
Research Article | DOI: https://doi.org/10.31579/2641-0419/421
University hospital MOHAMED VI, Department of Cardiology, Intensive care unit, Marrakesh, Morocco
*Corresponding Author: Noussaiba Malhabi, University hospital MOHAMED VI, Department of Cardiology, Intensive care unit, Marrakesh, Morocco.
Citation: Ztati Simohammed, Noussaiba Malhabi, Achraf, Abd Elkarim Ait Yahya, Mohammed EL Jamili, et al, (2024), Postural Orthostatic Tachycardia Syndrome: Experience of the Mohamed VI University Hospital, J Clinical Cardiology and Cardiovascular Interventions, 7(13); DOI: 10.31579/2641-0419/421
Copyright: © 2024, Noussaiba Malhabi. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 02 October 2024 | Accepted: 28 October 2024 | Published: 25 November 2024
Keywords: transcatheter intervention; mitraclip implantation; chordal entanglement; open heart surgery
Postural orthostatic tachycardia syndrome (POTS), one of the most prevalent autonomic disorders, presents with a variety of clinical symptoms, including postural tachycardia, dizziness, orthostatic intolerance, syncope, and exercise intolerance. It often develops following viral or bacterial infections.
Aims: we aim to study the Epidemiological, Diagnostic, Etiological Profile, and therapeutic approaches in Patients with Postural Orthostatic Tachycardia Syndrome (POTS) and to study the potential association with other dysautonomias in the same patients.
Materiel and methods: This is a prospective, descriptive, and analytical cross-sectional study. The patients were collected over one year, counting 53 patients included in our autonomic nervous unit diagnosed with POTS.
Results: we found an average age of 25 years, with more female then male, diagnostic wandering took from 3 months to 6 years as a cut-off in our study. Dysautonomias risqué factors found are COVID-19 infection and stressful lifestyle, main symptom is orthostatic intolerance. For our population the therapeutic approach was based on symptomatic treatment initially in particular; abundant drinks, lower limb muscle building, high salt diet, our results are that a check-up will be proposed in 6 months to see the evolution under treatment
Conclusions: Management of POTS focuses on educating patients and implementing non-pharmacological strategies to combat orthostatic intolerance, our aim is to improve the quality of life of our patients.
Postural Orthostatic Tachycardia Syndrome (POTS) is a condition of dysautonomia, specifically orthostatic intolerance. In this condition, a change from a lying-down position to an upright position causes an abnormally high increase in heart rate, known as tachycardia.(1)
Several studies show decreased cerebral blood flow due to reduced systolic and diastolic cerebral blood circulation velocities by 44% and 60%, respectively. POTS patients thus have difficulties in maintaining homeostasis when changing positions, such as moving from one chair to another. Many also experience these symptoms while lying down or without making any movement. The diagnosis is made using a tilt-table test.
The severity of symptoms varies among patients, with some being completely debilitated, preventing them from working. In the most severe cases, patients may become completely paralyzed. The most prominent symptom of POTS is an increase in heart rate within 5 to 12 minutes of transitioning from lying to upright. This increase is generally more than 30 beats per minute, and the heart rate of POTS patients often exceeds 120 beats per minute. This tachycardia response is sometimes associated with a drop in blood pressure.(1)
Study aims:
This is a prospective, descriptive, and analytical cross-sectional study. The patients were collected over one year, from August 2023 to August 2024.
The patients included in the study were referred from various departments of the university hospital center to the cardiology department for autonomic nervous system assessment or were collected during our general cardiology consultations. We included 53 patients.
The inclusion criteria were as follows:
(1) baseline sinus rhythm with no evidence of arrhythmia or cardiac disease,
(2) sustained heart rate increment of 30 beats/min or greater
in response to 10 minutes of head-up tilt, and
(3) symptoms of orthostatic intolerance such as light-headedness, weakness, palpitations, blurred vision, breathing difficulties,nausea, or headache developing on standing or after head-up tilt and resolving with recumbency. These symptoms had to be present for more than 3 months.
