, had summated the ensuing findings: Topical agents had demonstrated response and recurrence rates of 40% to 100% and 20% for imiquimod, and 48-74% and 11% for 5-fluorouracil, respectively. Discontinuation of topical agents in view of side effects had been noted in 12% of cases. Response rates for laser treatment options were 52 % 100%, with recurrence in 7 % 48% of cases and a change in penile sensitivity in 50%. Circumcision was documented to have cleared preputial PeIN. Recurrence rates pursuant to surgical treatment of glans PeIN were documented to be 25% for wide local excision, 4% for Mohs surgery, 5% for total glans resurfacing, and 10% for glansectomy. Limited data does exist related to the factors that would predict treatment response and to sequencing of treatment options. Many treatment options are available for men who have precancerous lesions of the foreskin or glans penis. Close follow-up is necessary inn view of the fact that PeIN lesions could or progress to invasive penile cancer, a close regular, follow-up assessments are required to establish early any recurrent PeIN lesion or the lesions that had become invasive or malignant. Considering the rarity of PeIN, and the fact that there is no global consensus opinion of the best treatment options of PeINs in various parts of the world it is important for all clinicians to be aware of the clinical manifestations, diagnosis, treatment options that may be available in every locality of the world including the developing countries taking into consideration the availability and non-availability of laser and other treatment agents. It is therefore important for readers to read carefully, summations related to PeINs of the penis in order to establish a quick diagnosis of the PeIN lesion so as to provide a suitable treatment for patients taking into consideration the local availability of treatment options.
Introduction
Intraepithelial neoplasm an in situ epithelial squamous cell carcinoma of the skin that generally does not infiltrate the dermis or surrounding tissues has been iterated to have been first reported by Bowen. [1] [2] It had also been iterated that intraepithelial neoplasm most commonly manifests within the proximal skin of the trunk or limbs and it could also be found within the oral mucosa, conjunctival membrane, and nail bed [1] [3]. It has furthermore been stated that the aetiology may be related to chemical factors including arsenic agents and human papillomavirus [1] [4] Considering that intra-epithelial carcinoma of the penis is rare, it would be envisaged that a number of clinicians may not be familiar with the manifestations, diagnostic features, management, as well as outcome of the lesion. The ensuing article on intraepithelial carcinoma of the penis is divided into two parts: (A) Overview and (B) Miscellaneous Narrations and Discussions from some Case Reports, Case Series and Studies Related to Intraepithelial carcinoma of penis.
Aims
To review and update the literature on Penile Intraepithelial neoplasia (PeIN)
Method
Internet data bases were searched including: Google; Google Scholar; Yahoo; and PUBMED. The search words that were used included: Penile Intraepithelial neoplasia; PeIN; Intra-epithelial neoplasm of penis; Intraepithelial neoplasm of glans penis; Intraepithelial tumour of foreskin; Intraepithelial tumour of penis. Fifty (50) references were identified which were used to write the article which has been divided into two parts: (A) Overview which has discussed various general aspects of Penile Intraepithelial neoplasms (PeINs) and (B) Miscellaneous Narrations and Discussions from some Case Reports, Case Series and Studies Related to Intraepithelial carcinoma of penis.
Results
[A] Overview
Definition / general statements [5]
Intraepithelial neoplastic proliferation with variable degree of dysplasia, keratinization and nuclear atypia
Penile intraepithelial neoplasia (PeIN) is classified as HPV related / dependent or HPV unrelated / independent, similar to invasive carcinomas [6] [7]
PeIN is regarded as a precursor of penile invasive carcinoma
Essential features [5]
PeIN is classified as HPV related / dependent or HPV unrelated / independent
PeIN may occur in any areas of the penis including: penile mucosal epithelial areas, most commonly in the glans penis and foreskin
Differentiated PeIN has tended to be related to lichen sclerosis
HPV16 is the most frequent genotype which tends to be associated with Pekin
Terminology [5]
Documented synonyms for Pekin include: erythroblastic of Quadrat, Bowen disease, carcinoma in situ (CIS), squamous intraepithelial lesion, dysplasia (mild, moderate and severe) and Bowenoid papulosis
It had been pointed out that Pekin is the recommended nomenclature or terminology to be used for penile precancerous lesions [8]
It has been stated that Pekin does refer to squamous lesions and does exclude Paget disease, urothelial carcinoma in situ and malignant melanoma in situ
It has been iterated that some authors do stratify Pekin into grades I, II and III [5] [9]
Epidemiology [5]
It has been iterated that there is geographic variation in the manifestation of Pekin [10]
It has been iterated that Differentiated Pekin has tended to be more commonly diagnosed within countries that have a high frequency of penile cancer. [5]
HPV related Pekin is more common in countries with a low frequency of penile cancer
It has been stated that within countries that have a high frequency of invasive penile carcinomas (2 - 5 cases/100,000), pen is rarely diagnosed as a solitary lesion [5] [10]
It has been iterated that within countries in which invasive penile carcinomas are rare (≤ 1 case/100,000), pen is the commonest penile neoplasia at clinical diagnosis. [5]
It has been documented that pen does tend to affect patients who are younger than those with invasive cancers [5] [11]
It has been iterated that the mean age of PeIN is about 58 years of age. [5]
It has been documented that HPV related PeIN preferentially does tend to afflict younger patients. [5]
It has been iterated that predisposing factors for PeIN include: HIV / immunosuppression, lack of or delayed circumcision, inflammatory / irritative conditions (balanitis, buried penis, phimosis) [5] [12]
Sites
It has been iterated that PeIN is most commonly found in the glans penis and foreskin [9] [13]
It has been documented that Differentiated PeIN, non-HPV related, preferentially does tend to involve the foreskin inner mucosal epithelium
It has been iterated that about 33% of cases with PeIN are multicentric, especially the HPV related types. [5]
It had also been pointed out that pen may occur in the skin of the shaft of the penis
Aetiology
It has been iterated that Undifferentiated pen is associated with: high risk HPV. [5]
It had also been stated that Differentiated pen is linked with: lichen sclerosis. [5]
Clinical Manifesting Features
Lesions can be subclassified according to morphology features and HPV genotypes present [14]
Non-HPV related pen / differentiated
Represented by differentiated pen
Squamous or simplex pen are synonyms
Putative precursors of non-HPV related keratinizing squamous cell invasive carcinomas, the majority of penile cancers
Most cases in association with invasive carcinoma and rarely as a solitary lesion
Difficult to diagnose and underrecognized by pathologists due to only subtle histologic changes
Foreskin is a preferential site but the glans is also involved
Frequently associated with lichen sclerosis
HPV related pen / undifferentiated
Subclassified in basaloid, warty and warty basaloid subtypes [15]
Bowen disease, CIS, high grade pen are synonyms
In young males with multicentric lesions, it has been referred to as Bowenoid papulosis [16]
More frequently multicentric than differentiated pen
Putative precursors of HPV related basaloid and condyloma Tous (warty) invasive carcinomas or mixtures, about 33% of penile cancers [14]
Straightforward diagnosis and well recognized by pathologists
Glans is a preferential site but the foreskin, coronal sulcus and shaft may also be involved
HPV16, 6 and 11 are the most commonly found genotypes [17] [18]
HIV positive patients are more susceptible to develop HPV related pen [19]
mixed pein
Coexisting non-HPV and HPV related pen in the same specimen
Rarely found as solitary lesions
Multicentric lesions may be in collision, next to each other or in separate foci
Pathological features and HPV composition are similar in pen and invasive carcinomas [18]
HPV is usually negative in differentiated pen and the corresponding invasive non-HPV related squamous cell carcinoma
HPV is usually positive in pen and the corresponding invasive basaloid or warty invasive carcinoma
Morphological similarity and HPV genotype composition indicate a causal relation of pen and corresponding invasive carcinoma
Diagnosis [5]
Diagnosis of intraepithelial neoplasia could be established based upon the ensuing: [5]
Meatoscopic
Pathology examination of Biopsy of the lesion.
Excision - Pathology examination of the excised lesion.
Prognostic factors
The prognostic factors of pen had been summated to include the ensuing: [5]
The development of frequent recurrence which has been iterated to constitute 48% of cases [20]
pen has been stated to be associated with low rate of progression to invasive carcinoma of 2%. [5] [20]
Treatment
The treatment of pen has been summated to include the ensuing: [5]
Local excision of the lesion (Mohs surgery, glans resurfacing, lensectomy, which had tended to be the most frequent approach, [21] [22]
Laser treatment which has been stated to be associated with higher complication and recurrence rate [23]
Utilization of topical agents including: 5-fluorouracil, and imiquimod in 5% of cases.
Undertaking of local destructive methods including: photodynamic therapy, cryotherapy, curettage and electrocautery. [5]
Gross description
The macroscopy examination features of pen had been summated to include the ensuing: [5]
Non-HPV related pen / differentiated
Solitary white or pink macule, plaque or slightly elevated geographical lesion
Affects the foreskin and glans and rarely the shaft
HPV related pen
Lesions are flat or slightly elevated or popular, velvety, erythematous, dark brown or black
Warty Pens are granular or villous
Borders are irregular or sharply delineated [15]
Microscopic (histologic) description
The microscopy examination features of pen had been summated to include the ensuing: [5]
Non-HPV related pen / differentiated
Common features are hyperkeratosis, parakeratosis, hyper granulosis, acanthosis, elongation of rete ridges, abnormal squamous maturation and squamous cell atypia
Prominent intercellular oedematous bridges and intraepithelial keratinization
Some histological heterogeneity: hyperplasia-like, classic and pleomorphic features
Most common or classic feature is a keratinized maturing lesion with obvious atypical cells involving 2 or 3 basal epithelial layers
Less common are the hyperplasia-like features, with acanthotic thickening of the epithelium and subtle basal cell atypia
In the pleomorphic variant, there are anaplastic cells involving most of the epithelial thickness but with evident maturation or cellular keratinization
Grading system if used can classify as follows: hyperplasia-like as grade 1, classic as grade 2, pleomorphic as grade 3
Basaloid pen
Most frequent subtype
Uni or multicentric
Usually, flat lesions with a broad or undulating base
Monotonous uniform small anaplastic basaloid cell population
Replace the full epithelial thickness
Superficial hyper and parakeratosis often with some koilocytes is typical
Rarely, cells are larger, spindly or pleomorphic
High nuclear cytoplasmic ratio
Numerous mitoses may be noted
Starry sky pattern is not uncommon
Warty pen
Presentation as a solitary lesion is unusual [14]
Most commonly, it is part of a multicentric lesion
Associated with invasive warty or basaloid carcinomas
Squamous maturing lesion
Striking micropapillary spiking features
Surface shows hyper and parakeratosis
Hallmark is atypical superficial or deep pleomorphic koilocytosis
Multinucleation, nuclei with irregular contours, perinuclear halo and dyskeratosis are common
Warty basaloid pen [5]
Warty cells and basaloid cells in about equal proportions
Unifocal or multicentric lesions
May be associated with invasive basaloid or warty carcinomas
Hyper and parakeratosis, papillary or spiking features at the upper half
Upper half is composed of clear warty-like cells
Lower half is composed of small, anaplastic basaloid type cells
Immunohistochemistry staining features of pen (positive and negative)
Positive stains [5]
The positive immunohistochemistry of pen had been summated as follows: [5]
Non-HPV related pen / differentiated
Ki67: positive above the basal cell layer
P53: may be positive in an irregular patchy pattern
HPV related pen / undifferentiated
Ki67: positive in most cells, full thickness
P16: 99% positive, en bloc for basaloid pen and ≤ 50% of epithelial thickness in warty basaloid and warty pen, [20] [24]
Negative stains [5]
The negative immunohistochemistry of pen had been summated as follows: [5]
Non-HPV related pen / differentiated
P16: [24]
Molecular / cytogenetics description [5]
The molecular / cytogenetics features of pen had been summated as follows: [5]
HPV detection by PCR or ISH is negative in differentiated pen
High risk HPV is detected in most HPV related pen
HPV16 found in 67% of basaloid pen [14]
Low risk HPV is present in 16% of warty pen [14]
More variable HPV genotypic composition in warty pen
Differential diagnosis [5]
The differential diagnoses of pen had been summated as follows: [5]
Non-HPV related / differentiated pen:
Squamous hyperplasia:
Atypia is not present
p53 positive cells are restricted to the basal cell layer
Ki67 positive scattered in basal cell layer
Condyloma acuminatum, flat type:
Koilocytes usually seen
HPV low risk positive
P16 is also negative so is not helpful
HPV related pen (versus pleomorphic differentiated pen):
No squamous maturation
Koilocytosis
HPV and p16 positive
HPV related pen: [5]
Urothelial carcinoma in situ (versus basaloid pen):
p16 negative
Condyloma acuminatum with atypical features (versus warty pen) [18]
p16 negative
May harbour low or high-risk HPV
Squamous cell carcinoma warty and basaloid types (versus warty and basaloid pen)
[b] miscellaneous narrations and discussions from some case reports, case studies related to intraepithelial neoplasms of penis
Huang et al. [1] reported a 44-year-old Asian male patient who had gradually developed a ventral mass upon his penis 7 years preceding his manifestation. At first, the lesion measured about 1 cm in diameter and was occasionally accompanied by paraesthesia’s and bleeding after friction. He had normal micturition and he did not attend the hospital at first. When he developed an ulcer, he applied erythromycin ointment. Sometimes, his focal penile ulceration healed, but the condition often recurred. The scope of the lesion gradually increased over the preceding period of 7 years. Finally, he presented to the dermatology department of the hospital of the authors, where he underwent penile lesion tissue biopsy. The pathology report of the biopsy specimen revealed that he had penile intraepithelial neoplasia. Taking into consideration the large range of lesions, he came to the urological ward for admission and surgical treatment. The patient did not have any clear history of exposure to chemical properties such as arsenic. The result of his HIV antibody test was negative. He did not have a history of smoking or drinking of alcohol. The lesion was found on the ventral side of his penis and the total area of the lesion was about 2 cm ×2.0 cm (see figure 1A). The surface of the penile lesion was pale red with a grey edge. The penile lesion had an irregular shape and clear boundaries, and the lesion slightly protruded out of the surface of the skin. There was no obvious exudate from the ulceration, and there was no obvious redness or swelling of the encompassing skin.
