
Research Article | DOI: https://doi.org/10.31579/2641-0419/235
1 Department of Medicine, McGovern Medical School, University of Texas Houston.
*Corresponding Author: Pushan Jani, MD Assistant Professor of Medicine Pulmonary and Sleep Medicine McGovern Medical School, University of Texas Houston 6410 Fannin Street #1014 Houston, TX 77030.
Citation: Alexis Preston, Bindu Akkanti, Prakash Balan, Biswajit Kar, Igor E. Gregoric.et all (2022). Pre Transcatheter-Aortic Valve Replacement CT Scans: An Opportunity Missed to Detect Lung Cancer?. J. Clinical Cardiology and Cardiovascular Interventions, 5(5); DOI:10.31579/2641-0419/235
Copyright: © 2022 Pushan Jani., This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 01 December 2021 | Accepted: 25 February 2022 | Published: 10 March 2022
Keywords: nodule; ct scan; pulmonary; tavr
Background
This study aimed to investigate the incidental pulmonary nodule findings in Trans Catheter Aortic Valve Replacements (TAVR) patients undergoing preoperative computed tomography (CT) scan workup and occurrence of appropriate CT scan follow-up for nodule management in eligible patients.
Methods
A single-center TAVR data was retrospectively analyzed between 2011 and 2017 to identify the incidental pulmonary nodule finding on preop chest CT scans routinely performed as part of TAVR workup. The primary study objective was to determine incidence of pulmonary nodule and to investigate occurrence of appropriate diagnostic follow-up and cancer in patients eligible for follow-up CT scan based on Fleischner criteria.
Results
Of the 899 patients (mean age 79 years, 50% male), 220 patients had finding of pulmonary nodule (117 multiple and 103 solitary) and 93 were eligible for a follow-up CT scan based on the Fleischner criteria. Of the 93 follow-up eligible patients, 35 (38%) had repeat CT scan and 58 (62%) had no follow-up CT scan. The lung cancer occurrence in no CT scan, CT within timeframe, CT early and CT delayed groups was 1 each (2% v. 14% v. 7% v. 7%. p=0.3).
Conclusion
This single center report shows that the pre TAVR CT scans serve as an excellent lung cancer screening opportunity, however most patients (92%) do not have an appropriate follow-up CT scan for the diagnosis and management of the nodules. A larger observational study using the Medicare database may shed more light on real-world practice of pulmonary nodule diagnostic management in TAVR patients.
CT – Computerized Tomography
CTA – Computerized Tomography Angiography
TAVR – Trans-Catheter Aortic Valve Replacement
In the United States over 70,000 transcatheter aortic valve replacement (TAVR) procedures are performed annually, primarily in patients aged over 65 years (93%) [1]. All patients undergoing the TAVR have a chest CT Angio (CTA) done prior to the procedure to determine aortic annulus size. Pulmonary nodule could be an incidental finding in these patients which may warrant further follow-up based on Fleischner criteria, however it is unclear how many of these eligible patients with pulmonary nodules receive follow-up management per guidelines [2]. We aimed to identify incidence of pulmonary nodules in patients receiving pre TAVR CTA and determine appropriate subsequent diagnostic management and occurrence of cancer in these patients.
After IRB approval, a single-center TAVR data was retrospectively analyzed between 2011 and 2017 to identify the incidental pulmonary nodule finding on preop chest CTA routinely performed as part of TAVR workup. Other chronic lung disease conditions were also evaluated. We further evaluated patients with pulmonary nodule to ascertain if the eligible patients received appropriate follow-up CT scans to identify any changes in the pulmonary nodules and its applicable management
The primary study objective was to determine incidence of pulmonary nodule in cohort of patients undergoing TAVR and to identify occurrence of appropriate diagnostic follow-up and cancer in patients with presence of pulmonary nodules. Basic descriptive statistics were used to analyze the data. The cohort was divided in 4 groups based on occurrence of follow-up CT scan based on Fleischner criteria.