Exclusion criteria were as follows:
(1) orthostatic hypotension defined as a decline of 30 mm Hg or more in systolic blood pressure or 20 mm Hg or more in mean blood pressure within 3 minutes of standing or head-up tilt;
(2) pregnancy or lactation;
(3) presence of another cause of autonomic failure; or
(4) presence of failure of other organ system or systemic illness affecting autonomic function or the patient’s ability to cooperate (dementia, pheochromocytoma, congestive heart failure, hypertension, renal or hepatic disease, severe anemia, alcoholism, malignant neoplasm, diabetes, hypothyroidism, sympathectomy, or cerebrovascular accident).
(5) hypertension under treatment or not
An operating sheet filled out during the exploration of the autonomic nervous system collects Epidemiological, clinical and para-clinical data, details are as follows:
It includes identity, age, sex, phone number and health coverage
❖ Fasting blood sugar ≥ 1.26 g/l (7 mmol/l) on 2 occasions and/or
❖ Blood sugar ≥ 2 g/l (11.1 mmol/l) 2 hours after a meal and/or
❖ HbA1c ≥ 6.5%.
o HDL-cholesterol < 0>
o LDL-cholesterol > 1.6 g/l and adjusted according to cardiovascular risk
o Triglycerides > 1.5g/l
o A waist circumference > 80 cm in women and 94 cm in men
o A body mass index (BMI=weight/height2) > 30 kg/m²
o MI or sudden death before age 55 in the father or a 1st-degree relative of
male gender.
o MI or sudden death before age 65 in the mother or a 1st-degree relative of
female gender.
o Early stroke (<45>
neurological disease, obliterative arterial disease of the limbs, stroke, revascularized ischemic heart disease, renal failure, pregnancy, medication intake, etc.
The four functional signs namely: dyspnea, chest pain, syncope, palpitations; and other associated signs are sought.
The parameters sought are: heart rate, respiratory rate, weight, height, BMI, waist circumference, blood pressure measurement by an electronic blood pressure monitor
The dosage of hemoglobin, HBA1C, creatinine, glomerular filtration rate estimated by the MDRD formula, triglycerides, total cholesterol, HDL cholesterol, HDL cholesterol, LDL cholesterol, complete ionogram, blood vitamin D dosage.
The resting electrocardiogram is also performed then the cardiac echocardiography if indicated.
Assessment of the autonomic nervous system:
The cardiovascular dynamic tests for assessing the autonomic nervous system (ANS), five in total, were initially described by Ewing and Clarke and further detailed by Phillip Low. They were developed to study cardiovascular autonomic nervous system disturbances. These tests evaluate parasympathetic and sympathetic function, as well as the baroreflex arc. They involve measuring blood pressure (BP) and/or heart rate (HR).(5)
The patient was first placed in a quiet environment in the supine position on a tilt table. Blood pressure (BP) was monitored using a Dynamap (Critikon, 1846SXP) and heart rate (HR) was monitored using a display screen (LCD CS 503 E; Hellige, EK 512 E).
All tests are interspersed with rest periods of approximately five minutes, necessary to return BP and HR to baseline figures.
The diagnosis of Postural Orthostatic Tachycardia Syndrome (POTS) is primarily based on the gold standard technique, the head-up tilt table test. This test involves monitoring a patient's heart rate and blood pressure while transitioning from lying to an upright position. A non-invasive, beat-to-beat hemodynamic monitoring system is typically used to detect significant changes, such as an excessive increase in heart rate (usually 30 beats per minute or more within 5 minutes of standing) without a corresponding drop in blood pressure. This test is essential for confirming POTS and distinguishing it from other forms of orthostatic intolerance.
