
Research | DOI: https://doi.org/10.31579/2642-973X/018
1 Internal Medicine II and Stroke Unit, San Giuseppe Hospital, Empoli, Italy.
2 Neurology, San Giuseppe Hospital, Empoli, Italy.
3 Cardiology, San Giuseppe Hospital, Empoli, Italy.
*Corresponding Author: Luca Masotti, 1Internal Medicine II and Stroke Unit, San Giuseppe Hospital, Empoli, Italy
Citation: Luca Masotti. (2022). Predicting Paroxysmal Atrial Fibrillation in Patients with Embolic Stroke of Undetermined Source (Esus) In the Real-World Practice: Comparison Between Brown-Af, As5f And Cha2ds2-Vasc Scores. Brain and Neurological Disorders. 5(3); DOI:10.31579/2642-973X/018
Copyright: © 2022, Luca Masotti, this is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 25 February 2022 | Accepted: 30 May 2022 | Published: 23 June 2022
Keywords: ESUS; stroke; atrial fibrillation; score; ECG monitoring
Introduction: Searching paroxysmal atrial fibrillation (PAF) is fundamental and strongly recommended in patients suffering from cryptogenic stroke or embolic stroke of undetermined source (ESUS). In the latest years some prediction scores for detecting post-stroke PAF have been proposed, such as Brown-AF and AS5F. However, external validations lack. The aim of the present study was to analyze the predictive power of AS5F and Brown-AF scores and compare them with the CHA2DS2-VASc score.
Materials and Methods
We analyzed demographic, clinical, trans-thoracic echocardiography and brain computer tomography characteristics of patients with ESUS undergone to two weeks external ECG monitoring after hospital discharge. PAF was considered detected when any evidence of AF and/or atrial flutter occurred at monitoring. For each patient we calculated the Brown-AF, AS5F and CHA2DS2-VASc scores and we analyzed and compared their predictive power by using area under the Receiver Operating Curve (AUROC).
Results: Eighty-two consecutive ESUS patients with mean age ± SD 72 ± 10 years were the study population. Overall, PAF was detected in 43.9% of patients. PAF detection increased from 18.75% of patients with Brown ESUS-AF score 0 to 54.3% of patients with Brown ESUS-AF score ≥ 2. PAF was detected in 37.2% of patients with AS5F < 67.5 and 51.2% of patients with AS5F score ≥ 67.5. AUROC of Brown ESUS-AF score in predicting AF detection was 0.642 (95% CI: 0.528-0.745), while AUROC of AS5F was 0.618 (95% CI: 0.504-0.723)(p=0.6872). No difference between predictive power of Brown ESUS-AF and AS5F scores with CHA2DS2-VASc (AUROC 0.671, 95% CI: 0.559-0.771) was found.
Conclusion:
Both Brown ESUS-AF and AS5F scores could be used as a screening tool for selecting ESUS patients requiring prolonged ECG monitoring aimed to detect PAF. However, in our study their predictive power was quite low and not superior to that of CHA2DS2-VASc score.