Figure 1: Intraepithelial neoplasia lesion located on the ventral side of the penis (A). Complete resection of the lesion tissue on the surface of the penile deep fascia (B). The penile surgical area was covered with a pedicled scrotal flap (C). The shape of the penis after lesion resection and plastic surgery (D). The surgical area of the penis of the patient is not completely healed half a month after the operation (E). Penile morphology after complete wound healing (F). Reproduced from [1] Under the Creative Commons Attribution License, which allows reproduction of figures and contents of the Journal article provided the original source is cited and credited.
Pursuant to contiguous epidural anaesthesia, a skin incision line was marked at a 1.0 cm margin from the edge penile lesion of the patient. The scrotal flap range that was needed for the lesion to be isolated was set preceding the resection of the lesion. The skin of the lesion was cut vertically along the designed incision margin line, deep to the deep fascia layer, and completely resected the lesion upon the surface of the deep fascia (see figure 1B). Pursuant to achievement of careful haemostasis by bipolar coagulation, a 5.0 cm ×3.0 cm scrotal flap based upon the resected wound area was made and it was dissociated upon the surface of the deep fascia. With a formed pedicled scrotal flap, it was stretched to the ventral side of the penis and the surgical area of the penile skin was covered (see figure 1 C). Intermittent suturing of the subcutaneous tissue had reduced cavity formation and accumulation of local exudate (see figure 1D). The wound area was dressed in gauze under pressure, and the penis was wrapped up with a self-adhesive bandage under appropriate tension to promote wound healing. No drainage tube was inserted into the operational area. The bandage and gauze were removed to expose the wound and keep it dry 3 days pursuant to the operation. Pursuant to excision of the penile lesion excision, the wound was covered by scrotal flaps with blood supply. There was postoperative oedema within the penile wound without infection. During his follow-up assessment two weeks pursuant to the operation, the wound edge had not healed completely because of tension (see figure 1E). By means of care with wound dressing changes, the wound area finally healed (see figure 1 F). The pathology images (see figures 2 A and 2 B) demonstrated that the lesion tissue was covered with squamous epithelium and had demonstrated finger-like protrusion. The basal part of the lesion revealed bulbous advancing growth. The epithelium within the lesion area had severe dysplasia, disordered arrangement of polarity, large nucleus, deep staining, and complete basement membrane. No definite infiltration of basal layer tissue was identified. The lesion area revealed infiltration of polymorphonuclear giant cells and lymphocytes. The pathology diagnosis was penile intraepithelial neoplasia with granulomatous inflammation. No diseased tissue was identified at the margin of incision. During his 6 months of follow-up assessment, the patient did not have any recurrence of penile intraepithelial neoplasia and he did not have any obvious discomfort upon penile erection.
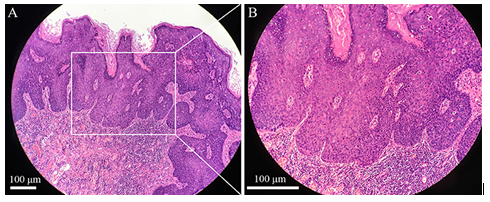
Figure 2: Pathological image of the penile intraepithelial neoplasia lesion with H&E staining, original amplification ×100, scale bar 100 μm (A). Pathological image of the penile intraepithelial neoplasia lesion with H&E staining, original amplification ×200, scale bar 100 μm (B). Reproduced from: [1] Under the Creative Commons Attribution License, which allows reproduction of figures and contents of the Journal article provided the original source is cited and credited.
Huang et al. [1] made the ensuing educative discussions:
The incidence of intraepithelial neoplasia is very low, and the incidence is also rare in Asian male penises.
Intraepithelial neoplasm usually occurs in people aged between 60 years and 70 years.
The lesions mostly tend to be located within the head, neck, hands, trunk, buttocks, oral cavity, as well as within the nail bed.
The lesion is very rarely found within the penis.
The lesions are typified by one or several raised plaques with clear borders, squamous epithelioid changes, and uneven surfaces.
At times, the lesion had easily been misdiagnosed as eczema or psoriasis.
Diagnosis of the lesion is usually established by pathology examination skin biopsy of the lesion.
At the time of publication of the article the cause of the disease had not been clarified.
It had been assumed that intra-epithelial neoplasm had generally been related to the following pathogenic factors [25] arsenic poisoning, excessive ultraviolet exposure, and human papillomavirus infection. Sometimes, the lesions occurring in the penile skin need to be differentiated from invasive squamous cell carcinoma of the penis.
In majority of cases, even small invasive tumours do require surgical therapy as well as expanded resection of the scope and depth of the lesions. This does tend necessitate a sufficient depth for definitive diagnosis of the lesion when excising the lesion tissue for biopsy and pathology examination.
Generally, it has been considered that intraepithelial neoplasia lesions could be surgically resected 5 mm encompassing the lesion [25].
Sufficient depth of tissue should be excised in order to prevent lesions in the case of invasive tumours.
Taking into consideration the integrity of lesion excision and the extensibility of scrotal flaps with regard to their patient, they had designed an incision 1 cm away from the edge of the lesion in their patient who had penile intraepithelial neoplasia.
They resected the underlying tissue and sarcolemma of the lesion.
The final results had demonstrated, that even though the resection range was large, it was covered by scrotal flaps, and the surgical wound had achieved good healing.
The scrotal skin had great extensibility and little restriction on the extension when the penis was erect. It reduced the effect on penile appearance and function to the greatest extent pursuant to plastic surgery repair of the operational wound.
Their method of operation was an ideal surgical method for repairing the skin defect of penile wounds.
Because these lesions tend to be localized within the epidermis and rarely do invade the deep part, smaller intraepithelial neoplasia lesions often tend to be treated by means of radiotherapy, cryotherapy [26], laser treatment, photodynamic treatment [27], or 5-fluorouracil ointment [28].
Nevertheless, the recurrence rate is higher pursuant to these treatments.
For their reported patient, they thought that the choice of surgical treatment was more reasonable in view of the large penile lesion area.
A larger extent and depth of surgical resection could be helpful in ensuring the integrity of lesion resection and in preventing the development of recurrence of penile intraepithelial neoplasia.
Some studies had indicated that [29] the extent of surgical resection does depend upon the size of the tumour and the depth of invasion.
Generally, the lesions not only rarely do involve the subcutaneous and alveolar membrane but they also tend not to be accompanied by lymph node metastasis within the inguinal region.
In order to undertake surgical resection of these lesions, local pressure bandage or indwelling negative pressure drainage tube tends to be utilized to reduce the accumulation of wound exudate.
Taking into consideration the large range of lesions in their reported patient, it was easy to form local exudate accumulation and might lead to surgical wound infection.
They utilized intermittent sutures of subcutaneous tissue in order to reduce the formation of the cavity and local exudate accumulation accompanied with a local appropriate pressure bandage.
There was no drainage tube inserted into the wound area.
Pursuant to the operation, the blood supply of the flap was noted to be good and there was oedema upon the penile wound without infection. About 6 months pursuant to the operation, the wound had healed well.
Ensuing 6 months of follow-up assessments, the Asian man had not developed recurrence of his penile skin lesions. His penile erectile function was not significantly affected.
The treatment of their reported patient with penile intraepithelial neoplasia had shown that it can promote healing of the surgical wound by surgical excision of the lesion and plastic surgery by utilizing a scrotal skin flap. It also provided useful surgical treatment planning for the surgical repair of penile skin defects, wound exposure, and other diseases in the case of trauma or surgery.
During the treatment of their reported patient, they had also found that there were some deficiencies in the treatment effect. Even though the scrotal flap was noted to be helpful for the healing of the surgical wound, it also caused hair attachment on the skin surface of the penis, which might arouse certain inconvenience during the coital life of the patient.
In view of the small number of such cases, their case report had only shared the treatment process and surgical experience of the patient.
As for the treatment of penile intraepithelial neoplasia in the future, there is the need to accumulate more cases in order to help explore as well as establish standard diagnoses and treatment procedures which may contribute to achieving better treatment effects for patients. Issa et al. [23] stated that penile intraepithelial neoplasia (PeIN) is an uncommon skin condition which is associated with the potential to progress to invasive cancer of the penis. Issa et al. [23] undertook a systematic review of treatment options and outcomes for pen and they summarized their findings as follows:
Topical agents had shown response and recurrence rates of 40% to 100% and 20% for imiquimod, and 48% to 74% and 11% for 5-fluorouracil, respectively.
Discontinuation of topical agents because of side effects had been observed in 12% of cases.
Response rates for laser treatments were 52% to 100%, with recurrence in 7% to 48% of cases and a change in penile sensitivity in 50%.
Circumcision had cleared preputial pen.
Rates of recurrence ensuing surgical treatment of glans pen were 25% for wide local excision, 4% for Mohs surgery, 5% for total glans resurfacing, and 10% for lensectomy.