The deep breathing (DB) test is crucial for determining the vagal response (VR). It evaluates autonomic function by measuring heart rate (HR) changes in response to deep breathing. The test involves continuous HR measurement during a cycle of six deep inhalations/exhalations performed over one minute. Respiratory rate influences the RR interval. This test is crucial for assessing the vagal response. Respiratory sinus arrhythmia is physiological and depends on vagal activity: it decreases when lung receptors are stimulated by stretching.
The variability of the RR interval is studied via electrocardiographic (ECG) recording throughout the test at a speed of 25 mm/s, during both inspiration (RR max) and expiration (RR min).
The result is expressed as a percentage:
(Maximal RR - Minimal RR) / Minimal RR x 100
A value of 30% is considered normal. Below this, there is vagal deficiency, and above this, hyperactive vagal response. This percentage tends to be very high in younger individuals.
This test involves a manual contraction effort used to determine changes in blood pressure (BP) during static exertion. The patient performs maximal hand pressure using a dynamometer for 15 seconds (isometric contraction). Normally, muscle contraction leads to an increase in both heart rate (HR) and BP. The increase in sympathetic activity at the muscular level is dependent on both the intensity and duration of the effort. The rise in BP is secondary to an increase in cardiac output and peripheral resistance. The HR increase is initially due to a withdrawal of vagal inhibition followed by sympathetic activation. This test involves the patient applying maximal pressure using a dynamometer for 15 seconds.(6)
For the vagal response: The test measures HR response during the 15 seconds following maximal pressure using a dynamometer.
For peripheral α-sympathetic response: A pressure of 50% less than the maximal force, sustained for 3 minutes, allows evaluation and measurement of BP variation.
This test explores the small-caliber fibers of the sympathetic efferent pathway in the reflex arc. It is used to detect dysautonomia, particularly in diabetic neuropathies, and provides insight into peripheral autonomic dysfunction.
The test's response is assessed by measuring changes in BP or HR according to the following formula:
(BP (or HR) after stimulation - BP (or HR) before stimulation) / BP (or HR) before stimulation
The result is expressed as a percentage. A response equal to 10% is considered normal. Above 10% indicates hyperactivity, and below 10% suggests vagal or sympathetic deficiency.(7)
During this test, the subject is asked to perform a mental calculation: subtracting the number 7 sequentially from 200 until reaching zero. Research has shown that mental calculation can lead to cardiovascular overreactivity and alterations in baseline heart rate variability (8).
This test induces an increase in central sympathetic activity, with a decrease in blood flow to the extremities and an increase in blood pressure (BP) and heart rate (HR). It explores the sympathetic efferent pathways (9). The result is an increase in BP and HR due to central sympathetic activation (10).
Central sympathetic "α" and "β" activities are expressed by the variations in BP and HR, respectively, before and after stimulation, according to the following formula:
(BP (or HR) after stimulation - BP (or HR) before stimulation) / BP (or HR) before stimulation
The result is expressed as a percentage. Typically, a response equal to 10% is considered normal; above 10% indicates hyperactivity, and below 10% suggests sympathetic deficiency.
After 10 minutes of rest, the patient is asked to breathe at a rate of 2 cycles per second for 4 minutes, and then to breathe spontaneously and normally for an additional 5 minutes (11).
These tests stimulate the sympathetic autonomic nervous system (ANS). Moving from a resting position to a standing position triggers a series of physiological adaptation processes in normal subjects: large volumes of blood are displaced. This reduces venous return to the heart, causing a decrease of about 40% in stroke volume and blood pressure. Baroreceptors detect these changes and send signals to the cardiovascular center, which responds by stimulating sympathetic tone. Under physiological conditions, the moderate drop in aortic pressure is corrected within 30 seconds by activating baroreflex arcs, which originate from the carotid and aortic baroreceptors. This results in arterial vasoconstriction and tachycardia. (12)
Passive Orthostatic Testing (Tilt Test)
The patient is placed on a tilting table with foot support and is gradually inclined up to 80° for 10 to 15 minutes. The duration can be extended up to 30 to 40 minutes depending on the pathology being investigated (e.g., syncope) (13).