Occult paroxysmal atrial fibrillation (PAF) represents one of the main causes of embolic stroke of undetermined source (ESUS). Therefore, searching PAF is fundamental in the diagnostic work-up of ESUS and strongly recommended by international experts who suggest that patients with ESUS should have continuous electrocardiogram (ECG) after stroke for at least 72 hours [1]. In the latest years, some prediction score has been proposed to detect post-stroke PAF and better identify patients requiring prolonged ECG monitoring. In 2018, Ricci B. et al proposed a new simple score named Brown ESUS-AF score aimed at predicting PAF detection on prolonged ECG monitoring in post ESUS outpatients [2]. The protocol by Ricci B. and colleagues consisted of a 30-day external ECG monitoring followed by an implantable device if the first monitoring was negative. PAF was considered detected when any evidence of PAF or atrial flutter including brief episodes occurred at ECG monitoring. Age ≥ 75 years (2 points), age 65-74 years (1 point), moderate-severe left atrial enlargement (2 points) were the variables they found as independent predictors of AF detection. The predictive power of the Brown ESUS-AF score was good with an area under the receiver operating characteristic curve (AUROC) of 0.725. PAF detection increased from 4.2% in patients with Brown ESUS-AF score of 0 to 55.6% in patients with a score of 4. In a study comparing 68 patients with first ever AF with 123 patients with cryptogenic stroke, Muscarine A et al found an AUROC of 0.70 (95% CI: 0.62-0.78) for the Brown ESUS-AF score [3]. Recently Mendez B. et al. showed that the Brown ESUS-AF score is also a good prognosticator of stroke recurrence in ESUS patients [4]. In 2019 Uphauls T et al. proposed the AS5F score for predicting PAF in cryptogenic stroke [5]. Age (0.76 x year) and NIHSS ( 5 9 points; > 5 21 points) were the variables included. Cut-off 67.5 defines low and high risk of PAF. The Authors found an AUROC of 0.780. The protocol of AS5F foresees a 72 hours long ECG monitoring [5]. Accordingly, Ghoshal S. et al confirmed an AUROC of AS5F score of 0.751 (95% CI 0.724-0.778) in more than one thousands of stroke patients. In this study the Authors found that combining AS5F with an automated software analyzing the first hour of 72-hours ECG monitoring could significantly increase the predictive power of AS5F reaching an AUROC of 0.789, 95% CI 0.763-0.814; difference between the AUC P = 0.022 [6].
Despite both scores are very simple and interesting tools, external validations lack. Thus, the aim of our study was to analyze the predictive power of Brown ESUS-AF and AS5F scores in a cohort of real-world patients suffering from ESUS and compare them with CHA2DS2-VASc score.
Study population encompasses 82 consecutive ESUS patients (48 females) defined according to standardized criteria [7], admitted to our Stroke Unit and undergone to 15-day external ECG monitoring by using an event recorder (Spider Flash-tTM, Sorin Group) after hospital discharge. For all the patients demographic characteristics (age, sex), modified Rankin scale (mRS) at hospital discharge, risk factors for AF, CHA2DS2-VASc score, Brown-AF score, AS5F score, National Institute of Health Stroke Scale (NIHSS) at stroke onset, brain infarct size (<2>2.5 cm), location (cortical, cortical-subcortical, subcortical, supra- or sub-tentorial) and number (single or multiple) of the ischemic lesions, left atrium size (with left atrial enlargement, defined as diameter ≥40 mm or area ≥20 cm2), were analyzed. We compared patients whose PAF was detected with those whose PAF was not detected.
For statistical analysis continuous variables were reported as mean ± standard deviation (SD) or as median and interquartile range (IQR) as appropriate. Categorical variables were analyzed using the χ2 test and Fisher's exact test when appropriate. To evaluate the predictive power of CHA2DS2-VASc, Brown-AF and AS5F scores, the AUROC of each score was calculated. A p value of less than 0.05 was considered statistically significant. All analyses were performed using MEDCALC statistical software (Medal Software Ltd, Acacialaan 22, B-8400 Ostend, Belgium).
General characteristics of patients are shown in Table 1.