They had found that there was limited data on factors predictive of treatment response and on sequencing of treatment options.
They had found out in their patient summary that many treatment options are available for men who have pre-cancerous lesions of the foreskin or glans.
They would recommend that close follow-up is necessary in view of the fact that the penile lesions could recur or progress to invasive penile cancer.
Cañete-Portillo et al. [30] stated the following:
Lichen sclerosis (LLCs) with penile cancer tends to be found in about two thirds of specimens.
It had been postulated that LLCs does represent a precancerous condition.
In order to qualify as such, in addition to cytological atypia and similarity with the invasive tumour, a spatial correlation between LLCs and neoplastic lesions does need to be demonstrated.
Cañete-Portillo et al. [30] undertook a study which was aimed to evaluate such a spatial relationship. Specimens were evaluated from circumcision that was undertaken in 28 cases, and penectomy that was undertaken in 81 cases. Cañete-Portillo et al. [30] reported that all cases had LLCs, penile intraepithelial neoplasia (pen), and/or invasive squamous cell carcinomas. Cañete-Portillo et al. [30] examined LLCs in relation to invasive carcinoma, pen, and normal epithelia. Invasive squamous cell carcinomas, classified according to the World Health Organization criteria as non-human papillomavirus (HPV)-related and HPV-related Cañete-Portillo et al. [30] reported their findings as follows:
pen, were found present in 100 cases.
Non-HPV-related (differentiated) PeIN was found to be commonest subtype associated with LSc (89%).
There were 5 spatial patterns identified which included:
LSc adjacent to PeIN in 23% of cases,
(2) LSc adjacent and comprising PeIN that was found in 42% of cases,
(3) LSc next to and within invasive carcinomas that was found in 8% of cases,
(4) LSc throughout the sequence PeIN-invasive carcinoma that was found in 24%) of cases, and
(5) LSc was separate (with normal tissue between the lesions) from PeIN and/or invasive carcinomas in a minority of cases that amounted to 3% of the cases.
Cañete-Portillo et al. [30] stated the ensuing:
LSc within the cancer had not been previously described.
In their case series, they had found 35 cases with LSc within invasive carcinomas.
The striking continuous spatial relationship among LSc, PeIN, and/or invasive carcinoma as shown in theirstudy may be a necessary (but not sufficient) condition for the hypothesis postulating LSc as a penile precancerous lesion.
Oertell et al. [13] stated that about 10% to 20% of all penile squamous cell carcinomas (SCCs) do originate within the foreskin, however, knowledge regarding preputial precursor and associated lesions is scant. Overtell et al. [13] undertook a study which was aimed to ascertain the prevalence of various precancerous and cancerous lesions exclusively affecting the foreskin, and to describe their pathological features. With regard the methods and results of their study, Overtell et al. [13] summated the ensuing:
One hundred consecutive circumcision specimens from symptomatic patients who were dwelling within a region of high penile cancer incidence were analysed.
Clinical diagnoses had included mainly phimosis and chronic balanoposthitis that were found in 40 cases and 35 cases, respectively, however, also a tumour mass was found in 11 cases.
Histopathology lesions which had been found included: squamous hyperplasia in 61 cases; lichen sclerosis in 53 cases; penile intraepithelial neoplasia (pen) in 30 cases (all differentiated PeIN, with two cases showing multicentric foci of basaloid and warty-basaloid pen); and invasive SCC in 11 cases (three usual, three pseudo hyperplastic, two verrucous-pseudohyperplastic, and one case each of basaloid, papillary and mixed usual-basaloid carcinomas).
Lichen sclerosus was found present in all low-grade SCC cases.
Patients who had no lesions were younger, with a mean age of 44 years, in comparison with those who had precursor lesions, who had a mean age of 54 years, or with invasive SCC patients whose mean age was 68 years.
Immunohistochemistry for p16(INK4a) was undertaken in 19 precancerous lesions and they had found the following:
All differentiated PeINs (18 lesions) were negative, and one basaloid PeIN was found to be positive.
Oertell et al. [13] concluded that the frequent coexistence of lichen sclerosus, squamous hyperplasia, differentiated PeIN and low-grade SCC had suggested a common non-human papillomavirus related pathogenic pathway for preputial lesions, and had highlighted the importance of circumcision in symptomatic patients for the prevention of penile cancer.
Chaux et al. [24] stated the following:
From the pathogenic point of view, penile cancers might be grouped in human papillomavirus-related and unrelated tumours, each one of them associated with distinctive morphologic features.
The former tend to be predominantly composed of small, undifferentiated basaloid cells, with more or less prominent koilocytic changes, as well as the latter of keratinizing differentiated squamous cells.
The same cellular types tend to be found in precancerous lesions.
Upon the basis of these observations, they had constructed a novel nomenclature for penile precancerous lesions and classified them as penile intraepithelial neoplasia (PeIN) of differentiated, warty, basaloid, and warty-basaloid types.
Chaux et al. [24] undertook a study which was aimed to test the usefulness of immunohistochemical p16 overexpression, which has been considered to be a surrogate for high-risk human papillomavirus infection, using this classification system. Chaux et al. [24] pathologically evaluated 141 patients with PeIN, associated (123 cases) and un-associated (18 cases) with invasive cancer. The distribution of PeIN types was found to be differentiated, in 72%; basaloid, in 9%; warty-basaloid, in 7%; warty, in 4%; and mixed, in 7%. Chaux et al. [24] also reported the following:
There was a striking similarity with regard to the morphology of in situ and invasive squamous cell carcinomas.
Differentiated PeIN was found to be commonly associated with usual, verrucous, papillary, and other low-grade keratinizing variants of squamous cell carcinoma whereas in basaloid and warty carcinomas the presence of in situ lesions with similar morphology was habitual.
They had evaluated p16 overexpression utilizing a 4-tiered (0, 1, 2, and 3) pattern-based system.
In order to properly distinguish differentiated PeIN from in situ lesions with warty and/or basaloid features only pattern 3, which required full-thickness staining in all epithelial cells, was considered positive.
Utilizing this approach, there was a significant association of the negative patterns and differentiated PeIN and of the positive pattern and warty, basaloid, and warty-basaloid PeIN (P<0>
Basaloid variant was found to have the strongest association.
The sensitivity rate of p16 positivity for discriminating types of PeIN was of 82%, with a specificity of 100% and an accuracy of 95%.
Lichen sclerosus had been identified in 42 cases and their epithelial component was found to be p16 negative in all cases.
Even though more studies are required to confirm these observations, p16 overexpression seemed to be a useful tool for discriminating differentiated from warty, basaloid, and warty-basaloid PeIN.
Chaux et al. [31] stated the ensuing:
Many classification schemes for penile precancerous lesions had been proposed, however, none of them seemed to have correlated with the current understanding of penile cancer pathogenesis.
Recently, a system, which had taken into account morphology features and purported etiopathogenesis, was proposed, separating penile intraepithelial neoplasia (PeIN) in differentiated and warty/basaloid subtypes.
Chaux et al. [31] undertook a study to seek an immunohistochemistry profile that could be helpful with regard to the classification and differential diagnosis of penile epithelial abnormalities and precancerous lesions utilizing the aforementioned system. The immunohistochemistry study panel included stains for p16, p53, and Ki-67. For p16 immunostaining study, only full-thickness positivity in all epithelial cells was considered as positive; for p53 and Ki-67 immunostaining, patchy or diffuse nuclear positivity above the basal layer was regarded as positive. Seventy-four lesions in 59 patients had been selected and classified as follows: differentiated PeIN, 34 cases; squamous hyperplasia (SH), 21 cases; basaloid PeIN, 15 cases; and warty PeIN, 4 cases. Chaux et al. [31] summarized the results as follows
The mean age of the patients was 64 years.
Forty-two lesions that amounted to 56.8%, were located within the glans penis and 32 lesions that amounted to 43.2% were located within the foreskin.
Overexpression of p16 was useful for distinguishing SH from warty/basaloid PeINs (0% vs. 94.7%, P<0 P=0.519). >
Furthermore, p16 allowed the differentiation of differentiated and warty/basaloid PeINs (5.9% vs. 94.7%, P<0>
The immunohistochemistry staining study results for p53 allowed the separation of SH and differentiated PeIN (9.5% vs. 44.1%, P=0.0078) and SH and warty/basaloid PeIN (9.5% vs. 55.6%, P=0.0042). Ki-67 immunostain was useful for differentiating SH from differentiated PeIN (52.6% versus. 89.7%, P=0.0062) and SH from PeIN with warty and/or basaloid features (52.6% versus. 100%, P=0.0011).
There seemed to be a distinctive immunohistochemical profile for associated and precursor epithelial lesions of the penis.
SH was found to be p16 and p53 negative, with variable Ki-67 positivity. Differentiated PeIN was p16 negative and Ki-67 positive, with variable p53 positivity. Basaloid and warty PeINs were consistently p16 and Ki-67 positive, with variable p53 positivity.
Utilization of a triple p16/p53/Ki-67 immunohistochemical panel had been found to be helpful in the classification, differential diagnosis, and morphologic standardization of penile intraepithelial lesions.
Chaux et al. [11] reported the morphology features of 121 cases of atypical penile intraepithelial lesions. Chaux et al. [11] stated that the terminology penile intraepithelial neoplasia (PeIN) was utilized to encompass all of them, and the lesions had been classified into 2 major groups including: differentiated and undifferentiated groups. The latter was further divided into: warty, basaloid, and warty-basaloid subtypes. Ninety-five cases were found to be associated with invasive squamous cell carcinomas. Differentiated lesions had predominated accounting for 68% of cases, followed by warty-basaloid (14%), basaloid (11%), and warty (7%) subtypes. Multifocality was found in 15% of the cases. Differentiated lesions were found to be preferentially located within foreskin, whereas warty and/or basaloid subtypes were identified and noted to be more prevalent within the glans penis. The former lesions were preferentially observed in association with keratinizing variants of squamous carcinoma; however, the latter subtypes were found mostly in conjunction with invasive warty, basaloid, and warty-basaloid carcinomas. Lichen sclerosus was found to be present in 51% of cases of differentiated lesions and absent in warty and/or basaloid subtypes. Chaux et al. [11] summated that:
PeIN could be classified into 4 distinctive morphological subtypes.
The proper pathological characterization of these lesions might provide important clues to the understanding of the pathogenesis and natural history of penile cancer.
Canete-Portillo et al. [32] stated the d following:
Several classification schemes for penile precancerous lesions had been proposed, however, none of them had seemed to correlate with the current understanding of penile cancer pathogenesis.
Recently, a system, which had taken into account morphology features and purported etiopathogenesis, had been proposed, separating penile intraepithelial neoplasia (PeIN) in differentiated and warty/basaloid subtypes.
Canete-Portillo et al. [32] undertook a study to seek an immunohistochemistry staining profile that could be helpful in the classification and differential diagnosis of penile epithelial abnormalities and precancerous lesions utilizing the aforementioned system. The immunohistochemistry staining panel included stains for p16, p53, and Ki-67. For p16 immunostaining, only full-thickness positivity in all epithelial cells was considered as positive; for p53 and Ki-67 immunostaining, patchy or diffuse nuclear positivity above the basal layer was considered as positive. Canete-Portillo et al. [32] reported the following:
Seventy-four lesions in 59 patients were selected and they were classified as follows: differentiated PeIN, 34 cases; squamous hyperplasia (SH), 21 cases; basaloid PeIN, 15 cases; and warty PeIN, 4 cases.
The mean age of patients was 64 years. Forty-two lesions (56.8%) were located in the glans and 32 (43.2%) in the foreskin.