Heart rate (HR) and blood pressure (BP) are measured throughout the examination. The curves of their variations corresponding to normal values are based on the work of Coghlan (Azzouzi, 2010).
Grade 0: Normal results.
Grade I: Presence of the following signs:
Excessive oscillation of BP: amplitude varies by more than 20 mmHg on recording, indicating baroreceptor abnormalities.
Increase in HR ≥ 30 bpm that persists for at least 50% of the 5-minute recording or exceeds 120 bpm: Postural Orthostatic Tachycardia Syndrome (POTS).
Increase in Diastolic Blood Pressure (DBP) ≥ 10 mmHg for 50% of the recording: Orthostatic Hypertension (OH).
Grade II: Decrease in systolic BP > 20 mmHg during the first minute of the test followed by recovery: Orthostatic Hypertension.
Grade III: Maintenance of OH but asymptomatic.
Grade IV: Maintenance of OH with symptoms of orthostatic intolerance.
This test also involves stimulation of the sympathetic nervous system. During this test, the subject uses their muscles to stand up. Continuous monitoring of BP, beat by beat, requires systems adapted to detect sudden BP changes (14).
The examination protocol varies according to clinical protocols and operators: for most authors, if the supine phase is 10 to 20 minutes, the orthostatic phase lasts about 5 to 45 minutes. The test we commonly perform lasts an average of 10 minutes, It is stopped if the patient experiences symptoms such as dizziness, chest pain, cyanosis of the extremities, or a pre-syncopal state, or if there are significant increases or decreases in HR and BP (15).
BP and HR values are recorded. Clinical or parametric signs of OH, POTS, or syncope are sought (16).
A decrease in systolic BP of 20 mmHg and diastolic BP of 10 mmHg, with systolic BP below 90 mmHg maintained for at least five minutes (some reduce the duration to at least 3 minutes), is considered orthostatic hypotension (17).
An increase in HR of 30 beats or more for three minutes is considered Postural Orthostatic Tachycardia Syndrome (POTS)(5).
Quantitative data are expressed as a mean plus or minus standard deviation and compared by the student test. While the qualitative data are expressed in number and percentage and compared by the chi 2 test. Statistical analysis was performed using SPSS software version 2.0 for Windows.
Baseline characteristics :
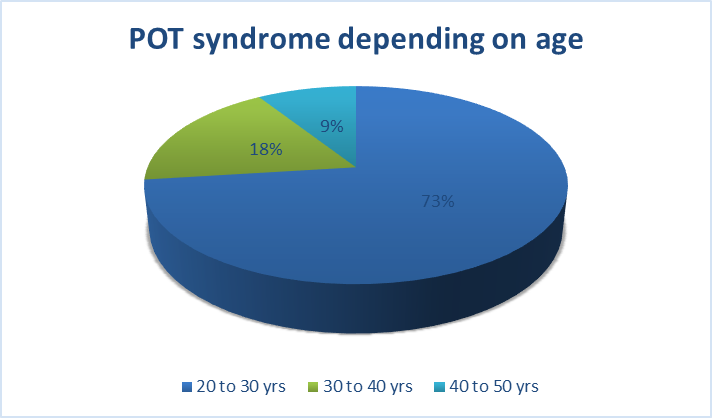
Age :
The age of our patients is between 20 and 50 years, with an average age of 25 years, the distribution of our population according to age is as follows
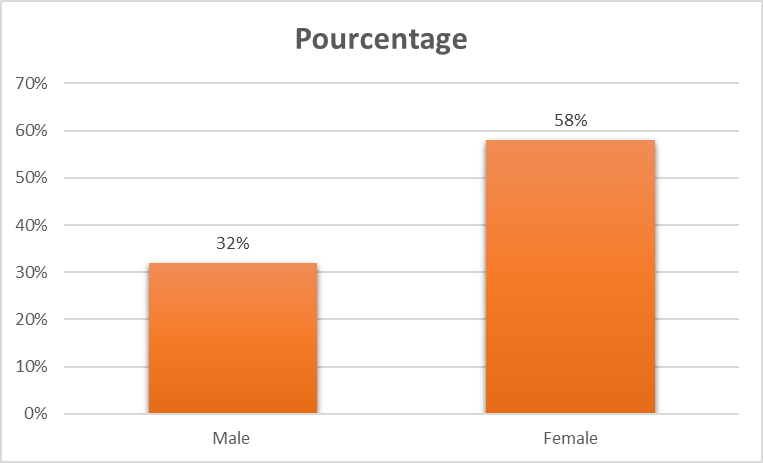
Sex:
We noted a clear female predominance before the age of 30 and a male predominance from the age of 45 years, in general we see a female predominance
Duration of symptoms:
Patients with POT syndrome had to wait an average of 3 years before their symptoms were related to their disease, diagnostic wandering took from 3 months to 6 years as a cut-off in our study.