During the study period, 899 patients (mean age 79 years, 50% male) underwent TAVR procedure and preop CTA. The occurrence of pulmonary nodule was in 220 (24%) of patients. Of all patients, 263 had pleural effusion (186 bilateral, 37 left, 40 right), 154 had emphysema, 43 had pulmonary fibrosis, and 29 had interstitial lung disease.
Of the 220 pulmonary nodule patients, 117 had multiple (49 were 6mm and 19 not available) and 103 had solitary (48 were 8mm, 11 not available) nodules. Of the 49 patients with multiple nodules >6mm, 21 had follow-up CT performed, of which only 2 had between 90-180 days (recommended timeframe), 9 had prior to 90, and 10 had after 180 days. In the 16 patients with solitary nodule sized 6-8mm, 4 had repeat CTA, 2 within 6-12 months, (recommended timeframe) 1 prior, and 1 after the recommended timeframe. In the 28 patients with solitary nodule >8mm, 10 had repeat CT scans, 3 between 3-6months (recommended timeframe), 3 after 6months, and 4 prior to 3 months (Figure 1).
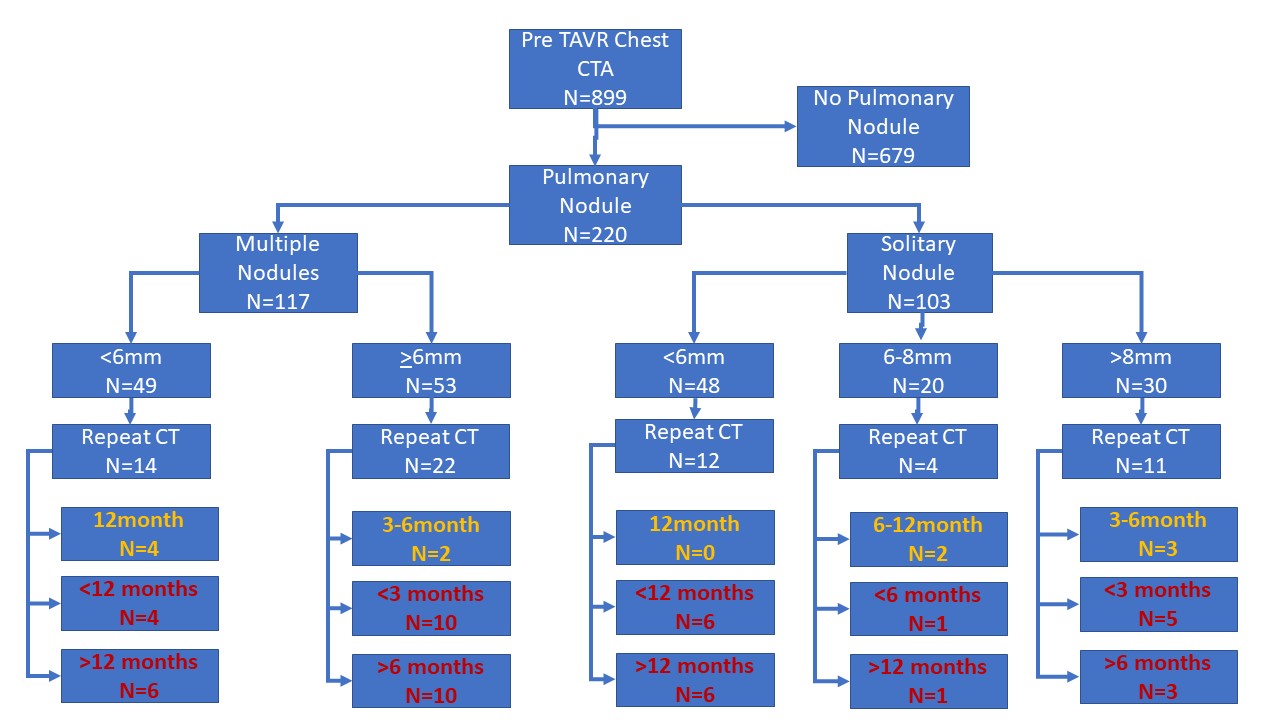
Of the 220 pulmonary nodule patients, 93 were eligible for a repeat CT scan based on the Fleischner criteria (>6mm nodule size for solitary and multiple). Of the 93 follow-up eligible patients 35 had repeat CT scan (7 within the timeframe of Fleischner criteria, 14 before and 14 after the recommended timeframe, Figure 1). Patients who received timely follow-up CT scans were more likely to be smokers, older and less likely to be African Americans (Table 1).