Overexpression of p16 was noted to be useful for distinguishing SH from warty/basaloid PeINs (0% versus. 94.7%, P<0 P=0.519). P=0.0078) P=0.0042). >
Ki-67 immunostaining was found to be useful for distinguishing SH from differentiated PeIN (52.6% versus. 89.7%, P=0.0062) and SH from PeIN with warty and/or basaloid features (52.6% versus. 100%, P=0.0011).
There seemed to be a distinctive immunohistochemical profile for associated and precursor epithelial lesions of the penis.
SH was p16 and p53 negative, with variable Ki-67 positivity.
Differentiated PeIN was found to be p16 negative and Ki-67 was positive, with variable p53 positivity.
Basaloid and warty PeINs were found to be consistently p16 and Ki-67 positive, with variable p53 positivity.
Utilization of a triple p16/p53/Ki-67 immunohistochemical panel was found to be helpful in the classification, differential diagnosis, and morphologic standardization of penile intraepithelial lesions
Velazquez et al. [33] stated the following:
Penile squamous cell carcinomas (SCCs) and their corresponding precancerous lesions could be classified in 2 major groups: human papillomavirus (HPV) related and HPV unrelated.
In the former (warty and basaloid SCC), there tends to be a predominance of undifferentiated basaloid cells.
In the latter (for example, usual, papillary, and verrucous SCC), the predominant cell tends to be larger with abundant eosinophilic cytoplasm.
Based upon these morphology features, a new terminology, "penile intraepithelial neoplasia" (PeIN), was proposed.
PeIN was in addition, subclassified into differentiated and undifferentiated, with the latter being subdivided into basaloid, warty, and warty-basaloid subtypes.
Macroscopically, PeIN subtypes are indistinguishable.
Microscopically, differentiated PeIN tends to be characterized by acanthosis, parakeratosis, enlarged keratinocytes with abundant "pink" cytoplasm (abnormal maturation), and hyperchromatic cells in the basal layer.
In basaloid PeIN the epithelium tends to be replaced by a monotonous population of uniform, small, round, and basophilic cells.
Warty PeIN is typified by a spiky surface, prominent atypical parakeratosis, and pleomorphic koilocytosis.
Warty-basaloid PeIN does tend to demonstrate features of both warty and basaloid PeIN.
There is a significant association of subtypes of PeIN with specific variants of invasive SCCs.
This represents a simple and reproducible nomenclature for penile precancerous lesions based upon cell type and differentiation. It does take into account the similarities between vulvar and penile pathology and the postulate of a bimodal pathway of penile cancer progression. Fernández-Nestosa et al. [14] stated that Laser capture microdissection-polymerase chain reaction (LCM-PCR) supported by p16 was utilized for the first time to demonstrate human papillomavirus (HPV) DNA within histologically specific penile lesions, that were as follows: squamous hyperplasia (12 lesions, in 10 patients), flat lesions (12 lesions, in 5 patients), condylomas (26 lesions, in 7 patients), penile intraepithelial neoplasia (PeIN) (115 lesions, in 43 patients), and invasive squamous cell carcinomas (26 lesions, in 26 patients). HPV was identified by whole-tissue section and LCM-PCR. LCM had proven to be more precise in comparison with whole-tissue section in assigning individual genotypes to specific lesions. They reported the following results:
HPV was negative or very infrequent in squamous hyperplasia, differentiated PeIN, and low-grade keratinizing variants of carcinomas.
HPV was found to be strongly associated with condylomas, warty/basaloid PeIN, adjacent flat lesions, and warty/basaloid carcinomas.
A single HPV genotype was identified in each lesion.
Some condylomas and flat lesions, especially those with atypia, were found to be preferentially associated with high-risk HPV.
Unlike invasive carcinoma, in which few genotypes of HPV were involved, there were 18 HPV genotypes in PeIN, usually HPV 16 in basaloid PeIN however, marked HPV heterogeneity in warty PeIN (11 different genotypes).
Variable and multiple HPV genotypes were identified within multicentric PeIN, whilst unicentric PeIN was found to be usually related to a single genotype.
There was a correspondence found among HPV genotypes within invasive and associated PeIN. p16 was positive in the majority of HPV-positive lesions with the exception of condylomas that contained LR-HPV. p16 was usually negative in squamous hyperplasia, differentiated PeIN, and low-grade keratinizing variants of squamous cell carcinomas.
They summarized that:
They had demonstrated that LCM-PCR was a superior research technique for the investigation of HPV genotypes in intraepithelial lesions.
Their significant finding was the heterogeneity of HPV genotypes in PeIN and the differential association of HPV genotypes with subtypes of PeIN.
The presence of atypia and high-risk HPV in condylomas and adjacent flat lesions had suggested a precursor role, and the correspondence of HPV genotypes in invasive carcinomas and associated PeIN had indicated a causal relation.
The data they had presented supported the bimodal postulate of penile cancer carcinogenesis in HPV-driven and non-HPV-driven carcinomas and justify the current WHO pathologic classification of PeIN in specimens
Fernández-Nestosa et al. [18] stated the ensuing:
Penile intraepithelial neoplasia (PeIN) currently has been classified in human papillomavirus (HPV)- and non-HPV-related subtypes with variable HPV genotypes.
PeINs have tended to be frequently associated with other intraepithelial lesions within the same specimen.
Fernández-Nestosa et al. [18] undertook a study which was aimed to detect and compare HPV genotypes in PeINs and associated lesions utilising high-precision laser capture microdissection-polymerase chain reaction and p16INK4a immunostaining. They evaluated resected penile specimens from 8 patients and they had identified 33 PeINs and 54 associated lesions. The commonest subtype was warty PeIN, followed by warty-basaloid and basaloid PeIN. Associated lesions that were found in the study were classical condylomas (17 cases), atypical classical condylomas (2 cases), flat condylomas (9 cases), atypical flat condylomas (6 cases), flat lesions with mild atypia (12 cases), and squamous hyperplasia (8 cases). Following a comparison, identical HPV genotypes were identified in pen and associated lesions in most of the patients (7 of 8 patients). HPV16 was the commonest genotype found present in both PeIN and corresponding associated lesion (50% of the patients). Non-specific flat lesions that contained mild atypia, classical condylomas, and atypical condylomas were the type of associated lesions that were most commonly related to HPV16. Other high-risk HPV genotypes that were found in PeIN and associated non-specific flat lesion with mild atypia were HPV35 and HPV39. They also stated that within their study of HPV in the microenvironment of penile precancerous lesions, they had identified identical high-risk HPV genotypes in pen and classical, flat, or atypical condylomas and, specially, in nonspecific flat lesions with mild atypia. They furthermore iterated that it is possible that some of these lesions represented hitherto unrecognized precancerous lesions
Fernández-Nestosa et al. [34] stated the following:
There are few pathology or molecular studies of penile precancerous lesions, and the majority refers to lesions that were associated with invasive carcinomas.
Penile Intraepithelial Neoplasia (PeIN) is classified in two morphology and distinctive molecular groups, non-HPV and HPV-related with special subtypes.
Fernández-Nestosa et al. [34] undertook a study which had a primary purpose of classifying PeIN morphologically, detecting HPV genotypes and determining their distribution according to PeIN subtypes. Their secondary aim was to evaluate the p16INK4a immunostaining as a possible HPV surrogate for high-risk HPV infection in penile precancerous lesions. The samples consisted of 84 PeIN cases, part of a retrospective cross-sectional analysis of 1095 penile carcinomas was designed to estimate the HPV DNA prevalence in penile cancers utilising PCR and p16INK4a immunostaining. Penile Intraepithelial Neoplasia (PeIN) was classified in HPV-related (basaloid, warty-basaloid, warty, hybrid, and mixed subtypes) and non-HPV-related (differentiated), the former was the most frequent. PeIN subtypes were differentiated (non-HPV-related) and basaloid, warty-basaloid, warty, hybrid and mixed (HPV-related). Basaloid PeIN was the most commonly diagnosed subtype, and HPV16 was documented as the most frequent HPV genotype they had detected. Warty-basaloid and warty PeIN had shown a more heterogeneous genotypic composition. Most HPV genotypes were found to be high-risk but low-risk HPV genotypes were also found present within a few cases (4%). A single HPV genotype was identified in 82% of HPV positive cases. On the contrary, multiple genotypes were found in the remaining 18% of cases. They iterated the following:
The findings in their study had supported the paradigm that penile in situ neoplasia, like its invasive counterparts, is HPV dependent or independent and has distinctive morphology subtypes readily identified in routine practice.
Considering that HPV16 is clearly the predominant type, and that the three available vaccines have HPV16, all of them would be suitable for vaccination programs; the price of the vaccines would be probably the main determinant to choose the vaccine.
Canete-Portillo et al. [35] stated the following:
Since 1995 it had been known that tumours that harbour human papillomavirus (HPV) preferentially show basaloid or condylomatous histology features, while HPV-negative tumours have a different morphology.
New classification models do separate sub-types of penile squamous cell carcinomas in two groups, non–HPV- and HPV-related.
It had been purported that HPV-related tumours do have better prognosis.
Other features such as inflammatory cell–rich medullary, clear-cell, and lymphoepithelioma-like patterns had also been iterated to be also strong predictors of the presence of HPV.
These tumours are morphologically distinctive and with some experience, pathologists might recognize them after routine haematoxylin and eosin staining.
Occasionally, p16 immunostaining might aid in the differential diagnosis.
The gold standard for HPV detection is polymerase chain reaction, however, this technique has been expensive and had not been available within most pathology laboratories.
In situ hybridization is useful and p16 immunostaining could identify HPV in about 85% of cases.
Correlation EXISTS between morphology and outcome.
Hoekstra et al. [9] undertook a study to determine the incidence of penile intraepithelial neoplasia in the Netherlands utilising a nationwide histopathology registry and to discuss the nomenclature of premalignant penile lesions.
Hoekstra et al. [9] collected data from patients in the Netherlands who were diagnosed with a premalignant penile lesion between January 1998 and December 2007 from the nationwide histopathology registry (PALGA); this database covered all pathology reports of inhabitants in the Netherlands. The premalignant lesions included were erythroplasia of Queyrat; Bowen's disease; bowenoid papulosis; mild, moderate and severe dysplasia; and carcinoma in situ of the penis. The terminology that was utilised in the pathology reports was translated to penile intraepithelial neoplasia. The grading was made analogous to that of vulvar premalignant lesions. Hoekstra et al. [9] summarized the results as follows:
The PALGA database had enrolled 380 patients who had premalignant penile lesions.
Severe premalignant lesions, penile intraepithelial neoplasia III, were identified in 254 patients (67%), penile intraepithelial neoplasia II in 84 (22%) and penile intraepithelial neoplasia I in 42 patients (11%).
Majority of the lesions were located upon the prepuce in 45% of cases, followed by the glans penis in 38% of the cases and the penile shaft in 3% of the cases.
The median age of patients who had penile intraepithelial neoplasia was 58 years.
Progression to malignant disease had occurred in 2% of patients for penile intraepithelial neoplasia I versus 7% for penile intraepithelial neoplasia III, in 26 patients.
Hoekstra et al. [9] made the ensuing conclusions
Penile intraepithelial neoplasia is a rarely diagnosed clinical condition.
Because of the wide variation of terminologies that are used for premalignant intraepithelial neoplasia of the penis, they would recommend restricting this nomenclature to penile intraepithelial neoplasia.