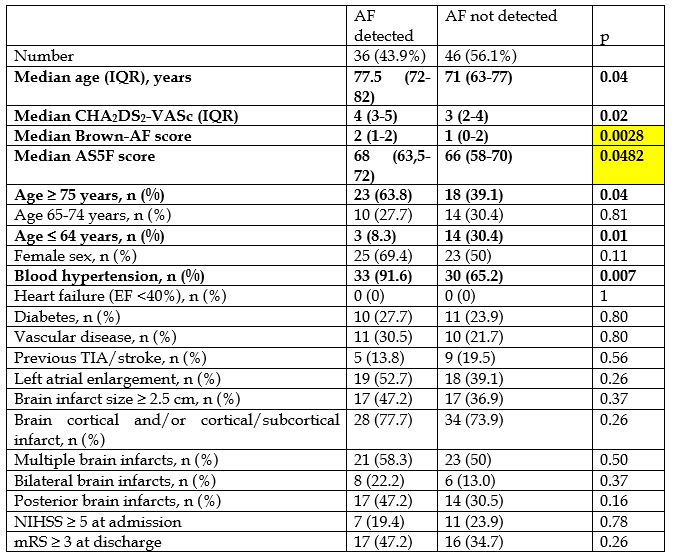
Mean age ± SD was 72 ± 10 years. Fourty-one patients (50%) were 75 years old and older, 24 (29.3%) were 65-74 years old, and 37 patients (45.1%) had left atrial enlargement defined as left atrial diameter > 40 mm or left atrial area > 20 cm2. PAF was detected in 36 patients (43.9%). Median CHA2DS2-VASc, Brown-AF and AS5F scores in patients with PAF detection were significantly higher compared with patients without PAF detection. Distribution of Brown-AF, AS5F and CHA2DS2-VASc scores are shown in
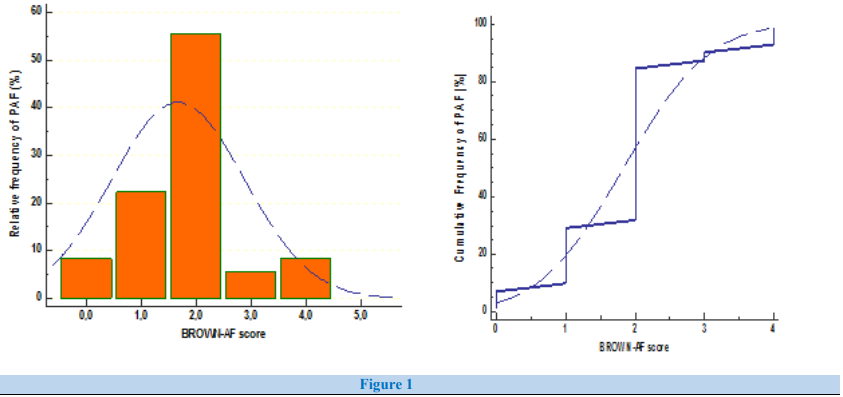

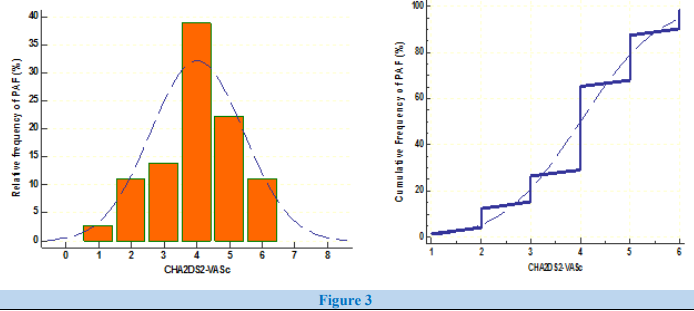
Figure 1-3: PAF detection increased from 18.75% in patients with Brown ESUS-AF score 0 to 54.3% in patients with Brown ESUS-AF score ≥ 2. PAF was detected in 37.2% of patients with AS5F < 67>
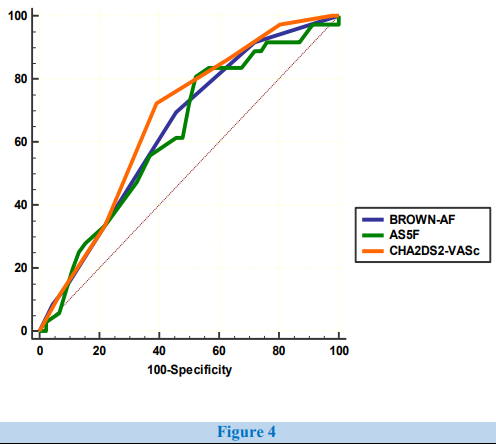
The AUROC of Brown ESUS-AF score in predicting AF detection was 0.642 (95% CI: 0.528-0.745, specificity 54.3%, sensitivity 69.4% for Brown ESUS-AF score > 1), while AUROC of AS5F was 0.618 (95% CI: 0.504-0.723, specificity 43.4%, sensitivity 80.5% for AS5F score > 62) (p=0.6872). No difference between predictive power of Brown ESUS-AF score and AS5F score with CHA2DS2-VASc score (AUROC 0.671, 95% CI: 0.559-0.771, specificity 60.8%, sensitivity 72.2% for CHA2DS2-VASc > 3)) was found (Table2, Figure 4).