Cardiovascular risk factors:
Regarding the cardiovascular risk factors encountered in our study: 30% of patients are smokers, 20% are diabetic, and 2 patients are obese.
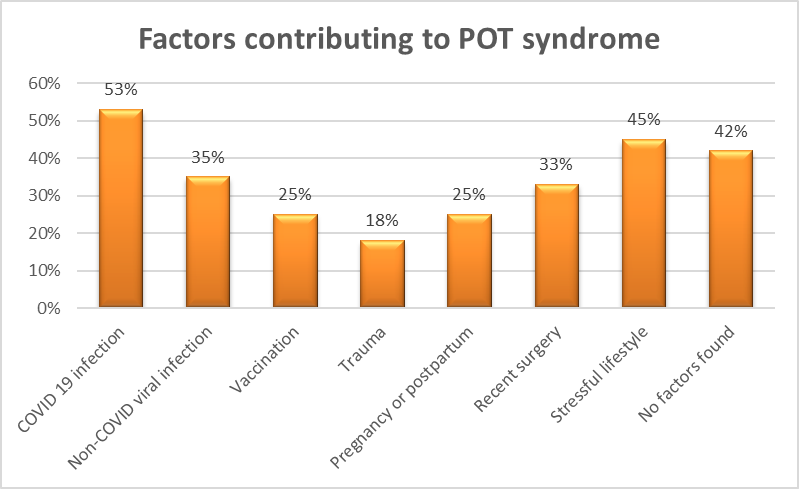
Factors contributing to dysautonomia:
Many factors contribute to POT syndrome according to many studies some of them are found in our study
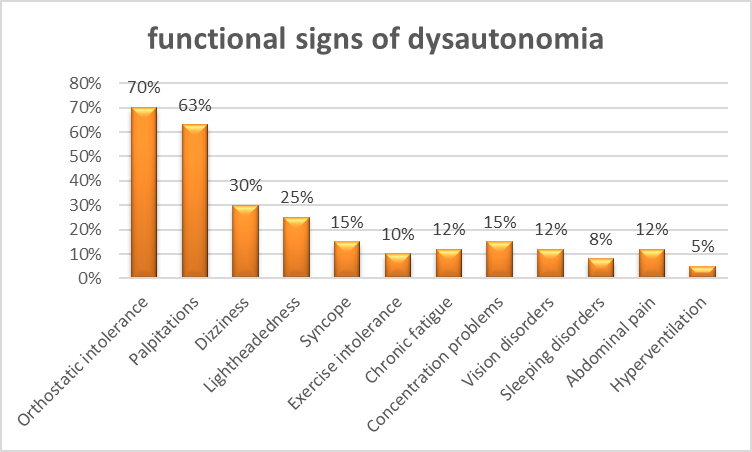
Functional signs of dysautonomia:
Orthostatic intolerance is the most frequently encountered symptom in POT syndrome, followed by palpitations and dizziness. The other symptoms are less seen in this dysautonomia.