Aynaud et al. [36] evaluated the study of the existence of the morphology features specific for penile intraepithelial neoplasia (PIN), 1000 male sexual partners of women with genital condyloma or intraepithelial neoplasia. Aynaud et al. [36] presented ninety-two patients who had lesions that suggested intraepithelial neoplasia (pigmented or leukoplastic papules, keratinized condylomata, or erythroplastic macules) which underwent biopsy for histology and virologic studies. Aynaud et al. [36] summarized the results as follows:
Histology results had shown penile intraepithelial neoplasia in 93% of the specimens.
Human papillomavirus (HPV) DNA from potentially oncogenic papillomaviruses was identified in 75% of patients who had Grade I PIN, in 93% of patients who had Grade II PIN, and in all patients who had Grade III PIN.
Uncircumcised and circumcised men had shown the same rate (52% versus. 45%; odds ratio [OR] = 1.3; 95% confidence interval, 0.97-1.73) of HPV-associated lesions, on the other hand, the rate of PIN was significantly higher in uncircumcised men in comparison with than in circumcised men (10% vs. 6%; OR = 1.77; 95% confidence interval, 1.02-3.07).
The mean age of patients who had Grade III PIN was 7 years older the mean age of patients who had Grade I PIN, which had indicated a step progression similar to that of cervical intraepithelial neoplasia.
Aynaud et al. [36] made the following conclusions:
Morphology does seem to be a specific enough indicator of PIN.
More data are required to ascertain whether treatment of PIN might contribute to the prevention of cervical or penile cancer. If so, the morphology criteria the had described would be clinically useful.
Porter, et al. [37] stated the following:
Penile intraepithelial neoplasia (PIN) is the terminology that is used to describe: erythroplasia of Queyrat (EQ), Bowen's disease (BD) and bowenoid papulosis (BP).
These conditions are distinct clinical entities and do have different epidemiology and aetiology associations and prognostic implications.
Porter, et al. [37] undertook a study to describe the manifestation and treatment of patients who had PIN. Porter, et al. [37] described thirty‐five patients who had presented with PIN over a 7‐year period. Porter, et al. [37] summarized the results as follows:
Their observations included:
patients who had BP are younger than those with EQ or BD and sometimes have a history of immunosuppression;
(b) patients who had BP usually have a history or clinical evidence of previous genital human papillomavirus infection;
(c) patients who had EQ often had a concurrent penile dermatosis (lichen sclerosus or lichen planus);
(d) patients who had PIN were usually uncircumcised;
and (e) response to treatment of BP depended upon the integrity of the immune system.
Porter, et al. [37] made the following conclusions:
They had recommended vigorous treatment of all patients who have PIN, including circumcision.
Smoking must be actively discouraged.
Patients need to undergo life‐long follow‐up and partners of patients who have BP should be screened for other forms of intraepithelial neoplasia (cervical and anal).
da Costa Nunes et al. [38] wrote an article to promote a literature revision of the relationship between the prevention of intraepithelial neoplasms (PeIN) and invasive penile cancer, and human papillomavirus (HPV) vaccination, aiming to enumerate the pros and cons of immunization. da Costa Nunes et al. [38] stated the following:
The immunization against the HPV is sufficiently safe and many countries had incorporated the vaccine into their immunization calendar.
In Comparison with men, the sampling size and the evidence quality of scientific researches among the female population were more robust.
Some randomized and nonrandomized studies had indicated that vaccination reduces the incidence of genital warts and no PeIN and penile cancer cases were developed in the vaccinal group. Nevertheless, 70% of patients could evolve with the neoplasia despite having been immunized and even among HPV infected patients, only 1% would develop cancer.
da Costa Nunes et al. [38] made the ensuing summations:
Results of studies about vaccination against HPV and prevention on penile cancer had been conflicting and the main academic urology societies still had not incorporated vaccination of men in their guidelines.
Future studies would be necessary to confirm the efficiency and cost–benefit of the vaccine in men in order to prevent intraepithelial neoplasms and invasive penile cancer.
RMarkos et al. [39] made the ensuing summating discussions:
The incidence of reporting of penile intraepithelial neoplasia (PIN) by genitourinary medicine clinics in the United Kingdom is not common.
The reporting of higher incidence, in majority of international studies, had been suggestive of under-diagnosis of PIN lesions in the United Kingdom, which does lead to improper treatment and follow-up of patients.
A systematic literature review was undertaken, regarding the current state of management of PIN and the possible avenues of improvement in the diagnosis and follow-up.
The role of genitourinary medicine clinics was examined, in view of the high number of patients that manifest with genital dermatological conditions, in whom there were patients with non-identified PIN lesions.
The notable increase in reporting of vulval intraepithelial neoplasia had been associated with an increase in vulval cancer, especially in younger patients.
The possibility of a similar trend in penile lesions does need to be observed and the association between high-risk human papillomavirus (HPV) types, and genital intraepithelial neoplasia and cancer, had been recognized and therefore an increased incidence in the diagnosis of HPV associated lesions should be considered.
Kravvas et al. [40] determined the incidence of penile intraepithelial neoplasia in the Netherlands utilizing a nationwide histopathology registry and discussed the nomenclature of premalignant penile lesions.
Kravvas et al. [40] collected data from patients in the Netherlands who were diagnosed with a premalignant penile lesion between January 1998 and December 2007 from the nationwide histopathology registry (PALGA); this database does cover all pathology reports of inhabitants in the Netherlands. The premalignant lesions that were included were: erythroplasia of Queyrat; Bowen's disease; bowenoid papulosis; mild, moderate and severe dysplasia; and carcinoma in situ of the penis. The terminology that was used in the pathology reports was translated to penile intraepithelial neoplasia. The grading was made analogous to that of vulvar premalignant lesions. Kravvas et al. [40] summarized the results as follows: The PALGA database had enrolled 380 patients who had premalignant penile lesions. Severe premalignant lesions, penile intraepithelial neoplasia III, were found in 254 patients which amounted to 67% of the patients, penile intraepithelial neoplasia II in 84 patients which amounted to 22% of patients and penile intraepithelial neoplasia I in 42 patients which amounted to 11% of the patients. Most lesions were located upon the prepuce which amounted to 45% of the patients, followed by glans (38%) and shaft (3%). The median age of patients with penile intraepithelial neoplasia was 58 years. Progression to malignant disease occurred (2% for penile intraepithelial neoplasia I vs 7% for penile intraepithelial neoplasia III) in 26 patients. Kravvas et al. [40] made the ensuing conclusions:
Penile intraepithelial neoplasia is an uncommonly diagnosed condition.
In view of the wide variation of terminologies used for premalignant intraepithelial neoplasia of the penis, they would recommend restricting this nomenclature to penile intraepithelial neoplasia.
Deen et al. [41] stated the following:
Penile intraepithelial neoplasia (PIN), or penile squamous cell carcinoma in situ, is an uncommon disease and might be associated with high morbidity and mortality.
In an attempt to avoid surgical intervention, which might result in poor cosmetic and functional outcomes for patients, many non-invasive treatments had been trialled with variable success rates.
They had undertaken a review which had summarised the available literature describing the use of topical imiquimod for PIN. While the results of their review had been limited by the heterogeneity of the methods and follow ups of the included case series and case reports, they had highlighted the fact that patients with PIN have variable responses to imiquimod which seem less effective than was previously reported. Therefore, if imiquimod treatment is instituted in PIN, clinicians should counsel their patients about the effects associated with treatment, the potential for a partial or no response to treatment, and the risk of recurrence. A strict follow-up plan is also necessary in order to monitor both patient adherence and PIN recurrence pursuant to treatment completion, in case surgical options need to be considered.
Baldur-Felskov et al. [42] assessed the trends in incidence of penile cancer during 1978 and 2008 and high-grade penile intraepithelial neoplasia (PIN2/3) during 1998 and 2008 in Denmark. Baldur-Felskov et al. [42] estimated using two nationwide registries, age- and period-specific incidence rates. They used log-linear Poisson regression analysis to estimate average annual percentage change (AAPC) and 95% confidence intervals (CI). Baldur-Felskov summarized the results as follows:
They identified 1,488 men with penile cancer and 285 men with PIN2/3.
The incidence of penile cancer increased from 1.0 to 1.3 per 100,000 men-years in 1978 -1979 to 2006–2008; this represented an AAPC of 0.8% (95% CI: 0.17–1.37). Squamous cell carcinoma (SCC) was the commonest histology type (91.7%).
The median age at diagnosis was 67 years, and the age-specific incidence rate of penile SCC had risen with increasing age.
The incidence rate of PIN2/3 had increased significantly (0.5 to 0.9 per 100,000 men-years) in 1998–1999 to 2006–2008, and this did represent an AAPC of 7.1% (95% CI: 3.30–11.05).
Baldur-Felskov et al. [42] made the ensuing conclusions:
The incidence of penile cancer had increased in 1978–2008 in Denmark, and the same increase applied to PIN2/3 in 1998–2008.
A high prevalence of human papillomavirus (HPV) and a low circumcision rate in Denmark might partly explain their results.
Gross and Pfister. [43] stated the following:
Utilizing PCR, the overall prevalence of human papillomavirus (HPV) DNA in carcinoma of penis is about 40% to 50%, which is similar to the detection rate of HPV-DNA in carcinoma of vulva (50%).
In analogy cancer of the vulva, two different pathways carcinogenesis of penis seem to exist.
In contrast to basaloid as well as warty cancers of the penis, which are regularly HPV-associated (about 80% to 100%), only a part of keratinizing and verrucous penile carcinomas, appear to be related with HPV (33% to 35%), comprising Bowen’s disease, erythroplasia of Queyrat, and Bowenoid papulosis are precursor lesions of basaloid and warty carcinomas of the penis.
Penile intra-epithelial neoplasms
[44] Wikström A, Hedblad MA, Syrjänen S. Penile intraepithelial neoplasia: histopathological evaluation, HPV typing, clinical presentation and treatment. Journal of the European Academy of Dermatology and Venereology. 2012 Mar;26(3):325-330.
Wikström et al. [44] stated that genital human papillomavirus (HPV) infection in male patients could cause great variety of lesions, majority of which are benign, but some are categorised as penile intraepithelial neoplasia (PIN). Wikström et al. [44] undertook a study by (a) performing HPV testing and correlating to histopathology from genital HPV-induced lesions in men; and (b) by determining the clinical manifestation and treatment of PIN. They included men attending the venereological clinic at Karolinska Hospital for surgical treatment of genital HPV infection. Two biopsies were taken from each patient, one for histopathology examination and one for HPV typing utilizing PCR. Patients who had exhibited PIN were selected for further analysis. The lesions were described, and treatment and follow-up data were recorded by Wikström et al. [44]
Wikström et al. [44] summarized the results as follows:
Forty-seven of 303 that amounted to 16% male HPV patients had exhibited PIN lesions.
Nineteen were afflicted with lesions which had been denominated as PIN I, 13 had PIN II lesions and 15 had PIN III lesions.
Macular lesions were the commonest which amounted to 27.
Ninety-three percent of the analysed PIN lesions were noted to be HPV-positive.
Three of twelve that amounted to 25% of HPV-positive PIN III lesions contained only low-risk HPV types in comparison to 13 of 19 that amounted 68% of PIN I lesions.
In addition, 9 of 12 that amounted to 75% of HPV-positive PIN III lesions contained high-risk HPV types compared to 6 of 19 (32%) PIN I-lesions. (P = 0.029).
HPV 6 and HPV 16 were the most prevalent genotypes. A mean of four surgical treatment sessions was performed during a treatment period of mean 27 months.
They concluded that PIN is highly HPV-positive, can show differing clinical pictures and is difficult to treat.
