
Case Report | DOI: https://doi.org/10.31579/2690-8794/152
1Anaesthesiologist, Francistown Academic Hospital, Francistown, Botswana.
2 Medical Officer, Francistown Academic Hospital, Francistown, Botswana.
*Corresponding Author: Arop M. D. Kual. Anaesthesiologist, Francistown Academic Hospital, Francistown, Botswana
Citation: Arop M. D. Kual and Chetty Sarvashni. (2023), Practical Experiences in COVID-19 Clinical Management Case Reports. Clinical Medical Reviews and Reports. 5(1); DOI:10.31579/2690-8794/152
Copyright: © 2023, Mauro Luisetto. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 03 January 2023 | Accepted: 16 January 2023 | Published: 27 January 2023
Keywords: COVID-19; Sars Cov2; acute respiratory distress syndrome (ARDS); acute respiratory failure; acute kidney injury; liver damage; sepsis; muti-organ dysfunction
Coronavirus disease 2019 (COVID-19) is a respiratory tract infection caused by a newly emergent coronavirus, that was first recognized in Wuhan, China, in December 2019. Genetic sequencing of the virus suggests that it is a betacoronavirus closely linked to the SARS virus (1).
Most patients (80%) with COVID-19 develop only mild or uncomplicated illness, approximately 15% develop severe disease that requires hospitalization and oxygen therapy, and 5% require admission to an intensive care unit (1). In most severe cases, COVID-19 can be complicated by the acute respiratory distress syndrome (ARDS), sepsis and septic shock, multiorgan failure, including acute kidney injury and liver & cardiac injury. Older age and co-morbid disease have been reported as risk factors for death.
We report the clinical presentations, laboratory changes, imaging findings, diagnostic criteria, treatments, outcomes, prognostic factors, and risk factors of COVID-19 admitted to our facility.
COVID-19 is characterized by low-grade fever, cough, dyspnea, chest pain, headache, vomiting, diarrhea, lymphocytopenia, pulmonary infiltrates/opacities on chest X-ray and ground-glass opacities on chest CT scan.
A majority of patients have elevated levels of D-dimer, serum transaminases and laboratory findings consistent with sepsis-induced diffuse intravascular coagulation, suggesting a coagulopathic process, yet no prospective study has demonstrated the predictive nature of these markers for the occurrence of a thromboembolic event, only a higher risk for mortality.
Late in December 2019 and early in January 2020, reports of a very progressive pneumonia-like respiratory syndrome, starting in Wuhan, China, induced global health concerns. Soon after the onset of disease, it was found that the pathogen was a new member of the coronaviridae family, named SARS-CoV-2 which is now called 2019-n-CoV. The respiratory syndrome caused by 2019-n-CoV is called COVID-19.
COVID-19 is characterized by low-grade fever, cough, dyspnea, lymphopenia, and ground-glass opacities on chest CT scan. COVID-19 is a highly contagious disease, probably an aerosol born one, with human to human transmission capacity which has implicated many countries all around the world. In this review article, we systematically surveyed 16 patients from our facility to give a picture of the clinical presentations, laboratory changes, imaging findings, diagnostic criteria, treatments, outcomes, prognostic factors, and risk factors of COVID-19.
Case Presentations
Participants and sources of data
All patients admitted to Francistown Academic Hospital, Francistown, Botswana, between July 26 and August 5, 2021, diagnosed with COVID-19 and treated according to Botswana Interim Clinical Guidance for the Management of COVID-19, were enrolled.
The Institutional Review Board of Francistown Academic Hospital approved this report and waived the need for informed consent from individual patients, due to the retrospective chart review design and absence of identifying images or personal/ clinical details that could compromise anonymity.
Procedures
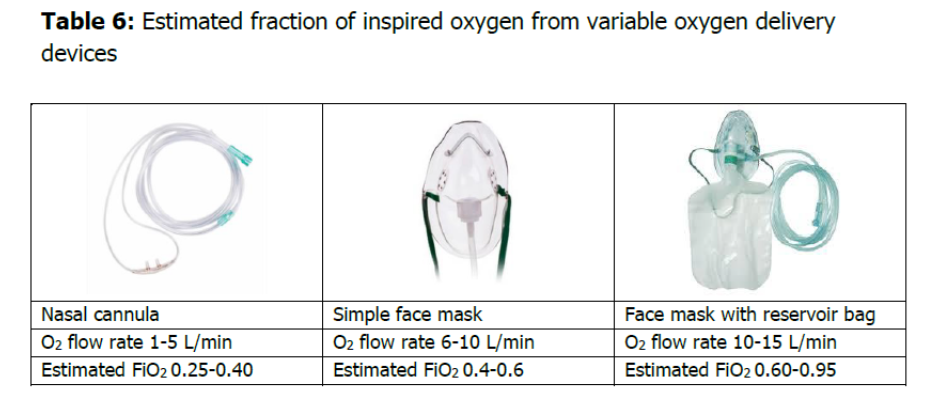
All patients received oxygen therapy at different flow rates according to Botswanan Interim Clinical Guidance for the management of patients with COVID-19 and according to the severity of the condition- Table 6.
All patients received standard treatment with azithromycin, co-amoxiclav, vitamin C, clexane and Tiophiline. Some selected patients received steroids.
Case 1
A 74 years old female was admitted with history of positive testing results for COVID-19 eleven days prior to the presentation. She reported symptoms of difficulty in breathing and cough. She was a known hypertensive on regular medications. Her oxygen saturation was 70% on oxygen.
Discussion
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Availability of data and materials
The datasets used and/or analysed in this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare that they have no competing interests.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