Autonomic nervous system exploration results:
The population of POT syndrome studied had a special autonomic profile with, for most of our patients: normal vagal activity, central alpha and beta hyperactivity and peripheral alpha sympathetic hypo activity 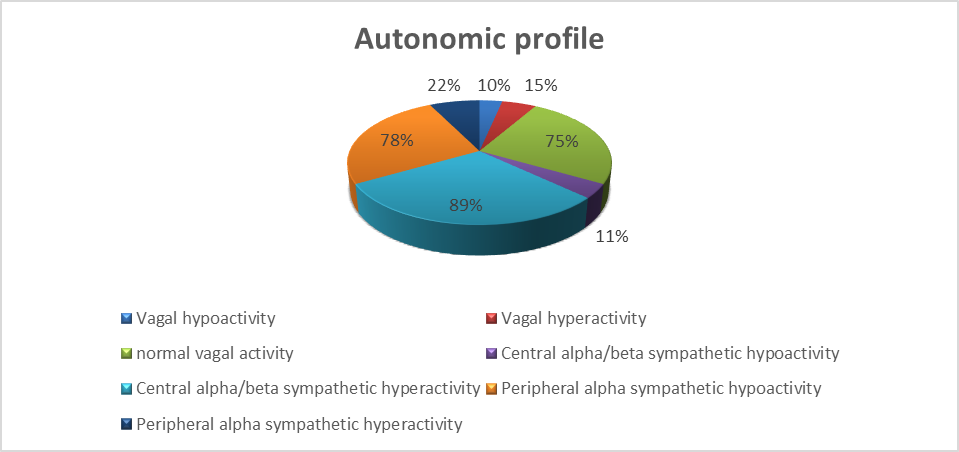 Therapeutic approaches:
Therapeutic approaches:
For our population the therapeutic approach was based on symptomatic treatment initially in particular; abundant drinks, lower limb muscle building, high salt diet, our results are that a check-up will be proposed in 6 months to see the evolution under treatment.
Over the past two decades, the number of publications on POT syndrome has consistently raised. However, it is uncertain whether this increase is due to the syndrome being recognized as a distinct clinical condition or because of the emergence of a new epidemic in developed nations. The heightened interest in POTS stems from its significant impact on patient's quality of life and the ongoing challenges in its diagnosis and treatment.(18)
Postural orthostatic tachycardia syndrome (POTS) is a relatively common but less well-known form of cardiovascular autonomic disorder. It is characterized by an excessive increase in heart rate upon standing, symptoms of orthostatic intolerance, and occasional episodes of syncope. The syndrome predominantly affects younger individuals, with women comprising about 80% of cases. Prevalence estimates in the U.S. range from 0.2% to 1.0%, translating to approximately 500,000 patients, while data from Europe remain largely unavailable.(19) (20) (21)
Schondorf and Low first introduced the term «POTS» in 1993 from the Mayo Clinic to describe sudden-onset idiopathic pan-dysautonomia, marked by hyperadrenergic circulatory symptoms and abnormal heart rate acceleration upon standing. However, similar conditions are documented earlier in medical history. (22)
In 1871, Da Costa published observations on abnormal postural tachycardia, typically occurring after intestinal infections, combat injuries, or excessive exertion among young soldiers during the American Civil War, which he termed "an irritable heart." In subsequent years, sporadic case reports described young individuals, often women, with characteristic postural tachycardia and reduced physical exercise capacity, though their long-term prognosis remained unclear.(23) (24)
Following their 1993 report, the Mayo Clinic group proposed diagnostic criteria for POTS, which included a heart rate increase of more than 30 beats per minute or a rate exceeding 120 beats per minute within the first 5 minutes of standing, along with symptoms of orthostatic intolerance. These criteria were later endorsed, with minor modifications, by major international neurological, autonomic, and cardiological societies.(25)
The diagnostic criteria for POTS are largely consistent across different consensus documents. However, many experts highlight that there may be overlap between POTS and other conditions, such as orthostatic hypotension, vasovagal syncope, panic disorders, psychogenic pseudo syncope, chronic fatigue syndrome, Ehlers-Danlos syndrome, and cardiac arrhythmias, which should be taken into account in more complex cases.(26)
The primary and pathognomonic feature of POTS is chronic orthostatic intolerance, which is often worsened by factors like high ambient temperature, inadequate fluid intake, dehydration, physical exertion, morning hours, or fever. However, patients with POTS typically present with additional symptoms as well. The most common symptoms during the initial presentation of POTS include dizziness, weakness, and rapid heartbeat, palpitations upon standing, headaches, fatigue, abdominal pain, and syncope. Two-thirds of patients report experiencing at least ten different symptoms, which can make diagnosis challenging for practitioners unfamiliar with the condition. A UK study found that patients waited an average of four years from the onset of symptoms to receive a correct diagnosis, with many initially suspected of having a psychiatric disorder.(27)