Fernández-Nestosa et al. [45] stated the following:
There are few pathological or molecular studies of penile precancerous lesions, and the majority refers to lesions that are associated with invasive carcinomas.
Penile intraepithelial neoplasia (PeIN) has been classified in two morphology and distinctive molecular groups, non-HPV and HPV-related with special subtypes.
The primary purpose of their international series was to classify PeIN morphology, detect HPV genotypes and determine their distribution according to PeIN subtypes. Their secondary aim was to evaluate the p16INK4a immunostaining as a possible HPV surrogate for high-risk HPV infection in penile precancerous lesions. The samples consisted of 84 PeIN cases, part of a retrospective cross-sectional analysis of 1095 carcinomas of penis designed to estimate the HPV DNA prevalence in cancers of the penis utilizing PCR and p16INK4a immunostaining.
Penile Intraepithelial Neoplasia (Pekin) was classified in HPV-related (basaloid, warty-basaloid, warty, hybrid, and mixed subtypes) and non-HPV-related (differentiated), the former being the most frequent. PeIN sub-types that were differentiated (non-HPV-related) and basaloid, warty-basaloid, warty, hybrid and mixed (HPV-related). Basaloid PeIN was the commonest diagnosed subtype, and HPV16 was the most frequent HPV genotype that was detected. Warty-basaloid and warty Pekin had shown a more heterogeneous genotypic composition. Majority of HPV genotypes were high-risk however, low-risk HPV genotypes were also present in a few cases (4%). A single HPV genotype was detected in 82% of HPV positive cases. On the contrary, multiple genotypes were detected in the remaining 18% of cases. The findings in their study had supported the paradigm that penile in situ neoplasia, like its invasive counterparts, is HPV dependent or independent and has distinctive morphological subtypes readily identified in routine practice. Considering that HPV16 was clearly the predominant type, and that the three available vaccines have HPV16, all of them would be suitable for vaccination programs; the price of the vaccines would be probably the main determinant to choose the vaccine.
Cañete-Portillo et al. [30] stated the following:
Lichen sclerosus (LSc) with penile cancer is found in about two thirds of specimens.
It had been postulated that that LSc represents a precancerous condition.
In order to qualify as such, in addition to cytology atypia and similarity with the invasive tumour, a spatial correlation between LSc and neoplastic lesions does need to be demonstrated.
Cañete-Portillo et al. [30] undertook a study to evaluate such a spatial relationship. They evaluated circumcision (28 cases) and penectomy (81 cases) specimens. All cases had LSc, penile intraepithelial neoplasia (PeIN), and/or invasive squamous cell carcinomas. Cañete-Portillo et al. [30] examined LSc in relation to invasive carcinoma, PeIN, and normal epithelia. Invasive squamous cell carcinomas, which were classified according to the World Health Organization criteria as non–human papillomavirus (HPV)-related and HPV-related PeIN, were present in 100 cases. Non-HPV-related (differentiated) PeIN was the commonest sub-type associated with LSc (89%). There were 5 spatial patterns which had been identified including: (1) LSc adjacent to PeIN (23%), (2) LSc adjacent and comprising PeIN (42%), (3) LSc next to and within invasive carcinomas (8%), (4) LSc throughout the sequence PeIN-invasive carcinoma (24%), and (5) LSc was separate (with normal tissue between the lesions) from PeIN and/or invasive carcinomas in a minority of cases (3%). Cañete-Portillo et al. [30] stated the following:
LSc within the cancer had not been previously described.
In their series, they found 35 cases with LSc within invasive carcinomas.
The striking continuous spatial relationship among LSc, PeIN, and/or invasive carcinoma as demonstrated in their study might be a necessary (but not sufficient) condition for the hypothesis postulating LSc as a penile precancerous lesion.
Guerrero et al. [46] stated the following:
Majority of human papillomavirus (HPV)-independent penile squamous cell carcinomas (PSCCs) originate from an intraepithelial precursor called differentiated penile intraepithelial neoplasia, typified by atypia limited to the basal layer with marked superficial maturation.
Previous studies related to vulvar cancer, which has a similar dual etiopathogenesis, had demonstrated that about one fifth of HPV-independent precursors are morphologically indistinguishable from high-grade squamous intraepithelial lesions (HSILs), the precursor of HPV-associated carcinomas.
Nevertheless, such lesions had not been described in PSCC.
Guerrero et al. [46] summarized their study as follows:
From 2000 to 2021, 55 surgical specimens of PSCC were identified. In all cases, thorough morphology assessment, HPV DNA detection, and p16, p53, and Ki-67 immunohistochemical (IHC) staining was undertaken. HPV-independent status was assigned based upon both negative results for p16 IHC and HPV DNA. Thirty-six of the 55 PSCC that amounted to 65% were HPV-independent. An intraepithelial precursor was identified in 26 cases out of 36 cases that amounted to 72%. Five of them that amounted to 19% had basaloid features, morphologically indistinguishable from HPV-associated HSIL. The median age of the 5 patients was 74 years and the ages of the patients had ranged between 67 years and 83 years. All 5 cases were p16 and DNA HPV-negative. Immunohistochemically, 3 cases had shown an abnormal p53 pattern, and had 2 shown wild-type p53 staining. The associated invasive carcinoma was noted to be basaloid in 4 cases and the usual (keratinizing) type in 1.
Guerrero et al. [46] made the ensuing conclusions:
A small proportion of HPV-independent PSCC might arise upon adjacent intraepithelial lesions morphologically identical to HPV-associated HSIL.
This unusual histology pattern had not been previously characterized in detail in PSCC. p16 IHC is a valuable tool to identify these lesions and differentiate them from HPV-associated HSIL.
Stojanović et al. [47] reported a case of a 36-year-old man who had a penile intraepithelial neoplasia who was evaluated at the Outpatient Clinic of the Department of Dermato-venereology Diseases of the Clinical Centre of Vojvodina in December of 2010. The patient was referred to the facility by a urologist and had histopathology reports of 4 biopsy-specimens taken from different plaques on his glans penis. Biopsy samples were collected from lesions which were clinically diagnosed as leukoplakia. The histopathology examination findings of all biopsy specimens had shown: “dysplasio epitheliiplanocellularis gradus levioris et partim gradus mediocris diffusa”. Given the histopathology diagnosis, the patient was referred to a dermatologist for conservative therapy of these lesions, avoiding radical surgery. During his admission, the patient had manifested with slightly indurated erythematous plaques with some desquamation at the surface, and a tendency for diffuse involvement of the entire glans penis. Topical 5% imiquimod cream was applied on the lesions once a day and was washed off after 8 hours during 10 weeks. Check-ups were scheduled for every other week in order to assess the course and progress of topical treatment. No significant side effects were observed, except for acute local inflammation which was accompanied by mild exudation and itching. After 10 weeks of treatment, complete regression of lesions resulted, and in the ensuing period of 18 months up to the time of publication of the article, no recurrence was observed
NUNES et al. [38] undertook a review which had the objective to promote a literature revision of the relationship between the prevention of intraepithelial neoplasms (PeIN) and invasive cancer of penis, and human papillomavirus (HPV) vaccination, which was aimed to enumerate the pros and cons of immunization. NUNES et al. [38] stated that their recent findings included the following:
Immunization against the HPV is sufficiently safe and many countries had incorporated the vaccine to their immunization calendar.
In comparison with men, the sampling size and the evidence quality of scientific researches among the female population are more robust.
Some randomized and nonrandomized studies had suggested that vaccination does reduce the incidence of genital warts and no PeIN and penile cancer cases were developed in the vaccinal group.
Nevertheless, 70% of patients could evolve with the neoplasia despite having been immunized and even among HPV infected patients, only 1% would develop cancer.
The studies about vaccination against HPV and prevention on cancer of penis are conflicting and the main academic urology societies still had not incorporated vaccination of men in their guidelines.
Future studies would be necessary in order to confirm the efficiency and cost-benefit of the vaccine in men so as to prevent the development of intraepithelial neoplasms and invasive penile cancer.
Fernández-Nestosa et al. [18] iterated the ensuing:
Penile intraepithelial neoplasia (PeIN) was at the time of publication of their article classified into human papillomavirus (HPV)- and non-HPV-related subtypes with variable HPV genotypes.
PeINs had been frequently associated with other intraepithelial lesions within the same specimen.
Fernández-Nestosa et al. [18] undertook a study which was aimed to detect and compare HPV genotypes in PeINs and associated lesions utilising high-precision laser capture microdissection-polymerase chain reaction and p16INK4a immunostaining. Fernández-Nestosa et al. [18] evaluated resected penile specimens from 8 patients and they had identified 33 PeINs and 54 associated lesions. The commonest sub-type was warty PeIN, followed by warty-basaloid and basaloid PeIN. They classified associated lesions which included: classical condylomas (17 cases), atypical classical condylomas (2 cases), flat condylomas (9 cases), atypical flat condylomas (6 cases), flat lesions with mild atypia (12 cases), and squamous hyperplasia (8 cases). After a comparison, they found identical HPV genotypes in PeIN and associated lesions in the majority of the patients (7 of 8 patients). HPV16 was the commonest genotype present in both PeIN and corresponding associated lesion (50% of the patients). Non-specific flat lesions associated with mild atypia, classical condylomas, and atypical condylomas were the type of associated lesions that were most commonly related to HPV16. Other high-risk HPV genotypes that were present in PeIN and associated nonspecific flat lesion with mild atypia included HPV35 and HPV39. In their study of HPV in the microenvironment of penile precancerous lesions, Fernández-Nestosa et al. [18] identified identical high-risk HPV genotypes in PeIN and classical, flat, or atypical condylomas and, specially, in nonspecific flat lesions with mild atypia. Fernández-Nestosa et al. [18] iterated that it is possible that some of these lesions did represent hitherto unrecognized precancerous lesions.
Fernández-Nestosa, et al. [45] stated the ensuing:
There are few pathology or molecular studies of penile precancerous lesions, and most of them refer to lesions that are associated with invasive carcinomas.
Penile Intraepithelial Neoplasia (PeIN) is classified into two morphology and distinctive molecular groups, non-HPV and HPV-related with special sub-types.
The primary purpose of their international series was to classify PeIN morphology, detect HPV genotypes and determine their distribution according to PeIN subtypes. A secondary aim was to ascertain the p16INK4a immunostaining as a possible HPV surrogate for high-risk HPV infection in penile precancerous lesions. Their samples had consisted of 84 PeIN cases, part of a retrospective cross-sectional analysis of 1095 penile carcinomas was designed to estimate the HPV DNA prevalence in penile cancers utilising PCR and p16INK4a immunostaining. They classified Penile Intraepithelial Neoplasia (PeIN) into: HPV-related (basaloid, warty-basaloid, warty, hybrid, and mixed subtypes) and non-HPV-related (differentiated), the former being the most frequent.
Fernández-Nestosa, et al. [45] summarized the rest of their results as follows:
PeIN sub-types included: differentiated (non-HPV-related) and basaloid, warty-basaloid, warty, hybrid and mixed (HPV-related).
Basaloid PeIN was the commonest diagnosed subtype, and HPV16 was the most frequent HPV genotype which had been detected.
Warty-basaloid and warty PeIN had shown a more heterogeneous genotypic composition.
Majority of HPV genotypes were high-risk but low-risk HPV genotypes were also found present within a few cases (4%).
A single HPV genotype was identified in 82% of HPV positive cases. In contrast, multiple genotypes were identified in the remaining 18% of cases.