No CT Scan | CT in Time | CT early | CT delayed | p-value | |
Age | 82 (77-84) | 85 (73-87) | 79 (73-84) | 79 (68-84) | 0.4 |
Sex (1) | 50% (29) | 43% (7) | 31% (4) | 43% (6) | 0.6 |
Race (AA) | 5% (3) | 0 (0) | 15% (2) | 7% (1) | 0.5 |
Smoker | 7% (4) | 33% (2) | 23% (3) | 7% (1) | 0.1 |
Hypertension | 95% (56) | 86% (6) | 100% (13) | 86% (12) | 0.2 |
Diabetes | 47% (27) | 29% (2) | 15% (2) | 29% (4) | 0.1 |
Dialysis | 2% (1) | 0 (0) | 8% (1) | 14% (2) | 0.1 |
Home O2 | 2% (1) | 0 (0) | 15% (2) | 7% (1) | 0.1 |
Immunosupperession | 17% (10) | 29% (2) | 31% (4) | 14% (2) | 0.6 |
Surgical Risk Score | 9 (6-12) | 8 (4-9) | 10 (8-16) | 10 (8-11) | 0.2 |
Table 1: Differences in Patient Characteristics by Status of Follow-up CT scan
The lung cancer occurrence in no CT scan, CT within timeframe, CT early and CT delayed groups was 1 each (2% v. 14% v. 7% v. 7%. p=0.3). The occurrence of lung cancer in patients who had any follow-up CT scan was 9% vs. 2% in patients who had no follow-up CT scan (p=0.11). Twelve patients in the nodule size <6mm>
The incidence of pulmonary nodule in our single center cohort of patients undergoing TAVR was 24%, similar to the number (27%) reported on the low dose CT scan trial [3]. In patients with a nodule >6mm, we observed that over 92% patient did not have an appropriate follow-up CT scan. Of all eligible patients (n=93), only 37% (35) received a follow-up CT scan and only 8% (7) within the recommended timeframe. Whereas 62% patients had no CT scan, and the rest had prior (15%) to or later (15%) than the recommended timeframe. Of 93 CT scan eligible patients 4% (4) had diagnosis of lung cancer which is slightly higher (1.1%) than reported on low-dose CT trial [3]. Although patients with follow-up CT scan within appropriate timeframe had higher detection rate (14% vs. 2% v. 7% v. 7%) of lung cancer, it did not reach statistical significance.
Our observations highlight lack of recommended follow-up CT scans in patients with pulmonary nodules. However, several factors could be responsible for these findings, including advanced age (median age 79 years), presence of comorbidities (35% diabetics, >85% hypertensives, >25% immunosuppressed), disabilities and inadequate family support. This study also suggests the racial disparity in receipt of follow up scan where no African American patients received a CT scan in appropriate follow-up timeframe [4]. Our findings corroborate other reports published using single center data on prevalence of incidental pulmonary nodules in pre-TAVR CTA, however, no other studies have focused on occurrences of follow up diagnostic management of the nodules based on widely accepted Fleischner criteria [4-6]. With approval of TAVR in low-risk patients, younger patients are likely to receive TAVR and the preop CTA, thus, increasing the pool of patients on whom an indirect screening for lung cancer can be done in addition to the aortic stenosis evaluation.
Being a retrospective single center study, several limitations apply. A major limitation is lack of individual scenarios responsible for no follow-up CTA in over 60% patients. Also, patients receiving follow-up elsewhere could not be accounted for.
This single center report shows that the pre TAVR CTA serve as an excellent lung cancer screening opportunity, however most patients (92%) do not have an appropriate follow-up CT scan for the diagnosis and management of the nodules. This study may prompt more institutionalized and protocol-based approach for improving follow-up nodule workup. A larger study using the Medicare database may shed more light on real-world practice of pulmonary nodule diagnostic management in TAVR patients.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