Cardiovascular symptoms in POTS are linked to an exaggerated and inadequate increase in heart rate upon standing, global postural hemodynamic instability, which may involve either a hypertensive or hypotensive tendency, cerebral hypoperfusion, venous pooling, and dysregulation of vascular tone in specific areas such as the head, coronary arteries, skin, and extremities. Additionally, around 30–50% of POTS patients experience fainting.(28) (29)
Non-cardiovascular symptoms in POTS are not directly associated with the observed hemodynamic abnormalities. The most significant non-cardiovascular features of POTS are general and include nonspecific physical deconditioning, reduced exercise capacity, fatigue, and weakness. The most affected non-cardiac areas are the head and the nervous and respiratory systems. The gastrointestinal and musculoskeletal systems are also commonly affected in POTS. Some symptoms result from impaired autonomic regulation of basic homeostatic functions, such as thermoregulation and peristalsis. The prevalence of various symptoms varies significantly, with some being more frequent and others less common.(30) (28) (29)
The heterogeneous symptomatology, early onset, and potential triggers in the patient’s history have led to various hypotheses about the syndrome’s origin. Initial clinical observations suggested that the illness often begins after an acute infection, typically viral, with a presentation similar to Guillain–Barré syndrome. This has drawn attention to the potential role of the immune system in POTS, though this theory remains debated and rarely confirmed. Nevertheless, several factors support this possibility. First, the higher prevalence in women and the association with prior viral infections, vaccinations, or trauma resemble features commonly seen in autoimmune diseases. Additionally, signs of immune dysfunction and positive autoimmune tests are frequently observed in POTS patients. For example, one in four POTS patients tests positive for antinuclear antibodies, and 20% have a history of autoimmune disorders like Hashimoto's thyroiditis, rheumatoid arthritis, or Sjögren’s syndrome, a rate higher than expected in the general population. (31) (32)
The symptoms of POTS, particularly tachycardia, may be triggered either by a direct effect on the sinus rate-controlling system (through adrenergic and muscarinic receptors) or via a compensatory response to peripheral vasodilation (involving adrenergic, angiotensin, and other potential vasoactive receptors). This intriguing hypothesis still requires validation in larger, more independent patient populations and well-selected control groups.(31)
Other suggested pathological mechanisms include disruptions in autonomic cardiovascular regulation, such as abnormally elevated sympathetic activity and excess circulating catecholamine, as well as peripheral sympathetic denervation leading to central hypovolemia. According to this theory, increased central sympathetic outflow could account for inappropriate sinus tachycardia, while venous pooling and reduced preload—resulting from peripheral sympathetic denervation—would lead to a compensatory increase in heart rate. Although these mechanisms may seem contradictory, if associated, they could produce the characteristic postural tachycardia. It remains uncertain whether this autonomic dysfunction is hereditary or acquired.(33) (34)
The diagnostic process for POTS should ideally be entrusted to a center or specialist with substantial experience in managing the condition. The gold standard for diagnosing POTS is the head-up tilt test, accompanied by non-invasive beat-to-beat hemodynamic monitoring. Additional tests may be conducted to assess the patient’s hemodynamic profile, distinguish between the 'hyper adrenergic' and 'neuropathic' forms, and evaluate symptom severity. In specialized autonomic centers—though not widely accessible—a comprehensive battery of autonomic tests can be performed to further classify dysfunctions affecting the entire autonomic nervous system, not just the cardiovascular branch. These tests can help both clinicians and patients gain a deeper understanding of the specific symptoms associated with POTS. They may be used to educate patients on non-pharmacological therapies to ease non-cardiovascular symptoms.(35)