Fernández-Nestosa, et al. [45] made the ensuing concluding iterations:
The findings in their study had supported the paradigm that penile in situ neoplasia, like its invasive counterparts, is HPV dependent or independent and it has distinctive morphology sub-types readily identified in routine practice.
Taking into consideration that HPV16 is clearly the predominant type, and that the three available vaccines had HPV16, all of them would be suitable for vaccination programs; the price of the vaccines would be probably the main determinant to choose the vaccine.
Sabater-Marco et al. [48] described the association of balanitis xerotica obliterans and differentiated penile intraepithelial neoplasia (PeIN) with dermal elastosis and “bramble-bush” elastic fibres in a diabetic patient who had no history of penicillamine intake. Sabater-Marco et al. [48] reported an 84-year-old man who had presented with urethral obstruction syndrome which required postectomy, meatotomy, and foreskin excision. Histopathology examination of the specimen revealed changes of lichen sclerosus and differentiated PeIN. Orcein staining had shown striking dermal elastosis and trans-epidermal elimination of elastic fibres. At higher magnification, multiple serrations and buds arising from the borders of the elastic fibres were identified giving the so-called bramble-bush appearance. Sabater-Marco et al. [48] made the ensuing summating discussions:
Balanitis xerotica obliterans is considered to be a premalignant disease, and 14% of patients do have evidence of PeIN.
The differentiated sub-type could be difficult to diagnose in view of the minimal basal cell atypia, so a striking dermal elastosis, which might even occur before the neoplasm becomes invasive, might facilitate its diagnosis.
The terminology “acquired perforating dermatosis” does seem appropriate to describe those cases of perforating elastosis which occurs in adults with systemic diseases.
The bramble-bush appearance of elastic fibres is not specific for penicillamine-induced elastopathy, and it might occur within other diseases, such as diabetes mellitus. This peculiar morphology of elastic fibres might be related to the enzymatic imbalance between matrix metalloproteinases and lysyl oxidase, an enzyme that is required for the cross-linking of elastic fibres.
Kristiansen et al. [49] stated the ensuing;
Studies on risk factors for penile intraepithelial neo?plasia had been small in size, had not differentiated penile intraepithelial neoplasia from invasive cancer, as well as had relied upon self-reported information. Kristiansen et al. [49] undertook a study which investigated risk factors for penile intraepithelial neoplasia in a cohort of 580 penile intraepithelial neoplasia cases and 3,436 controls using information from 7 Swedish registers. Kristiansen et al. [49] reported their results as follows:
Cases with penile intraepithelial neoplasia had increased odds ratios (ORs) for inflammatory skin diseases (14.7, 95% CI 6.5?33.4) including lichen planus (12.0, 95% CI 3.0?48.0), indicating lichen planus to be an important risk factor.
Increased ORs were also noted for diseases of the prepuce (4.0, 95% CI 2.2?7.4), immunosuppressive drugs (5.0, 95% CI 2.5?9.8), penile surgical procedures (4.8, 95% CI 2.2?10.8), balanitis (9.2, 95% CI 5.0?16.8), genital warts (9.9, 95% CI 4.3?22.7) and organ transplantation (7.0, 95% CI 2.4?20.8).
The study had revealed important risk factors for penile intraepithelial neoplasia, providing knowledge that can help prevent the development of penile cancer.
Kristiansen et al. [50] analysed the incidence, treatment strategies and complications associated with penile intraepithelial neoplasia (PeIN) in Sweden over a period of 20 years. Withregard to the materialsand methods of their study, Kristiansen et al. [50] reported that data on PeIN from the Swedish National Penile Cancer Register were analysed regarding treatment in relation to age, size of the PeIN lesion, localization of the PeIN lesion and complications using chi-squared tests and logistic regression. They calculated the incidence of PeIN and age-standardized according to the European Standard population. Kristiansen et al. [50] summarized the results as follows:
Between 2000 and 2019 a total of 1113 PeIN cases were reported. The age-standardized incidence of PeIN was found to be 1.40 per 100 000 men (95% confidence interval [CI] 1.32-1.49).
An increase in incidence over time was noted, with a standardized incidence rate of 2.37 (95% CI 1.56-3.70) in 2019 in comparison with the baseline year, 2000.
Surgical or topical treatments were provided in 75.0% and 14.6% of cases, respectively.
The complication rate was higher in laser surgery (12.1%, 7/58) when compared to local surgery (4.6%, 16/348; P = 0.03) with an age-adjusted odds ratio (OR) of 2.82 (95% CI 1.10-7.19; P = 0.03).
Local surgery was found to be more common than laser surgery in the preceding 5 years in comparison with the first 5 years of the study period: OR 5.75 (95% CI 2.94-11.27).
Treatments with imiquimod and topical 5-fluorouracil (5-FU) were more commonly undertaken than destructive methods including: photodynamic therapy, cryotherapy, curettage and electrocautery in the preceding 5 years compared to the first 5 years: OR 9.48 (95% CI 2.29-39.24).
Kristiansen et al. [50] made the ensuing conclusions:
A twofold increase in the age-standardized incidence of PeIN was noted in Sweden over 20 years.
Complications were noted to be three times more common in laser surgery in comparison with local surgery.
Changes in treatment had shown an increase of treatment strategies such as local surgery and treatment with imiquimod and topical 5-FU over time.
Conclusions
Penile Intraepithelial neoplasia (PeIN) is regarded as the putative histology precursor of penile squamous cell carcinoma.
PeIN has been classified into HPV-associated and HPV-independent (differentiated) (dPeIN).
While HPV-associated PeIN had been linked to the oncogenic effect of human papillomavirus (HPV), the HPV-independent pathway is stated to driven by chronic inflammatory conditions.
The aforementioned two biological pathways had been iterated to be associated with distinct histopathologic features.
The commonest morphology patterns of HPV-associated PeIN do include: basaloid, warty, and mixed PeIN.
DPeIN is stated to be the morphology expression of HPV-independent PeIN.
It had been pointed out that the 2016 and 2022 WHO classification had endorsed a dual pathogenic pathway of penile carcinogenesis, including: HPV-associated and HPV-independent. Within this classification, there are three main sub-types of HPV-associated PeIN, including: basaloid, warty, and mixed, and one main HPV-independent subtype,
dPeIN. HPV16 is the commonest genotype which had been detected within HPV-related PeIN, and most frequently in the basaloid subtype, while variable genotypes do characterize warty PeIN, which shows a diverse genotypic
It is important for all clinicians to update their knowledge about the manifestations, diagnosis, management as well as outcome of PeINs following their treatment as well as to follow-up carefully all cases of PeINs that are treated.
A global multi-centre treatment trial for PeINs would be strongly recommended in order to ascertain the best treatment options that would help improve upon the long-term outcome of all cases of PeINs.
Conflict Of Interest – Nil
Acknowledgements
Acknowledgements to Frontiers in Surgery for granting permission for reproduction of figures and contents of their journal article under the Creative Commons Attribution Licence; which allows reproduction of figures and contents of the Journal article provided the original source is cited and credited; which in this case is highly educative.
References
Huang K, Lu S, Wang Y, Tu X. (2021). Case Report: Treatment of Penile Intraepithelial Neoplasia in an Asian Male with Reconstructive Plastic Surgery. Front Surg. Jun 28; 8: 667417. View
at Publisher |
View
at Google Scholar
Bowen JT. Centennial paper. May (1912). (J Cutan Dis Syph 1912; 30:241-255). Precancerous dermatoses: a study of two cases of chronic atypical epithelial proliferation. By John T. Bowen, M.D., Boston. Arch Dermatol. 1983 Mar;119(3):243-60. PMID: 6297414. View
at Publisher |
View
at Google Scholar
Kallini JR, Hamed N, Khachemoune A. (2014). Squamous cell carcinoma of the skin: epidemiology, classification, management, and novel trends. Int J Dermatol. 2015 Feb;54(2):130-140. View
at Publisher |
View
at Google Scholar
Omori Y, Tanito K, Ito K, Ishiji T, Saeki H. (2014). Bowen's carcinoma of the penis with sebaceous differentiation associated with human papillomavirus type 16. Int J Dermatol. Nov;53(11): e531-532. View
at Publisher |
View
at Google Scholar
Sanchez DF, Cubilla AL. (2023). Penile intraepithelial neoplasia (PeIN). PathologyOutlines.com website. PeIN.html. Accessed November 2nd. View
at Publisher |
View
at Google Scholar
Rubin MA, Kleter B, Zhou M, Ayala G, Cubilla AL, (2001). Detection and typing of human papillomavirus DNA in penile carcinoma: evidence for multiple independent pathways of penile carcinogenesis. Am J Pathol. Oct;159(4):1211-1218. View
at Publisher |
View
at Google Scholar
Sanchez DF, Cañete S, Fernández-Nestosa MJ, Lezcano C, Rodríguez I,et all., (2015). . HPV- and non-HPV-related subtypes of penile squamous cell carcinoma (SCC): Morphological features and differential diagnosis according to the new WHO classification (2015). Semin Diagn Pathol. May;32(3):198-221. View
at Publisher |
View
at Google Scholar
Epstein Jonathan I, Magi-Galluzi C, Zhou M, Cubilla L A. (2020). Tumors of the Prostate Gland, Seminal Vesicles, Scrotum, (AFIP Atlas of Tumor and Non - Tumor Pathology, Series 5,) Hard Cover – October 30. View
at Publisher |
View
at Google Scholar
Hoekstra RJ, Trip EJ, Ten Kate FJ, Horenblas S, (2019). Lock MT. Penile intraepithelial neoplasia: Nomenclature, incidence and progression to malignancy in the Netherlands. Int J Urol. Mar;26(3):353-357. View
at Publisher |
View
at Google Scholar
Soskin A, Vieillefond A, Carlotti A, Plantier F, Chaux A, et all., (2012). Warty/basaloid penile intraepithelial neoplasia is more prevalent than differentiated penile intraepithelial neoplasia in nonendemic regions for penile cancer when compared with endemic areas: a comparative study between pathologic series from Paris and Paraguay. Hum Pathol. Feb;43(2):190-196. View
at Publisher |
View
at Google Scholar
Chaux A, Velazquez EF, Amin A, Soskin A, Pfannl R, et all., (2012). Distribution and characterization of subtypes of penile intraepithelial neoplasia and their association with invasive carcinomas: a pathological study of 139 lesions in 121 patients. Hum Pathol. Jul;43(7):1020-1027. View
at Publisher |
View
at Google Scholar
Straub Hogan MM, Spieker AJ, Orejudos M, Gheit T, Herfs M, et all., (2022). Pathological characterization and clinical outcome of penile intraepithelial neoplasia variants: a North American series. Mod Pathol. Aug;35(8):1101-1109. View
at Publisher |
View
at Google Scholar