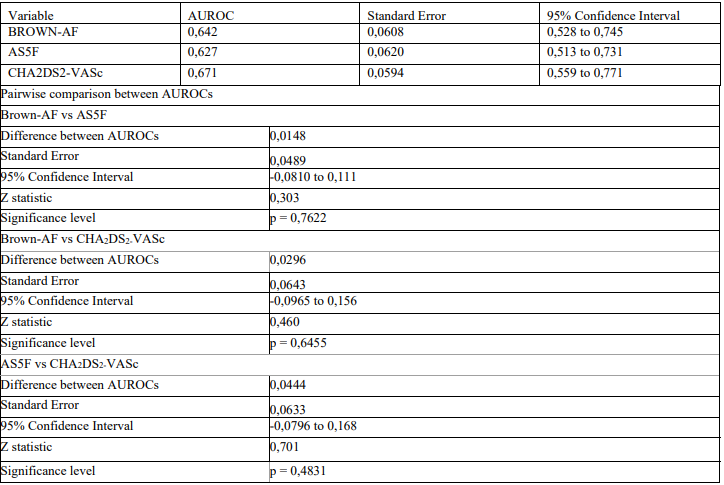
Table 2: Comparison between scores
Identifyng predictors of PAF detection in post ESUS patients is of the main importance to choose the appropriate treatment and reduce the risk of stroke recurrence. Systematic reviews showed that the rate of stroke recurrence in ESUS patients is 4.5% [8]. Randomized clinical trials found no advantage in the use of direct oral anticoagulants compared with antiplatelets in ESUS patients for preventing stroke recurrence (9,10), while in AF-related strokes direct oral anticoagulants are now recognized as the first choice in secondary prevention due to the best efficacy/safety profile compared with vitamin K antagonists or antiplatelets [11].
In the latest years, scores for predicting post-stroke PAF in cryptogenic and ESUS patients have been proposed, but external validations lack [2,5,12-15]. Therefore, we performed the present study aimed to analyzed retrospectively the predictive power of some of the proposed scores and compared them with CHA2DS2-VASc score which is a score mainly used for predicting stroke and/or systemic embolism in patients with AF. We were able to analyze performance of Brown-AF and AS5F scores. Our study confirms that the Brown ESUS-AF score and AS5F could be used as screening tools for identifying PAF in ESUS patients confirming that these scores may be useful to select patients with priority for searching PAF by prolonged ECG monitoring. However, in our study population, both scores showed a quite low predictive power for PAF detection and not different when compared with that of the most widespread CHA2DS2-VASc score.
We recognized that our study has limitations, mainly due to its retrospective design and difference in length of ECG monitoring (two weeks in our study while it was one month in the study of Ricci B. et al and 72 hours in the study of Uphauls T. et al) [2,5].
Brown ESUS-AF and AS5F scores could be used as screening tools for selecting ESUS patients requiring prolonged ECG monitoring aimed to detect PAF. However, in our study both Brown ESUS-AF than AS5F scores seems to bring no advantage compared with CHA2DS2-VASc score as PAF prognosticator. Further evidence is warranted.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