The heterogeneity and wide range of symptoms associated with POTS present a significant challenge for both clinicians and patients. Additionally, the poorly understood pathophysiology of POTS makes it nearly impossible to directly treat the underlying cause of the condition. As a result, management typically focuses on alleviating symptoms rather than addressing the root of the disease. The long-term prognosis for POTS remains uncertain, but it is estimated that approximately 50% of patients experience spontaneous recovery within 1–3 years.(36)
The first step in the effective management of POTS is ensuring an accurate diagnosis. Patients should be thoroughly informed about the syndrome, both verbally and through dedicated resources such as printed materials, brochures, and other educational tools. This helps patients better understand their condition and the available management options. The core of effective POTS management lies in patient education, which includes avoiding orthostatic intolerance triggers and gaining a better understanding of POTS pathophysiology. Exercise training can be highly effective and showed to reduce symptoms related to POTS deconditioning. When symptoms are more severe, pharmacological treatment should be considered. (37) (38)
To summarize key non-pharmacological management strategies for POTS:
Currently, there are no Class I recommendations for the treatment of POTS. The only Class IIA recommendations are for exercise training to address chronic symptoms and acute saline infusions for decompensated POTS, both of which have been shown to affect plasma volume positively. Class IIB recommendations include increasing fluid and salt intake, as well as using medications like midodrine, beta-blockers, fludrocortisone, pyridostigmine, clonidine, and alpha-methyldopa. As a result, physicians and patients often face the challenge of deciding which medication to try, frequently relying on a trial-and-error approach, leading to frequent polypharmacy. Typically, clinicians test various drugs aimed at controlling heart rate, increasing peripheral vasoconstriction, and expanding intravascular volume. However, the overall effectiveness of pharmacological therapy remains limited, and many patients with severe symptoms continue to experience significant challenges even with the use of multiple medications.(37)
Postural orthostatic tachycardia syndrome (POTS) is a type of cardiovascular autonomic disorder characterized by orthostatic intolerance and an abnormal increase in heart rate upon standing. It is often accompanied by symptoms such as deconditioning, cognitive impairment, and various nonspecific complaints. POTS primarily affects young women of reproductive age. Although the exact cause is unknown, factors like autoimmunity, a hyperadrenergic state, chronic hypovolemia, and autonomic neuropathy are suggested as potential underlying mechanisms. While POTS is a chronic condition, some patients show improvement within a few years of onset.
Management of POTS focuses on educating patients and implementing non-pharmacological strategies to combat orthostatic intolerance. Medications control heart rate, enhance peripheral vasoconstriction and increase intravascular volume, though their efficacy is limited in more severe cases. Future research should aim to deepen the understanding of POTS pathophysiology and develop randomized controlled trials to identify treatments that are more effective.
This study is a single-center study, the sample size is small, and the follow-up time is short. Maybe there is a certain bias, and if we extended their follow-up and expanded the sample size, the benefit of cardiovascular events would be more obvious, and the long-term adverse side effects would be more persuasive.
No funding
The authors declare that they have no competing interests
Data is collected with respect of anonymity and confidentiality of the information provided after patient consent
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