Oertell J, Caballero C, Iglesias M, Chaux A, Amat L, et all., (2011). Histopathology. Differentiated precursor lesions and low-grade variants of squamous cell carcinomas are frequent findings in foreskins of patients from a region of high penile cancer incidence. May;58(6):925-933. View
at Publisher |
View
at Google Scholar
Hoekstra RJ, Trip EJ, Ten Kate FJ, Horenblas S, Lock MT. (2019). Penile intraepithelial neoplasia: Nomenclature, incidence and progression to malignancy in the Netherlands. Int J Urol. Mar;26(3):353-357. View
at Publisher |
View
at Google Scholar
Fernández-Nestosa MJ, Guimerà N, Sanchez DF, Cañete-Portillo S, et all., (2017). Human Papillomavirus (HPV) Genotypes in Condylomas, Intraepithelial Neoplasia, and Invasive Carcinoma of the Penis Using Laser Capture Microdissection (LCM)-PCR: A Study of 191 Lesions in 43 Patients. Am J Surg Pathol. Jun;41(6):820-832. View
at Publisher |
View
at Google Scholar
Epstein in: Moch H, Cubilla AL, Humphrey PA, Reuter VE, (2016). The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs-Part A: Renal, Penile, and Testicular Tumours. Eur Urol. Jul;70(1):93-105. View
at Publisher |
View
at Google Scholar
Olesen TB, Sand FL, Rasmussen CL, Albieri V, Toft BG, et all., (2018). Prevalence of human papillomavirus DNA and p16INK4a in penile cancer and penile intraepithelial neoplasia: a systematic review and meta-analysis. Lancet Oncol. 2019 Jan;20(1):145-158. View
at Publisher |
View
at Google Scholar
Fernández-Nestosa MJ, Guimerà N, Sanchez DF, Cañete-Portillo S, Lobatti A, (2019). Velazquez EF, Jenkins D, Quint W, Cubilla AL. Comparison of Human Papillomavirus Genotypes in Penile Intraepithelial Neoplasia and Associated Lesions: LCM-PCR Study of 87 Lesions in 8 Patients. Int J Surg Pathol. 2020 May;28(3):265-272. View
at Publisher |
View
at Google Scholar
Sirera G, Videla S, Piñol M, Cañadas MP, Llatjos M, et all., (2006). High prevalence of human papillomavirus infection in the anus, penis and mouth in HIV-positive men. AIDS. May 12;20(8):1201-1204. View
at Publisher |
View
at Google Scholar
Straub Hogan MM, Spieker AJ, Orejudos M, Gheit T, Herfs M, et all., (2022). Pathological characterization and clinical outcome of penile intraepithelial neoplasia variants: a North American series. Mod Pathol. Aug;35(8):1101-1109. View
at Publisher |
View
at Google Scholar
Kristiansen S, Torbrand C, Svensson Å, Forslund O, Bjartling C. Incidence of penile intraepithelial neoplasia and treatment strategies in Sweden 2000-2019. BJU Int. 2022 Jun;129(6):752-759. View
at Publisher |
View
at Google Scholar
Corbishley CM, Tinwell B, Kaul A, Ayres B, Watkin NA. (2015). Glans resurfacing for precancerous and superficially invasive carcinomas of the glans penis: Pathological specimen handling and reporting. Semin Diagn Pathol. May;32(3):232-337. View
at Publisher |
View
at Google Scholar
Issa A, Sebro K, Kwok A, Janisch F, Grossmann Ncet all., (2022). Fankhauser CD. Treatment Options and Outcomes for Men with Penile Intraepithelial Neoplasia: A Systematic Review. Eur Urol Focus. May;8(3):829-832. View
at Publisher |
View
at Google Scholar
Chaux A, Pfannl R, Lloveras B, Alejo M, Clavero O. (2010). Distinctive association of p16INK4a overexpression with penile intraepithelial neoplasia depicting warty and/or basaloid features: a study of 141 cases evaluating a new nomenclature. Am J Surg Pathol. Mar;34(3):385-392. View
at Publisher |
View
at Google Scholar
Hansen JP, Drake AL, Walling HW. Bowen's Disease: a four-year retrospective review of epidemiology and treatment at a university center. Dermatol Surg. Jul;34(7):878-83. View
at Publisher |
View
at Google Scholar
Morton CA, Birnie AJ, Eedy DJ. (2014). British Association of Dermatologists' guidelines for the management of squamous cell carcinoma in situ (Bowen's disease) 2014. Br J Dermatol. Feb;170(2):245-260. View
at Publisher |
View
at Google Scholar
Hambly R, Mansoor N, Quinlan C, Shah Z, Lenane P, Ralph N, Moloney FJ. Topical photodynamic therapy for primary Bowen disease and basal cell carcinoma: optimizing patient selection. Br J Dermatol. 2017 Sep;177(3):e55-e57. View
at Publisher |
View
at Google Scholar
Morton C, Horn M, Leman J, Tack B, Bedane Cet all., (2006). Comparison of topical methyl aminolevulinate photodynamic therapy with cryotherapy or Fluorouracil for treatment of squamous cell carcinoma in situ: Results of a multicenter randomized trial. Arch Dermatol. Jun;142(6):729-735 View
at Publisher |
View
at Google Scholar
Sarmiento JM, Wolff BG, Burgart LJ, Frizelle FA, Ilstrup DM. (1997). Perianal Bowen's disease: associated tumors, human papillomavirus, surgery, and other controversies. Dis Colon Rectum. Aug;40(8):912-918. View
at Publisher |
View
at Google Scholar
Cañete-Portillo S, Sanchez DF, Fernández-Nestosa MJ, Piris A, Zarza P, et all., (2019). Continuous spatial sequences of lichen sclerosis, penile intraepithelial neoplasia, and invasive carcinomas: a study of 109 cases. International Journal of Surgical Pathology. Aug;27(5):477-482. View
at Publisher |
View
at Google Scholar
Chaux A, Pfannl R, Rodríguez IM, Barreto JE, Velazquez EF, et all., (2011). Distinctive immunohistochemical profile of penile intraepithelial lesions: a study of 74 cases. Am J Surg Pathol. Apr;35(4):553-562 View
at Publisher |
View
at Google Scholar
Canete-Portillo S, Velazquez EF, Kristiansen G, Egevad L, Grignon D, et all., (2020). Report From the International Society of Urological Pathology (ISUP) Consultation Conference on Molecular Pathology of Urogenital Cancers V: Recommendations on the Use of Immunohistochemical and Molecular Biomarkers in Penile Cancer. Am J Surg Pathol. Jul;44(7): e80-e86. View
at Publisher |
View
at Google Scholar
Velazquez EF, Chaux A, Cubilla AL. (2012). Histologic classification of penile intraepithelial neoplasia. Semin Diagn Pathol. May;29(2):96-102. View
at Publisher |
View
at Google Scholar
Fernández-Nestosa MJ, Clavero O, Sánchez DF, Giannico GA, Lobatti A,et all., (2023). Penile intraepithelial neoplasia: Distribution of subtypes, HPV genotypes and p16INK4a in 84 international cases. Hum Pathol. Jan; 131:1-8. View
at Publisher |
View
at Google Scholar
Sofía Canete-Portillo, Diego F. Sanchez, Antonio L. Cubilla, (2019). Pathology of Invasive and Intraepithelial Penile Neoplasia, European Urology Focus, 5(5): 713-717, ISSN 2405-4569, View
at Publisher |
View
at Google Scholar
Aynaud O, Ionesco M, Barrasso R. (1994). Penile intraepithelial neoplasia. Specific clinical features correlate with histologic and virologic findings. Cancer. Sep 15;74(6):1762-1767. View
at Publisher |
View
at Google Scholar
Porter WM, Francis N, Hawkins D, Dinneen M, Bunker CB. (2002). Penile intraepithelial neoplasia: clinical spectrum and treatment of 35 cases. Br J Dermatol. Dec;147(6):1159-1165. View
at Publisher |
View
at Google Scholar
da Costa Nunes JF, Pires S, Chade DC. (2020). Human papillomavirus vaccination and prevention of intraepithelial neoplasia and penile cancer. Current Opinion in Urology. Mar 1;30(2):208-212. View
at Publisher |
View
at Google Scholar
Markos AR. (2003). The management of penile intraepithelial neoplasia in genitourinary medicine. International Journal of STD & AIDS.14(5):314-319. View
at Publisher |
View
at Google Scholar
Kravvas G, Ge L, Ng J, Shim TN, Doiron PR, Watchorn R, Kentley J, et all., (2022). The management of penile intraepithelial neoplasia (PeIN): clinical and histological features and treatment of 345 patients and a review of the literature. Journal of Dermatological Treatment. Feb 17;33(2):1047-1062. View
at Publisher |
View
at Google Scholar
Deen K, Burdon‐Jones D. (2017). Imiquimod in the treatment of penile intraepithelial neoplasia: An update. Australasian Journal of Dermatology. May;58(2):86-92. View
at Publisher |
View
at Google Scholar
Baldur-Felskov B, Hannibal CG, Munk C, Kjaer SK. (2012). Increased incidence of penile cancer and high-grade penile intraepithelial neoplasia in Denmark 1978-2008: a nationwide population-based study. Cancer Causes Control. Feb;23(2):273-280. View
at Publisher |
View
at Google Scholar
Gross G, Pfister H. (2004). Role of human papillomavirus in penile cancer, penile intraepithelial squamous cell neoplasias and in genital warts. Med Microbiol Immunol. Feb;193(1):35-44. View
at Publisher |
View
at Google Scholar
Wikström A, Hedblad MA, Syrjänen S. (2012). Penile intraepithelial neoplasia: histopathological evaluation, HPV typing, clinical presentation and treatment. Journal of the European Academy of Dermatology and Venereology. Mar;26(3):325-330. View
at Publisher |
View
at Google Scholar
María José Fernández-Nestosa, Omar Clavero, Diego F. Sánchez, et all., (2023). Penile intraepithelial neoplasia: Distribution of subtypes, HPV genotypes and p16INK4a in 84 international cases, Human Pathology. 131: 1-8. View
at Publisher |
View
at Google Scholar
Guerrero J, Trias I, Veloza L, Del Pino M, Garcia A, et all., (2022). HPV-Negative penile intraepithelial neoplasia (PeIN) with basaloid features. The American Journal of Surgical Pathology. Aug;46(8):1071 - 1077. View
at Publisher |
View
at Google Scholar
Stojanović S, Vučković N, Vemić D. (2022). Penile Intraepithelial Neoplasia: Successful Treatment with Topical 5% Imiquimod Cream. Serbian Journal of Dermatology and Venereology;4(4):163-170. View
at Publisher |
View
at Google Scholar
Sabater-Marco, Vicente; Navalon-Verdejo, Pedro; Sabater-Abad, Vicente Javier EXTRAORDINARY CASE REPORT Balanitis Xerotica Obliterans Associated with Differentiated Penile Intraepithelial Neoplasia and “Bramble-Bush” Elastic Fibers Accumulation: A Finding Not Specific for Penicillamine Intake. The American Journal of Dermatopathology View
at Publisher |
View
at Google Scholar
Kristiansen, S., Svensson, Åke, Drevin, L., Forslund, O., & Bjartling, C. et all., (2018). Risk Factors for Penile Intraepithelial Neoplasia: A Population-based Register Study in Sweden. 2000-2012 Acta Dermato-Venereologica, 99(3), 315–320. View
at Publisher |
View
at Google Scholar
Kristiansen S, Torbrand C, Svensson Å, Forslund O, Bjartling C. (2022). Incidence of penile intraepithelial neoplasia and treatment strategies in Sweden 2000-2019. BJU Int. Jun;129(6):752-759. View
at Publisher |
View
at Google Scholar
Dear Editorial Team,
Clinical Medical Reviews and Reports.
My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal.
Best wishes from,
Elena Popa.
Dr Elena Popa
It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.
Dr Nikolaos Andreas Chrysanthakopoulos
Dear Grace Pierce,
Editorial Coordinator of Journal of Clinical Research and Reports,
Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future.
Best wishes from,
Robert W. McGee
Robert W McGee
Dear Grace Pierce,
Editorial Coordinator of Journal of Clinical Research and Reports,
Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal.
Best wishes from,
DR Aibing Rao, Head of R&D
Aibing Rao
I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.
Kashani Mehdi
Dear Mercy Grace,
Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences,
We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage.
We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences!
Best wishes from,
Alla Konstantinovna Politova,